Autism spectrum
| Autism spectrum | |
|---|---|
| Other names: Autism spectrum disorder, autistic spectrum disorder, autistic spectral disorder,[1] autism spectrum condition, autistic spectrum condition[2] | |
 | |
| Repetitively stacking or lining up objects is associated with autism spectrum | |
| Specialty | Psychiatry, clinical psychology |
| Symptoms | Problems with communication, social interaction, restricted interests, repetitive behavior[3] |
| Complications | Employment problems, few relationships, suicide[4] |
| Usual onset | By age 2 years[3] |
| Duration | Long-term[5] |
| Causes | Uncertain[5] |
| Risk factors | Advanced parental age, exposure to valproate during pregnancy, low birth weight[3] |
| Diagnostic method | Based on symptoms[5] |
| Differential diagnosis | Intellectual disability, Rett syndrome, ADHD, selective mutism, childhood-onset schizophrenia[3] |
| Treatment | Behavioral therapy, medication[6][7] |
| Frequency | 1% of people (62.2 million 2015)[3][8] |
Autism spectrum a mental disorder with onset in childhood, that includes the prior diagnosis autism and Asperger syndrome.[3] Symptoms include long-term difficulties with communication, social interaction, restricted interests, and repetitive behavior.[3] Symptoms are typically recognized before two years of age.[3] Complications may include difficulties in performing daily tasks, creating and keeping relationships, maintaining a job, and suicide.[4]
While the cause is uncertain, it is beleived to involve a combination of genetic and enviromental factors.[5] Risk factors include having an older parent, a family history of autism, and certain genetic conditions.[5] It is estimated that between 65% and 90% of risk is due to genetics.[9] Diagnosis is based on symptoms.[5] In 2013, the DSM-5 replaced the previous subgroups of autistic disorder, Asperger syndrome, pervasive developmental disorder not otherwise specified (PDD-NOS), and childhood disintegrative disorder with the single term "autism spectrum disorder".[10][11]
While there is no cure treatment can improve outcomes.[12] Efforts are generally individualized and can include behavioural therapy and the teaching of coping skills.[5] These efforts often involve the parents and other family members.[5] Medications may be used to try to help improve some associated symptoms.[5] Evidence to support the use of medications, however, is not very strong.[7]
Autism spectrum is estimated to affect about 1% of people (62.2 million globally) as of 2015.[3][8] In the United States it is estimated to affect about 2.5% of children (about 1.5 million) as of 2016.[13] Males are diagnosed four times more often than females.[12] The term "spectrum" refers to the variation in the type and severity of symptoms.[11] Outcomes are variable, with some with mild symptoms function independently, while those with more severe symptoms requiring substantial support in their daily lives.[14][4]
Classification

Autism forms the core of the autism spectrum disorders. Asperger syndrome is closest to autism in signs and likely causes;[15] unlike autism, people with Asperger syndrome have no significant delay in language development or cognitive development, according to the older DSM-IV criteria.[16] PDD-NOS is diagnosed when the criteria are not met for a more specific disorder. Some sources also include Rett syndrome and childhood disintegrative disorder, which share several signs with autism but may have unrelated causes; other sources differentiate them from ASD, but group all of the above conditions into the pervasive developmental disorders.[15][17]
Autism, Asperger syndrome, and PDD-NOS are sometimes called the autistic disorders instead of ASD,[18] whereas autism itself is often called autistic disorder, childhood autism, or infantile autism.[19] Although the older term pervasive developmental disorder and the newer term autism spectrum disorder largely or entirely overlap,[17] the earlier was intended to describe a specific set of diagnostic labels, whereas the latter refers to a postulated spectrum disorder linking various conditions.[20] ASD is a subset of the broader autism phenotype (BAP), which describes individuals who may not have ASD but do have autistic-like traits, such as avoiding eye contact.[19]
A revision to autism spectrum disorder (ASD) was presented in the Diagnostic and Statistical Manual of Mental Disorders version 5 (DSM-5), released May 2013.[21] The new diagnosis encompasses previous diagnoses of autistic disorder, Asperger syndrome, childhood disintegrative disorder, and PDD-NOS. Compared with the DSM-IV diagnosis of autistic disorder, the DSM-5 diagnosis of ASD no longer includes communication as a separate criterion, and has merged social interaction and communication into one category.[22] Slightly different diagnostic definitions are used in other countries. For example, the ICD-10 is the most commonly-used diagnostic manual in the UK and European Union.[23] Rather than categorizing these diagnoses, the DSM-5 has adopted a dimensional approach to diagnosing disorders that fall underneath the autism spectrum umbrella. Some have proposed that individuals on the autism spectrum may be better represented as a single diagnostic category. Within this category, the DSM-5 has proposed a framework of differentiating each individual by dimensions of severity, as well as associated features (i.e., known genetic disorders, and intellectual disability).
Another change to the DSM includes collapsing social and communication deficits into one domain. Thus, an individual with an ASD diagnosis will be described in terms of severity of social communication symptoms, severity of fixated or restricted behaviors or interests, hyper- or hyposensitivity to sensory stimuli, and associated features. The restricting of onset age has also been loosened from 3 years of age to "early developmental period", with a note that symptoms may manifest later when social demands exceed capabilities.[24]
Signs and symptoms
Autism spectrum disorder (ASD) is characterized by persistent challenges with social communication and social interaction, and by the presence of restricted, repetitive patterns of behavior, interests, or activities.[25] These symptoms begin in early childhood, and can impact function.[26] There is also a unique disorder called savant syndrome that can co-occur with autism.[27] As many as one in 10 children with autism and savant syndrome can have outstanding skills in music, art, and mathematics.[27] Self-injurious behavior (SIB) is more common and has been found to correlate with intellectual disability.[28][29] Approximately 50% of those with ASD take part in some type of SIB (head-banging, self-biting).[30]
Other characteristics of ASD include restricted and repetitive behaviors (RRBs). These include a range of gestures and behaviors as defined in the Diagnostic and Statistic Manual for Mental Disorders.[31]
Asperger syndrome was distinguished from autism in the DSM-IV by the lack of delay or deviance in early language development.[32] Additionally, individuals diagnosed with Asperger syndrome did not have significant cognitive delays.[33] PDD-NOS was considered "subthreshold autism" and "atypical autism" because it was often characterized by milder symptoms of autism or symptoms in only one domain (such as social difficulties).[34] The DSM-5 eliminated the four separate diagnoses: Asperger Syndrome, Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS), Childhood Disintegrative Disorder, and Autistic Disorder and combined them under the diagnosis of Autism Spectrum Disorder.[26]
Developmental course
Most parents report that the onset of autism symptoms occur within the first year of life.[35][36] There are two possible developmental courses of autism spectrum disorder. One course of development is more gradual in nature, in which parents report concerns in development over the first two years of life and diagnosis is made around 3–4 years of age. Some of the early signs of ASDs in this course include decreased looking at faces, failure to turn when name is called, failure to show interests by showing or pointing, and delayed imaginative play.[37]
A second course of development is characterized by normal or near-normal development in the first 15 months to 3 years before onset of regression or loss of skills. Regression may occur in a variety of domains, including communication, social, cognitive, and self-help skills; however, the most common regression is loss of language.[38][39] Childhood disintegrative disorder, a DSM-IV diagnosis now included under ASD in DSM-V, is characterized by regression after normal development in the first 3 to 4 years of life.[40]
There continues to be a debate over the differential outcomes based on these two developmental courses. Some studies suggest that regression is associated with poorer outcomes and others report no differences between those with early gradual onset and those who experience a regression period.[41] While there is conflicting evidence surrounding language outcomes in ASD, some studies have shown that cognitive and language abilities at age 2 1⁄2 may help predict language proficiency and production after age 5.[42] Overall, the literature stresses the importance of early intervention in achieving positive longitudinal outcomes.[43]
Social skills
Impairments in social skills present many challenges for individuals with ASD. Deficits in social skills may lead to problems with friendships, romantic relationships, daily living, and vocational success.[44] One study that examined the outcomes of adults with ASD found that, compared to the general population, those with ASD were less likely to be married, but it is unclear whether this outcome was due to deficits in social skills or intellectual impairment.[45]
Prior to 2013, deficits in social function and communication were considered two separate symptoms of autism.[46] The current criteria for Autism diagnosis require individuals to have deficits in three social skills: social-emotional reciprocity, nonverbal communication, and developing and sustaining relationships.[3]
Some of the symptoms related to social reciprocity include:
- Lack of mutual sharing of interests: many children with autism prefer not to play or interact with others.
- Lack of awareness or understanding of other people's thoughts or feelings: a child may get too close to peers without noticing that this makes them uncomfortable.
- Atypical behaviors for attention: a child may push a peer to gain attention before starting a conversation.[47]
People with autism spectrum usually display atypical nonverbal behaviors:
- Poor eye contact: a child with autism may fail to make eye contact when called by name, or they may avoid making eye contact with an observer. Aversion of gaze can also be seen in anxiety disorders, however poor eye contact in autistic children is not due to shyness or anxiety; rather, it is overall diminished in quantity.
- Facial expressions: they often don't know how to recognize emotions from others' facial expressions, or they may not respond with the appropriate facial expressions.
- Unusual speech: at least half of children with autism speak in a flat, monotone voice or they may not recognize the need to control the volume of their voice in different social settings. For example, they may speak loudly in libraries or movie theaters.[48]
Communication skills
Communication deficits are due to problems with social-emotional skills like joint attention and social reciprocity. Difficulties with nonverbal communication skills such as poor eye contact, and impaired use of proper facial expressions and gestures are common.[49][50] Some of the linguistic behaviors in individuals with autism include repetitive or rigid language, and restricted interests in conversation. For example, a child might repeat words or insist on always talking about the same subject.[47] ASD can present with impairments in pragmatic communication skills, such as difficulty initiating a conversation or failure to consider the interests of the listener to sustain a conversation.[47] Language impairment is also common in children with autism, but it is not necessary for the diagnosis.[47] Many children with ASD develop language skills at an uneven pace where they easily acquire some aspects of communication, while never fully developing others.[50] In some cases, individuals remain completely nonverbal throughout their lives, although the accompanying levels of literacy and nonverbal communication skills vary.
They may not pick up on body language or social cues such as eye contact and facial expressions if they provide more information than the person can process at that time. Similarly, they have trouble recognizing subtle expressions of emotion and identifying what various emotions mean for the conversation. They struggle with understanding the context and subtext of conversational or printed situations, and have trouble forming resulting conclusions about the content. This also results in a lack of social awareness and atypical language expression.[51] How emotional processing and facial expressions differ between those on the autism spectrum and others is not clear, but emotions are processed differently between different partners.[52]
It is also common for individuals with ASD to communicate strong interest in a specific topic, speaking in lesson-like monologues about their passion instead of enabling reciprocal communication with whomever they are speaking to.[50] What looks like self-involvement or indifference toward others stems from a struggle to recognize or remember that other people have their own personalities, perspectives, and interests.[51] The ability to be focused in on one topic in communication is known as monotropism, and can be compared to "tunnel vision" in the mind for those individuals with ASD.[53] Language expression by those on the autism spectrum is often characterized by repetitive and rigid language. Often children with ASD repeat certain words, numbers, or phrases during an interaction, words unrelated to the topic of conversation. They can also exhibit a condition called echolalia in which they respond to a question by repeating the inquiry instead of answering.[50]
Behavioral characteristics
Autism spectrum disorders include a wide variety of characteristics. Some of these include behavioral characteristics which widely range from slow development of social and learning skills to difficulties creating connections with other people. They may develop these difficulties of creating connections due to anxiety or depression, which people with autism are more likely to experience, and as a result isolate themselves.[54] Other behavioral characteristics include abnormal responses to sensations including sights, sounds, touch, and smell, and problems keeping a consistent speech rhythm. The latter problem influences an individual's social skills, leading to potential problems in how they are understood by communication partners. Behavioral characteristics displayed by those with autism spectrum disorder typically influence development, language, and social competence. Behavioral characteristics of those with autism spectrum disorder can be observed as perceptual disturbances, disturbances of development rate, relating, speech and language, and motility.[55]
The second core symptom of Autism spectrum is a pattern of restricted and repetitive behaviors, activities, and interests. In order to be diagnosed with ASD, a child must have at least two of the following behaviors:[3][25]
- Stereotyped behaviors– Most children with autism perform repetitive behaviors such as rocking, hand flapping, finger flicking, head banging, or repeating phrases or sounds.[47] These behaviors may occur constantly or only when the child gets stressed, anxious or upset.
- Resistance to change– Children with autism spectrum also tend to have routines and rituals that they must follow, like eating certain foods in a specific order, or taking the same path to school every day.[47] The child may have a meltdown if there is any change or disruption to his routine.
- Restricted interests– Children may become excessively interested in a particular thing or topic, and devote all their attention to it. For example, young children might completely focus on things that spin and ignore everything else. Older children might try to learn everything about a single topic, such as the weather or sports, and talk about it constantly.[47]
- Sensory processing disorder– Many people with Autism have difficulty processing complex combinations of emotional and sensory stimuli. Their inability to process this information in a timely manner produces an information pile up which will trigger a stress reaction. They must be able to escape the environment causing this information pile up or their stress reaction may escalate to a severe anxiety reaction or panic attack. This will ultimately result in an autistic meltdown.
- Oversensitivity– Many people with autism are overly sensitive to loud sounds, bright lights, strong smells, or being touched.
Self-injury
Self-injurious behaviors (SIB) are common in ASD and include head-banging, self-cutting, self-biting, and hair-pulling.[30] These behaviors can result in serious injury or death.[30] Following are theories about the cause of self-injurious behavior in autistic individuals:[29]
- Frequency and/or continuation of self-injurious behavior can be influenced by environmental factors e.g. reward in return for halting self-injurious behavior. However this theory is not applicable to younger children with autism. There is some evidence that frequency of self-injurious behavior can be reduced by removing or modifying environmental factors that reinforce this behavior.
- Higher rates of self-injury are also noted in socially isolated individuals with autism
- Self-injury could be a response to modulate pain perception when chronic pain or other health problems that cause pain are present
- An abnormal basal ganglia connectivity may predispose to self-injurious behavior
Causes
While specific causes of autism spectrum disorders have yet to be found, many risk factors identified in the research literature may contribute to their development. These risk factors include genetics, prenatal and perinatal factors, neuroanatomical abnormalities, and environmental factors. It is possible to identify general risk factors, but much more difficult to pinpoint specific factors. Given the current state of knowledge, prediction can only be of a global nature and therefore requires the use of general markers.[56]
Genetics
As of 2018, it appeared that somewhere between 74% and 93% of ASD risk is heritable.[25] After an older child is diagnosed with ASD, 7–20% of subsequent children are likely to be as well.[25] If parents have a child with ASD they have a 2% to 8% chance of having a second child with ASD. If the child with ASD is an identical twin the other will be affected 36 to 95 percent of the time. If they are fraternal twins the other will only be affected up to 31 percent of the time.[57]
As of 2018, understanding of genetic risk factors had shifted from a focus on a few alleles to an understanding that genetic involvement in ASD is probably diffuse, depending on a large number of variants, some of which are common and have a small effect, and some of which are rare and have a large effect. The most common gene disrupted with large effect rare variants appeared to be CHD8, but less than 0.5% of people with ASD have such a mutation. Some ASD is associated with clearly genetic conditions, like fragile X syndrome; however only around 2% of people with ASD have fragile X.[25]
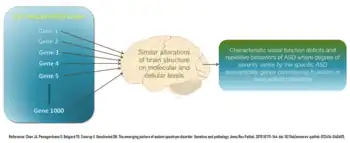
Current research suggests that genes that increase susceptibility to ASD are ones that control protein synthesis in neuronal cells in response to cell needs, activity and adhesion of neuronal cells, synapse formation and remodeling, and excitatory to inhibitory neurotransmitter balance. Therefore despite up to 1000 different genes thought to contribute to increased risk of ASD, all of them eventually affect normal neural development and connectivity between different functional areas of the brain in a similar manner that is characteristic of an ASD brain. Some of these genes are knows to modulate production of the GABA neurotransmitter which is the main inhibitory neurotransmitter in the nervous system. These GABA-related genes are underexpressed in an ASD brain. On the other hand, genes controlling expression of glial and immune cells in the brain e.g. astrocytes and microglia, respectively, are overexpressed which correlates with increased number of glial and immune cells found in postmortem ASD brains. Some genes under investigation in ASD pathophysiology are those that affect the mTOR signaling pathway which supports cell growth and survival.[58]
All these genetic variants contribute to the development of the autistic spectrum, however, it can not be guaranteed that they are determinants for the development.[59]
Early life
Several prenatal and perinatal complications have been reported as possible risk factors for autism. These risk factors include maternal gestational diabetes, maternal and paternal age over 30, bleeding after first trimester, use of prescription medication (e.g. valproate) during pregnancy, and meconium in the amniotic fluid. While research is not conclusive on the relation of these factors to autism, each of these factors has been identified more frequently in children with autism, compared to their siblings who do not have autism, and other typically developing youth.[60] While it is unclear if any single factors during the prenatal phase affect the risk of autism,[61] complications during pregnancy may be a risk.[61]
Low vitamin D levels in early development has been hypothesized as a risk factor for autism.[62]
Disproven vaccine hypothesis
In 1998 Andrew Wakefield led a fraudulent study that suggested that the MMR vaccine may cause autism.[63][64][65][66][67] This conjecture suggested that autism results from brain damage caused either by the MMR vaccine itself, or by thimerosal, a vaccine preservative.[68] No convincing scientific evidence supports these claims, and further evidence continues to refute them, including the observation that the rate of autism continues to climb despite elimination of thimerosal from routine childhood vaccines.[69] A 2014 meta-analysis examined ten major studies on autism and vaccines involving 1.25 million children worldwide; it concluded that neither the MMR vaccine, which has never contained thimerosal,[70] nor the vaccine components thimerosal or mercury, lead to the development of ASDs.[71]
Pathophysiology
In general, neuroanatomical studies support the concept that autism may involve a combination of brain enlargement in some areas and reduction in others.[72] These studies suggest that autism may be caused by abnormal neuronal growth and pruning during the early stages of prenatal and postnatal brain development, leaving some areas of the brain with too many neurons and other areas with too few neurons.[73] Some research has reported an overall brain enlargement in autism, while others suggest abnormalities in several areas of the brain, including the frontal lobe, the mirror neuron system, the limbic system, the temporal lobe, and the corpus callosum.[74][75]
In functional neuroimaging studies, when performing theory of mind and facial emotion response tasks, the median person on the autism spectrum exhibits less activation in the primary and secondary somatosensory cortices of the brain than the median member of a properly sampled control population. This finding coincides with reports demonstrating abnormal patterns of cortical thickness and grey matter volume in those regions of autistic persons' brains.[76]
Brain connectivity
Brains of autistic individuals have been observed to have abnormal connectivity and the degree of these abnormalities directly correlates with the severity of autism. Following are some observed abnormal connectivity patterns in autistic individuals:[77][58]
- Decreased connectivity between different specialized regions of the brain (e.g. lower neuron density in corpus callosum) and relative overconnectivity within specialized regions of the brain by adulthood. Connectivity between different regions of the brain ('long-range' connectivity) is important for integration and global processing of information and comparing incoming sensory information with the existing model of the world within the brain. Connections within each specialized regions ('short-range' connections) are important for processing individual details and modifying the existing model of the world within the brain to more closely reflect incoming sensory information. In infancy, children at high risk for autism that were later diagnosed with autism were observed to have abnormally high long-range connectivity which then decreased through childhood to eventual long-range underconnectivity by adulthood.[77]
- Abnormal preferential processing of information by the left hemisphere of the brain vs. preferential processing of information by right hemisphere in neurotypical individuals. The left hemisphere is associated with processing information related to details whereas the right hemisphere is associated with processing information in a more global and integrated sense that is essential for pattern recognition. For example, visual information like face recognition is normally processed by the right hemisphere which tends to integrate all information from an incoming sensory signal, whereas an ASD brain preferentially processes visual information in the left hemisphere where information tends to be processed for local details of the face rather than the overall configuration of the face. This left lateralization negatively impacts both facial recognition and spatial skills.[77]
- Increased functional connectivity within the left hemisphere which directly correlates with severity of autism. This observation also supports preferential processing of details of individual components of sensory information over global processing of sensory information in an ASD brain.[77]
- Prominent abnormal connectivity in the frontal and occipital regions. In autistic individuals low connectivity in the frontal cortex was observed from infancy through adulthood. This is in contrast to long-range connectivity which is high in infancy and low in adulthood in ASD.[77] Abnormal neural organization is also observed in the Broca's area which is important for speech production.[58]
Neuropathology
Listed below are some characteristic findings in ASD brains on molecular and cellular levels regardless of the specific genetic variation or mutation contributing to autism in a particular individual:
- Limbic system with smaller neurons that are more densely packed together. Given that the limbic system is the main center of emotions and memory in the human brain, this observation may explain social impairment in ASD.[58]
- Fewer and smaller Purkinje neurons in the cerebellum. New research suggest a role of the cerebellum in emotional processing and language.[58]
- Increased number of astrocytes and microglia in the cerebral cortex. These cells provide metabolic and functional support to neurons and act as immune cells in the nervous system, respectively.[58]
- Increased brain size in early childhood causing macrocephaly in 15–20% of ASD individuals. The brain size however normalizes by mid-childhood. This variation in brain size in not uniform in the ASD brain with some parts like the frontal and temporal lobes being larger, some like the parietal and occipital lobes being normal sized, and some like cerebellar vermis, corpus callosum, and basal ganglia being smaller than neurotypical individuals.[58]
- Cell-adhesion molecules (CAMs) that are essential to formation and maintenance of connections between neurons, neuroligins found on postsynaptic neurons that bind presynaptic CAMs, and proteins that anchor CAMs to neurons are all found to be mutated in ASD.[58]
Gut-immune-brain axis
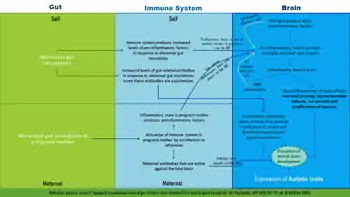
Up to 70% of autistic individuals have GI related problems like reflux, diarrhea, constipation, inflammatory bowel disease, and food allergies. The severity of GI symptoms is directly proportional to the severity of autism. It has also been shown that the makeup of gut bacteria in ASD patients is different than that of neurotypical individuals. This has raised the question of influence of gut bacteria on ASD development via inducing an inflammatory state.[78]
Listed below are some research findings on the influence of gut bacteria and abnormal immune responses on brain development:[78]
- Some studies on rodents have shown gut bacteria influencing emotional functions and neurotransmitter balance in the brain, both of which are impacted in ASD.[58]
- The immune system is thought to be the intermediary that modulates the influence of gut bacteria on the brain. Some ASD individuals have a dysfunctional immune system with higher numbers of some types of immune cells, biochemical messengers and modulators, and autoimmune antibodies. Increased inflammatory biomarkers correlate with increased severity of ASD symptoms and there is evidence to support a state of chronic brain inflammation in ASD.[78]
- More pronounced inflammatory responses to bacteria were found in ASD individuals with an abnormal gut microbiota. Additionally IgA antibodies that are central to gut immunity were also found in elevated levels in ASD populations. Some of these antibodies may also attack proteins that support myelination of the brain, a process that is important for robust transmission of neural signal in many nerves.[78]
- Activation of the maternal immune system during pregnancy (by gut bacteria, bacterial toxins, an infection, or non-infectious causes) and gut bacteria in the mother that induce increased levels of Th17, a proinflammatory immune cell, have been associated with an increased risk of autism. Some maternal IgG antibodies that cross the placenta to provide passive immunity to the fetus can also attack the fetal brain. One study found that 12% of mothers of autistic children have IgG that are active against the fetal brain.[78]
- Inflammation within the gut itself does not directly affect brain development. Rather it is the inflammation within the brain promoted by inflammatory responses to harmful gut microbiome that impact brain development.[78]
- Proinflammatory biomessengers IFN-γ, IFN-α, TNF-α, IL-6 and IL-17 have been shown to promote autistic behaviors in animal models. Giving anti-IL-6 and anti-IL-17 along with IL-6 and IL-17, respectively, have been shown to negate this effect in the same animal models.[78]
- Some gut proteins and microbial products can cross the blood-brain barrier (BBB) and activate mast cells in the brain. Mast cells release proinflammatory factors and histamine which further increase BBB permeability and help set up a cycle of chronic inflammation.[78]
Mirror neuron system
The mirror neuron system (MNS) consists of a network of brain areas that have been associated with empathy processes in humans.[79] In humans, the MNS has been identified in the inferior frontal gyrus (IFG) and the inferior parietal lobule (IPL) and is thought to be activated during imitation or observation of behaviors.[80] The connection between mirror neuron dysfunction and autism is tentative, and it remains to be seen how mirror neurons may be related to many of the important characteristics of autism.[81][82]
"Social brain" interconnectivity
A number of discrete brain regions and networks among regions that are involved in dealing with other people have been discussed together under the rubric of the "social brain". As of 2012, there is a consensus that autism spectrum is likely related to problems with interconnectivity among these regions and networks, rather than problems with any specific region or network.[83]
Temporal lobe
Functions of the temporal lobe are related to many of the deficits observed in individuals with ASDs, such as receptive language, social cognition, joint attention, action observation, and empathy. The temporal lobe also contains the superior temporal sulcus (STS) and the fusiform face area (FFA), which may mediate facial processing. It has been argued that dysfunction in the STS underlies the social deficits that characterize autism. Compared to typically developing individuals, one fMRI study found that individuals with high-functioning autism had reduced activity in the FFA when viewing pictures of faces.[84]
Mitochondria
ASD could be linked to mitochondrial disease (MD), a basic cellular abnormality with the potential to cause disturbances in a wide range of body systems.[85] A 2012 meta-analysis study, as well as other population studies have shown that approximately 5% of children with ASD meet the criteria for classical MD.[86] It is unclear why the MD occurs considering that only 23% of children with both ASD and MD present with mitochondrial DNA (mtDNA) abnormalities.[86]
Serotonin
Serotonin is a major neurotransmitter in the nervous system and contributes to formation of new neurons (neurogenesis), formation of new connections between neurons (synaptogenesis), remodeling of synapses, and survival and migration of neurons, processes that are necessary for a developing brain and some also necessary for learning in the adult brain. 45% of ASD individuals have been found to have increased blood serotonin levels.[58] It has been hypothesized that increased activity of serotonin in the developing brain may facilitate the onset of autism spectrum disorder, with an association found in six out of eight studies between the use of selective serotonin reuptake inhibitors (SSRIs) by the pregnant mother and the development of ASD in the child exposed to SSRI in the antenatal environment. The study could not definitively conclude SSRIs caused the increased risk for ASDs due to the biases found in those studies, and the authors called for more definitive, better conducted studies.[87] Confounding by indication has since then been shown to be likely.[88] However, it is also hypothesized that SSRIs may help reduce symptoms of ASD and even positively affect brain development in some ASD patients.[58]
Diagnosis
ASD can be detected as early as 18 months or even younger in some cases.[89] A reliable diagnosis can usually be made by the age of two years, however, because of delays in seeking and administering assessments, diagnoses often occur much later.[90] The diverse expressions of ASD behavioral and observational symptoms and absence of one specific genetic or molecular marker for the disease pose diagnostic challenges to clinicians who use assessment methods based on symptoms alone. Individuals with an ASD may present at various times of development (e.g., toddler, child, or adolescent), and symptom expression may vary over the course of development.[91] Furthermore, clinicians who use those methods must differentiate among pervasive developmental disorders, and may also consider similar conditions, including intellectual disability not associated with a pervasive developmental disorder, specific language disorders, ADHD, anxiety, and psychotic disorders.[92] Ideally the diagnosis of ASD should be given by a team of professionals from different disciplines (e.g. child psychiatrists, child neurologists, psychologists) and only after the child has been observed in many different settings.[93]
Considering the unique challenges in diagnosing ASD using behavioral and observational assessment, specific practice parameters for its assessment were published by the American Academy of Neurology in the year 2000,[94] the American Academy of Child and Adolescent Psychiatry in 1999,[91] and a consensus panel with representation from various professional societies in 1999.[95] The practice parameters outlined by these societies include an initial screening of children by general practitioners (i.e., "Level 1 screening") and for children who fail the initial screening, a comprehensive diagnostic assessment by experienced clinicians (i.e. "Level 2 evaluation"). Furthermore, it has been suggested that assessments of children with suspected ASD be evaluated within a developmental framework, include multiple informants (e.g., parents and teachers) from diverse contexts (e.g., home and school), and employ a multidisciplinary team of professionals (e.g., clinical psychologists, neuropsychologists, and psychiatrists).[96]
As of 2019, psychologists would wait until a child showed initial evidence of ASD tendencies, then administer various psychological assessment tools to assess for ASD.[96] Among these measurements, the Autism Diagnostic Interview-Revised (ADI-R) and the Autism Diagnostic Observation Schedule (ADOS) are considered the "gold standards" for assessing autistic children.[97][98] The ADI-R is a semi-structured parent interview that probes for symptoms of autism by evaluating a child's current behavior and developmental history. The ADOS is a semistructured interactive evaluation of ASD symptoms that is used to measure social and communication abilities by eliciting several opportunities (or "presses") for spontaneous behaviors (e.g., eye contact) in standardized context. Various other questionnaires (e.g., The Childhood Autism Rating Scale, Autism Treatment Evaluation Checklist) and tests of cognitive functioning (e.g., The Peabody Picture Vocabulary Test) are typically included in an ASD assessment battery.
Screening
Screening recommendations for autism in children younger than 3 years are:[99]
- US Preventive Services Task Force (USPSTF) does not recommend universal screen of young children for autism due to poor evidence of benefits of this screening when parents and clinicians have no concerns about ASD. The major concern is a false-positive diagnosis that would burden a family with very time consuming and financially demanding treatment interventions when it is not truly required. USPSTF also did not find any robust studies showing effectiveness of behavioral therapies in reducing ASD symptom severity[99]
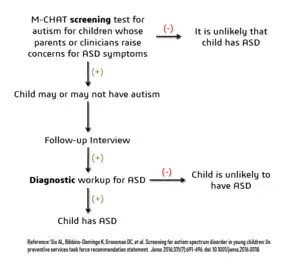
- American Academy of Pediatrics recommends ASD screening of all children between the ages if 18 and 24 months.[99] The AAP also recommends that children who screen positive for ASD be referred to ASD treatment services without waiting for a comprehensive diagnostic workup.[100]
- The American Academy of Family Physicians did not find sufficient evidence of benefit of universal early screening for ASD[99]
- The American Academy of Neurology and Child Neurology Society recommends general routine screening for delayed or abnormal development in children followed by screening for ASD only if indicated by the general developmental screening[99]
- Thee American Academy of Child and Adolescent Psychiatry recommend routinely screening autism symptoms in young children[99]
- The UK National Screening Committee does not recommend universal ASD screening in young children. Their main concerns includes higher chances of misdiagnosis at younger ages and lack of evidence of effectiveness of early interventions[99]
Misdiagnosis
There is a concern about significant levels of misdiagnosis of autism in neurodevelopmentally normal children. This is because 18–37% of children diagnosed with ASD eventually lose their diagnosis and this high rate of lost diagnosis cannot be accounted for by successful ASD treatment alone. The common reasons parents understood as the cause of lost ASD diagnosis were new information about child (73.5%), diagnosis given so child could receive ASD treatment services (24.2%) to treat another developmental disorder, ASD treatment success (21%), and incorrect diagnosis (1.9%).[100]
Many of the children who were later found not to meet ASD diagnosis criteria then received diagnosis for another developmental disorder like ADHD (most common), sensory disorders, anxiety, personality disorder, or learning disability.[100] Neurodevelopment and psychiatric disorders that are commonly misdiagnosed as ASD include specific language impairment, social communication disorder, anxiety disorder, reactive attachment disorder, cognitive impairment, visual impairment, hearing impairment and normal behavioral variations. Some normal behavioral variations that resemble autistic traits are repetitive behaviors, sensitivity to change in daily routines, focused interests, and toe-walking. These are considered normal behavioral variations when they do not cause impaired function. Boys are more likely to exhibit repetitive behaviors especially when excited, tired, bored, or stressed. Some ways of distinguishing normal behavioral variations from abnormal behaviors are the ability of the child to suppress these behaviors and the absence of these behaviors during sleep.[93]
Listed below are some risk factors for ASD misdiagnosis:
- Children diagnosed with PDD-NOS or a mild form of ASD which may be harder to distinguish from other developmental delays[100]
- Children diagnosed with ASD whose parents had no concerns about abnormal development in their child[100]
- Initial ASD diagnosis given by generalists (e.g. pediatricians, family physicians etc.), mental health providers, and schools rather than specialists in child neurodevelopmental disorders e.g. child psychiatrists or child neurologists[100]
Prognosis
Few children who are correctly diagnosed with ASD are thought to lose this diagnosis due to treatment or outgrowing their symptoms. Children with poor treatment outcomes also tend to be ones that had moderate to severe forms of ASD, whereas children who appear to have responded to treatment are the ones with milder forms of ASD.[100]
Comorbidity
Autism spectrum disorders tend to be highly comorbid with other disorders. Comorbidity may increase with age and may worsen the course of youth with ASDs and make intervention/treatment more difficult. Distinguishing between ASDs and other diagnoses can be challenging, because the traits of ASDs often overlap with symptoms of other disorders, and the characteristics of ASDs make traditional diagnostic procedures difficult.[101][102]
- The most common medical condition occurring in individuals with autism spectrum disorders is seizure disorder or epilepsy, which occurs in 11–39% of individuals with ASD.[103]
- Tuberous sclerosis, an autosomal dominant genetic condition in which non-malignant tumors grow in the brain and on other vital organs, is present in 1–4% of individuals with ASDs.[104]
- Intellectual disabilities are some of the most common comorbid disorders with ASDs. Recent estimates suggest that 40–69% of individuals with ASD have some degree of an intellectual disability,[41] more likely to be severe for females. A number of genetic syndromes causing intellectual disability may also be comorbid with ASD, including fragile X, Down, Prader-Willi, Angelman, Williams syndrome[105] and SYNGAP1-related intellectual disability.[106][107]
- Learning disabilities are also highly comorbid in individuals with an ASD. Approximately 25–75% of individuals with an ASD also have some degree of a learning disability.[108]
- Various anxiety disorders tend to co-occur with autism spectrum disorders, with overall comorbidity rates of 7–84%.[41] Rates of comorbid depression in individuals with an ASD range from 4–58%.[109] The relationship between ASD and schizophrenia remains a controversial subject under continued investigation, and recent meta-analyses have examined genetic, environmental, infectious, and immune risk factors that may be shared between the two conditions.[110][111][112]
- Deficits in ASD are often linked to behavior problems, such as difficulties following directions, being cooperative, and doing things on other people's terms.[113] Symptoms similar to those of attention deficit hyperactivity disorder (ADHD) can be part of an ASD diagnosis.[114]
- Sensory processing disorder is also comorbid with ASD, with comorbidity rates of 42–88%.[115]
- Starting in adolescence, some people with Asperger syndrome (26% in one sample)[116] fall under the criteria for the similar condition schizoid personality disorder, which is characterised by a lack of interest in social relationships, a tendency towards a solitary or sheltered lifestyle, secretiveness, emotional coldness, detachment and apathy.[116][117][118] Asperger syndrome was traditionally called "schizoid disorder of childhood".
Management
There is no known cure for autism, although those with Asperger syndrome and those who have autism and require little-to-no support are more likely to experience a lessening of symptoms over time.[119][120][121] Several interventions can help children with autism.[12] The main goals of treatment are to lessen associated deficits and family distress, and to increase quality of life and functional independence. In general, higher IQs are correlated with greater responsiveness to treatment and improved treatment outcomes.[122][123] Although evidence-based interventions for autistic children vary in their methods, many adopt a psychoeducational approach to enhancing cognitive, communication, and social skills while minimizing problem behaviors. It has been argued that no single treatment is best and treatment is typically tailored to the child's needs.[124]
Non-medication
Intensive, sustained special education or remedial education programs and behavior therapy early in life can help children acquire self-care, social, and job skills. Available approaches include applied behavior analysis, developmental models, structured teaching, speech and language therapy, social skills therapy, and occupational therapy.[124] Among these approaches, interventions either treat autistic features comprehensively, or focus treatment on a specific area of deficit.[123] Generally, when educating those with autism, specific tactics may be used to effectively relay information to these individuals. Using as much social interaction as possible is key in targeting the inhibition autistic individuals experience concerning person-to-person contact. Additionally, research has shown that employing semantic groupings, which involves assigning words to typical conceptual categories, can be beneficial in fostering learning.[125]
There has been increasing attention to the development of evidence-based interventions for young children with ASD. Two theoretical frameworks outlined for early childhood intervention include applied behavioral analysis (ABA) and the developmental social-pragmatic model (DSP).[123] Although ABA therapy has a strong evidence base, particularly in regard to early intensive home-based therapy, ABA's effectiveness may be limited by diagnostic severity and IQ of the person affected by ASD.[126] The Journal of Clinical Child and Adolescent Psychology has deemed two early childhood interventions as "well-established": individual comprehensive ABA, and focused teacher-implemented ABA combined with DSP.[123]
Another evidence-based intervention that has demonstrated efficacy is a parent training model, which teaches parents how to implement various ABA and DSP techniques themselves.[123] Various DSP programs have been developed to explicitly deliver intervention systems through at-home parent implementation.
A multitude of unresearched alternative therapies have also been implemented. Many have resulted in harm to autistic people and should not be employed unless proven to be safe.[124] However, a recent systematic review on adults with autism has provided emerging evidence for decreasing stress, anxiety, ruminating thoughts, anger, and aggression through mindfulness-based interventions for improving mental health.[127]
In October 2015, the American Academy of Pediatrics (AAP) proposed new evidence-based recommendations for early interventions in ASD for children under 3.[128] These recommendations emphasize early involvement with both developmental and behavioral methods, support by and for parents and caregivers, and a focus on both the core and associated symptoms of ASD.[128] However, a Cochrane review found no evidence that early intensive behavioral intervention (EIBI) is effective in reducing behavioral problems associated with autism in most children with ASD but did help improve IQ and language skills. The Cochrane review did acknowledge that this may be due to the low quality of studies currently available on EIBI and therefore providers should recommend EIBI based on their clinical judgement and the family's preferences. No adverse effects of EIBI treatment were found.[129] Studies on pet therapy have shown positive effects.[130]
Generally speaking, treatment of ASD focuses on behavioral and educational interventions to target its two core symptoms: social communication deficits and restricted, repetitive behaviors.[131] If symptoms continue after behavioral strategies have been implemented, some medications can be recommended to target specific symptoms or co-existing problems such as restricted and repetitive behaviors (RRBs), anxiety, depression, hyperactivity/inattention and sleep disturbance.[131] Melatonin for example can be used for sleep problems.[132]
While there are a number of parent-mediated behavioral therapies to target social communication deficits in children with autism, there is uncertainty regarding the efficacy of interventions to treat RRBs.[133][134]
Medication
There is some emerging data that show positive effects of risperidone on restricted and repetitive behaviors, but due to the small sample size of these studies and the concerns about its side effects, antipsychotics are not recommended as primary treatment of RRBs.[135]
Epidemiology
While rates of autism spectrum disorders are consistent across cultures, they vary greatly by gender, with boys diagnosed far more frequently than girls. The average male-to-female diagnosis ratio for ASDs is 4.2:1,[136] with 1 in 70 boys, but only 1 in 315 girls.[137] Girls, however, are more likely to have associated cognitive impairment. Among those with an ASD and intellectual disability, the sex ratio may be closer to 2:1.[138] Prevalence differences may be a result of gender differences in expression of clinical symptoms, with women and girls with autism showing less atypical behaviors and, therefore, less likely to receive an ASD diagnosis.[139]
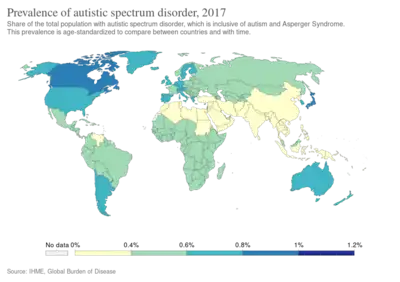
Autism prevalence has been estimated at 1-2 per 1,000, Asperger syndrome at roughly 0.6 per 1,000, childhood disintegrative disorder at 0.02 per 1,000, and PDD-NOS at 3.7 per 1,000.[140] These rates are consistent across cultures and ethnic groups, as autism is considered a universal disorder.[41]
Using DSM-V criteria 92% of the children diagnosed with a autism spectrum disorder per DSM-IV still meet the diagnostic criteria of an autism spectrum disorder. However if both Autism Spectrum Disorder and Social Communication Disorder categories of DSM-V are combined, the prevalence of autism is mostly unchanged from the prevalence per the DSM-IV criteria. The best estimate for prevalence of ASD is 0.7% or 1 child in 143 children.[141] Relatively mild forms of autism, such as Aspergers as well as other developmental disorders were included in the recent DSM-5 diagnostic criteria.[142] ASD rates were constant between 2014 and 2016 but twice the rate compared to the time period between 2011 and 2014 (1.25 vs 2.47%). A Canadian meta-analysis from 2019 confirmed these effects as the profiles of people diagnosed with autism became less and less different from the profiles of the general population.[143] In the US, the rates for diagnosed ASD have been steadily increasing since 2000 when records began being kept.[144] While it remains unclear whether this trend represents a true rise in incidence, it likely reflects changes in ASD diagnostic criteria, improved detection, and increased public awareness of autism.[145]
United States
In the United States it is estimated to affect more than 2% of children (about 1.5 million) as of 2016.[146] According to the latest CDC prevalence reports, 1 in 59 children (1.7%) in the United States had a diagnosis of ASD in 2014, reflecting a 2.5-fold increase from the prevalence rate in 2000.[142] Prevalence is estimated at 6 per 1,000 for autism spectrum disorders as a whole,[140] although prevalence rates vary for each of the developmental disorders in the spectrum.
History
Controversies have surrounded various claims regarding the etiology of autism spectrum disorders. In the 1950s, the "refrigerator mother theory" emerged as an explanation for autism. The hypothesis was based on the idea that autistic behaviors stem from the emotional frigidity, lack of warmth, and cold, distant, rejecting demeanor of a child's mother.[147] Naturally, parents of children with an autism spectrum disorder suffered from blame, guilt, and self-doubt, especially as the theory was embraced by the medical establishment and went largely unchallenged into the mid-1960s. The "refrigerator mother" theory has since continued to be refuted in scientific literature, including a 2015 systematic review which showed no association between caregiver interaction and language outcomes in ASD.[148]
Leo Kanner, a child psychiatrist, was the first person to describe ASD as a neurodevelopmental disorder in 1943 by calling it 'infantile autism' and therefore rejected the 'refrigerator mother' theory.[149]
Another controversial claim suggests that watching extensive amounts of television may cause autism. This hypothesis was largely based on research suggesting that the increasing rates of autism in the 1970s and 1980s were linked to the growth of cable television at this time.[69]
Society and culture
Caregivers
Families who care for an autistic child face added stress from a number of different causes. Parents may struggle to understand the diagnosis and to find appropriate care options. Parents often take a negative view of the diagnosis, and may struggle emotionally. In the words of one parent whose two children were both diagnosed with autism, "In the moment of diagnosis, it feels like the death of your hopes and dreams."[150] More than half of parents over the age of 50 are still living with their child as about 85% of people with ASD have difficulties living independently.[151]
Autism rights movement
The autism rights movement is a social movement within the context of disability rights that emphasizes the concept of neurodiversity, viewing the autism spectrum as a result of natural variations in the human brain rather than a disorder to be cured.[152] The autism rights movement advocates for including greater acceptance of autistic behaviors; therapies that focus on coping skills rather than imitating the behaviors of those without autism;[153] and the recognition of the autistic community as a minority group.[153][154] Autism rights or neurodiversity advocates believe that the autism spectrum is genetic and should be accepted as a natural expression of the human genome. This perspective is distinct from two other likewise distinct views: the medical perspective, that autism is caused by a genetic defect and should be addressed by targeting the autism gene(s), and fringe theories that autism is caused by environmental factors such as vaccines.[152] A common criticism against autistic activists is that the majority of them are "high-functioning" or have Asperger syndrome and do not represent the views of "low-functioning" autistic people.[154]
Academic performance
The number of students identified and served as eligible for autism services in the United States has increased from 5,413 children in 1991–1992 to 370,011 children in the 2010–2011 academic school year.[155] The United States Department of Health and Human Services reported approximately 1 in 68 children at age 8 are diagnosed with autism spectrum disorder (ASD) although onset is typically between ages 2 and 4.[155]
The increasing number of students with ASD in the schools presents significant challenges to teachers, school psychologists, and other school professionals.[155] These challenges include developing a consistent practice that best support the social and cognitive development of the increasing number of students with ASD.[155] Although there is considerable research addressing assessment, identification, and support services for children with ASD, there is a need for further research focused on these topics within the school context.[155] Further research on appropriate support services for students with ASD will provide school psychologists and other education professionals with specific directions for advocacy and service delivery that aim to enhance school outcomes for students with ASD.[155]
Attempts to identify and use best intervention practices for students with autism also pose a challenge due to overdependence on popular or well-known interventions and curricula.[155] Some evidence suggests that although these interventions work for some students, there remains a lack of specificity for which type of student, under what environmental conditions (one-on-one, specialized instruction or general education) and for which targeted deficits they work best.[155] More research is needed to identify what assessment methods are most effective for identifying the level of educational needs for students with ASD.
A difficulty for academic performance in students with ASD, is the tendency to generalize learning.[53] Learning is different for each student, which is the same for students with ASD. To assist in learning, accommodations are commonly put into place for students with differing abilities. The existing schema of these students works in different ways and can be adjusted to best support the educational development for each student.[156]
The cost of educating a student with ASD in the US is about $8,600 a year more than the cost of educating an average student, which is about $12,000.[157]
Employment
About half of people in their 20s with autism are unemployed, and one third of those with graduate degrees may be unemployed.[158] Among those on the autism spectrum who find work, most are employed in sheltered settings working for wages below the national minimum.[159] While employers state hiring concerns about productivity and supervision, experienced employers of autistics give positive reports of above average memory and detail orientation as well as a high regard for rules and procedure in autistic employees.[158] A majority of the economic burden of autism is caused by lost productivity in the job market.[160] Some studies also find decreased earning among parents who care for autistic children.[161][162] Adding content related to autism in existing diversity training can clarify misconceptions, support employees, and help provide new opportunities for autistics.
References
- ↑ Narayan, Sunil; Rao, JS Mohan; K, Nagarajan; Mohammed, Faruq; Kandasamy, Preeti; Subramaniam, Mahadevan (14 April 2020). "Non-Syndromic Autistic Spectral Disorders in Tamilian Chldren Commonly Associated with Brain imaging anomalies and Spectral EEG changes (4209)". Neurology. 94 (15 Supplement). ISSN 0028-3878. Archived from the original on 27 August 2021. Retrieved 4 August 2020.
- ↑ Baron-Cohen S, Scott FJ, Allison C, Williams J, Bolton P, Matthews FE, Brayne C (June 2009). "Prevalence of autism-spectrum conditions: UK school-based population study". The British Journal of Psychiatry. 194 (6): 500–9. doi:10.1192/bjp.bp.108.059345. PMID 19478287.
We favour use of the term 'autism-spectrum condition' rather than 'autism-spectrum disorder' as it is less stigmatising, and it reflects that these individuals have not only disabilities which require a medical diagnosis, but also areas of cognitive strength
- 1 2 3 4 5 6 7 8 9 10 11 American Psychiatric Association (2013). "Autism Spectrum Disorder. 299.00 (F84.0)". Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington, VA: American Psychiatric Publishing. pp. 50–59. doi:10.1176/appi.books.9780890425596. ISBN 978-0-89042-559-6.
- 1 2 3 Howlin, P; Magiati, I (March 2017). "Autism spectrum disorder: outcomes in adulthood". Current opinion in psychiatry. 30 (2): 69–76. doi:10.1097/YCO.0000000000000308. PMID 28067726.
- 1 2 3 4 5 6 7 8 9 "Autism Spectrum Disorder". NIMH. 2018. Archived from the original on 21 April 2017. Retrieved 21 February 2021.
- ↑ Case-Smith J, Arbesman M (2008). "Evidence-based review of interventions for autism used in or of relevance to occupational therapy". The American Journal of Occupational Therapy. 62 (4): 416–29. doi:10.5014/ajot.62.4.416. PMID 18712004.
- 1 2 Accordino RE, Kidd C, Politte LC, Henry CA, McDougle CJ (2016). "Psychopharmacological interventions in autism spectrum disorder". Expert Opinion on Pharmacotherapy. 17 (7): 937–52. doi:10.1517/14656566.2016.1154536. PMID 26891879. S2CID 6255194.
- 1 2 Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators) (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- ↑ Tick B, Bolton P, Happé F, Rutter M, Rijsdijk F (May 2016). "Heritability of autism spectrum disorders: a meta-analysis of twin studies". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 57 (5): 585–95. doi:10.1111/jcpp.12499. PMC 4996332. PMID 26709141.
- ↑ "Autism spectrum disorder fact sheet" (PDF). DSM5.org. American Psychiatric Publishing. 2013. Archived from the original (PDF) on 6 October 2013. Retrieved 13 October 2013.
- 1 2 Lai MC, Lombardo MV, Chakrabarti B, Baron-Cohen S (23 April 2013). "Subgrouping the autism "spectrum": reflections on DSM-5". PLOS Biology. 11 (4): e1001544. doi:10.1371/journal.pbio.1001544. PMC 3635864. PMID 23630456.
- 1 2 3 "10 Facts about Autism Spectrum Disorder (ASD)". Early Childhood Development | ACF. Archived from the original on 6 November 2019. Retrieved 6 November 2019.
- ↑ "HRSA-led study estimates 1 in 40 U.S. children has diagnosed autism". hrsa.gov. 19 November 2018. Archived from the original on 17 October 2019. Retrieved 17 October 2019.
- ↑ Sanchack, KE; Thomas, CA (15 December 2016). "Autism Spectrum Disorder: Primary Care Principles". American family physician. 94 (12): 972–979. PMID 28075089.
- 1 2 Lord C, Cook EH, Leventhal BL, Amaral DG (November 2000). "Autism spectrum disorders". Neuron. 28 (2): 355–63. doi:10.1016/S0896-6273(00)00115-X. PMID 11144346.
- ↑ American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., text revision (DSM-IV-TR). 2000. ISBN 0890420254. Diagnostic criteria for 299.80 Asperger's Disorder (AD). "Archive copy". Archived from the original on 7 June 2007. Retrieved 4 August 2020.
{{cite web}}: CS1 maint: archived copy as title (link) CS1 maint: bot: original URL status unknown (link) - 1 2 National Institute of Mental Health. Autism spectrum disorders (pervasive developmental disorders); 2009 [archived 29 April 2009].
- ↑ Freitag CM (January 2007). "The genetics of autistic disorders and its clinical relevance: a review of the literature". Molecular Psychiatry. 12 (1): 2–22. doi:10.1038/sj.mp.4001896. PMID 17033636. S2CID 205678822.
- 1 2 Piven J, Palmer P, Jacobi D, Childress D, Arndt S (February 1997). "Broader autism phenotype: evidence from a family history study of multiple-incidence autism families". The American Journal of Psychiatry. 154 (2): 185–90. doi:10.1176/ajp.154.2.185. PMID 9016266.
- ↑ Klin A (May 2006). "[Autism and Asperger syndrome: an overview]". Revista Brasileira de Psiquiatria. 28 (suppl 1): S3-11. doi:10.1590/S1516-44462006000500002. PMID 16791390.
- ↑ "Home | APA DSM-5". Dsm5.org. Archived from the original on 19 November 2008. Retrieved 21 February 2012.
- ↑ Kulage KM, Smaldone AM, Cohn EG (August 2014). "How will DSM-5 affect autism diagnosis? A systematic literature review and meta-analysis". Journal of Autism and Developmental Disorders. 44 (8): 1918–32. doi:10.1007/s10803-014-2065-2. PMID 24531932.
- ↑ "Profiles and criteria – NAS". autism.org.uk. Archived from the original on 28 July 2020. Retrieved 4 August 2020.
- ↑ "DSM-5 Diagnostic Criteria". U.S. Department of Health & Human Services Interagency Autism Coordinating Committee. Archived from the original on 11 February 2017. Retrieved 17 May 2017.
- 1 2 3 4 5 Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J (August 2018). "Autism spectrum disorder". Lancet. 392 (10146): 508–520. doi:10.1016/S0140-6736(18)31129-2. PMID 30078460. S2CID 51922565.
- 1 2 American Psychiatric Association, ed. (2013). "Autism Spectrum Disorder, 299.00 (F84.0)". Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. American Psychiatric Publishing. pp. 50–59.
- 1 2 Treffert DA (May 2009). "The savant syndrome: an extraordinary condition. A synopsis: past, present, future". Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 364 (1522): 1351–7. doi:10.1098/rstb.2008.0326. PMC 2677584. PMID 19528017.
- ↑ Minshawi NF, Hurwitz S, Fodstad JC, Biebl S, Morriss DH, McDougle CJ (2014). "The association between self-injurious behaviors and autism spectrum disorders". Psychology Research and Behavior Management. 7: 125–36. doi:10.2147/PRBM.S44635. PMC 3990505. PMID 24748827.
- 1 2 Oliver C, Richards C (October 2015). "Practitioner Review: Self-injurious behaviour in children with developmental delay". J Child Psychol Psychiatry (Review). 56 (10): 1042–54. doi:10.1111/jcpp.12425. PMID 25916173.
- 1 2 3 Minshawi NF, Hurwitz S, Fodstad JC, Biebl S, Morriss DH, McDougle CJ (April 2014). "The association between self-injurious behaviors and autism spectrum disorders". Psychology Research and Behavior Management. 7: 125–36. doi:10.2147/PRBM.S44635. PMC 3990505. PMID 24748827.
- ↑ Richler J, Huerta M, Bishop SL, Lord C (1 January 2010). "Developmental trajectories of restricted and repetitive behaviors and interests in children with autism spectrum disorders". Development and Psychopathology. 22 (1): 55–69. doi:10.1017/S0954579409990265. PMC 2893549. PMID 20102647.
- ↑ Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.). Washington, D.C.: American Psychiatric Association. 2000.
- ↑ "NINDS Asperger Syndrome Information Page". National Institute of Neurological Disorders and Stroke. Archived from the original on 17 July 2020. Retrieved 4 August 2020.
- ↑ Mesibov GB (1997). "Ask the Editor: What is PDD-NOS and how is it diagnosed?". Journal of Autism and Developmental Disorders. 27 (4).
- ↑ Zwaigenbaum L, Bryson S, Lord C, Rogers S, Carter A, Carver L, et al. (May 2009). "Clinical assessment and management of toddlers with suspected autism spectrum disorder: insights from studies of high-risk infants". Pediatrics. 123 (5): 1383–91. doi:10.1542/peds.2008-1606. PMC 2833286. PMID 19403506.
- ↑ Lord C (November 1995). "Follow-up of two-year-olds referred for possible autism". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 36 (8): 1365–82. doi:10.1111/j.1469-7610.1995.tb01669.x. PMID 8988272.
- ↑ Zwaigenbaum L (October 2001). "Autistic spectrum disorders in preschool children". Canadian Family Physician. 47 (10): 2037–42. PMC 2018435. PMID 11723598. Archived from the original on 28 July 2020. Retrieved 4 August 2020.
- ↑ Martínez-Pedraza F, Carter AS (July 2009). "Autism spectrum disorders in young children". Child and Adolescent Psychiatric Clinics of North America. 18 (3): 645–63. doi:10.1016/j.chc.2009.02.002. PMC 3166636. PMID 19486843.
- ↑ Werner E, Dawson G, Munson J, Osterling J (June 2005). "Variation in early developmental course in autism and its relation with behavioral outcome at 3-4 years of age". Journal of Autism and Developmental Disorders. 35 (3): 337–50. doi:10.1007/s10803-005-3301-6. PMID 16119475. S2CID 22485657.
- ↑ "Autism spectrum disorder – childhood disintegrative disorder: MedlinePlus Medical Encyclopedia". medlineplus.gov. Archived from the original on 26 July 2020. Retrieved 8 May 2020.
- 1 2 3 4 Mash, Eric J.; Barkley, Russell A. (2003). Child Psychopathology. New York: The Guilford Press. pp. 409–454.
- ↑ Ellis Weismer S, Kover ST (December 2015). "Preschool language variation, growth, and predictors in children on the autism spectrum". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 56 (12): 1327–37. doi:10.1111/jcpp.12406. PMC 4565784. PMID 25753577.
- ↑ Dawson G, Osterling J (1997). "Early Intervention in Autism". In Guralnick MJ (ed.). The effectiveness of early intervention. Baltimore: Brookes. pp. 307–326.
- ↑ Barnhill GP (2007). "Outcomes in adults with Asperger syndrome". Focus on Autism and Other Developmental Disabilities. 22 (2): 116–126. doi:10.1177/10883576070220020301.
- ↑ Howlin P, Moss P (May 2012). "Adults with autism spectrum disorders". Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie. 57 (5): 275–83. doi:10.1177/070674371205700502. PMID 22546059. S2CID 44544407.
- ↑ Frye RE (August 2018). "Social Skills Deficits in Autism Spectrum Disorder: Potential Biological Origins and Progress in Developing Therapeutic Agents". CNS Drugs. 32 (8): 713–734. doi:10.1007/s40263-018-0556-y. PMC 6105175. PMID 30105528.
- 1 2 3 4 5 6 7 Augustyn, Marilyn. "Autism spectrum disorder: Clinical features". UpToDate. Archived from the original on 26 July 2020. Retrieved 22 March 2020.
- ↑ Fusaroli R, Lambrechts A, Bang D, Bowler DM, Gaigg SB (March 2017). "Is voice a marker for Autism spectrum disorder? A systematic review and meta-analysis" (PDF). Autism Research. 10 (3): 384–407. doi:10.1002/aur.1678. PMID 27501063. Archived (PDF) from the original on 20 March 2021. Retrieved 4 August 2020.
- ↑ "Autism: Overview". American Speech-Language-Hearing Association. Archived from the original on 23 April 2019. Retrieved 17 December 2017.
- 1 2 3 4 "Autism Spectrum Disorder: Communication Problems in Children". NIDCD. 18 August 2015. Archived from the original on 22 December 2017. Retrieved 17 December 2017.
- 1 2 Vicker, Beverly. "Social communication and language characteristics associated with high-functioning, verbal children and adults with autism spectrum disorder". Indiana Resource Center for Autism. Archived from the original on 14 December 2018. Retrieved 17 December 2017.
- ↑ Keating CT, Cook JL (July 2020). "Facial expression production and recognition in autism spectrum disorders: a shifting landscape". Child Adolesc Psychiatr Clin N Am (Review). 29 (3): 557–571. doi:10.1016/j.chc.2020.02.006. PMID 32471602.
- 1 2 Lawson, Wendy (2001). Understanding and Working With the Spectrum of Autism An Insider's View. Philadelphia, PA: Jessica Kingsley Publishers London and Philadelphia. pp. 33. ISBN 978-1853029714.
- ↑ "Engaging people on the autism spectrum". Autism Spectrum Australia. 7 October 2013. Archived from the original on 29 September 2020. Retrieved 4 August 2020.
- ↑ Shaughnessy Hinerman, Paige (1983). Teaching Autistic Children to Communicate. Rockville, Maryland: Aspens System Corporation. p. 180. ISBN 978-0-89443-884-4.
- ↑ Tager-Flusberg H (2010). "The origins of social impairments in autism spectrum disorder: studies of infants at risk". Neural Networks. 23 (8–9): 1072–6. doi:10.1016/j.neunet.2010.07.008. PMC 2956843. PMID 20800990.
- ↑ "Signs & Symptoms – Autism Spectrum Disorder (ASD) – NCBDDD – CDC". Centers for Disease Control and Prevention. 26 February 2015. Archived from the original on 13 August 2020. Retrieved 4 August 2020.
- 1 2 3 4 5 6 7 8 9 10 11 Chen JA, Peñagarikano O, Belgard TG, Swarup V, Geschwind DH (2015). "The emerging picture of autism spectrum disorder: genetics and pathology". Annu Rev Pathol (Review). 10: 111–44. doi:10.1146/annurev-pathol-012414-040405. PMID 25621659.
- ↑ Werling DM, Brand H, An JY, Stone MR, Zhu L, Glessner JT, et al. (April 2018). "An analytical framework for whole-genome sequence association studies and its implications for autism spectrum disorder". Nature Genetics. 50 (5): 727–736. doi:10.1038/s41588-018-0107-y. PMC 5961723. PMID 29700473.
- ↑ Gardener H, Spiegelman D, Buka SL (August 2011). "Perinatal and neonatal risk factors for autism: a comprehensive meta-analysis". Pediatrics. 128 (2): 344–55. doi:10.1542/peds.2010-1036. PMC 3387855. PMID 21746727.
- 1 2 Gardener H, Spiegelman D, Buka SL (July 2009). "Prenatal risk factors for autism: comprehensive meta-analysis". The British Journal of Psychiatry. 195 (1): 7–14. doi:10.1192/bjp.bp.108.051672. PMC 3712619. PMID 19567888.
- ↑ Mazahery H, Camargo CA, Conlon C, Beck KL, Kruger MC, von Hurst PR (April 2016). "Vitamin D and Autism Spectrum Disorder: A Literature Review". Nutrients. 8 (4): 236. doi:10.3390/nu8040236. PMC 4848704. PMID 27110819.
- ↑ Deer, Brian (8 February 2009). "MMR doctor Andrew Wakefield fixed data on autism". The Sunday Times. Archived from the original on 20 March 2017. Retrieved 4 August 2020.
- ↑ Boseley, Sarah (2 February 2010). "Lancet retracts 'utterly false' MMR paper". The Guardian. Archived from the original on 17 January 2021. Retrieved 4 August 2020 – via theguardian.com.
- ↑ Committee to Review Adverse Effects of Vaccines, Institute Of M, Stratton K, Ford A, Rusch E, Clayton EW, et al. (Committee to Review Adverse Effects of Vaccines; Board on Population Health and Public Health Practice; Institute of Medicine) (August 2011). "Chapter: 6 Influenza Vaccine". In Stratton K, Ford A, Rusch E, Clayton EW (eds.). Adverse Effects of Vaccines: Evidence and Causality. Washington (DC): National Academies Press (US). doi:10.17226/13164. ISBN 978-0-309-21435-3. PMID 24624471. Archived from the original on 27 August 2021. Retrieved 4 August 2020.
- ↑ Flaherty DK (October 2011). "The vaccine-autism connection: a public health crisis caused by unethical medical practices and fraudulent science". The Annals of Pharmacotherapy. 45 (10): 1302–4. doi:10.1345/aph.1Q318. PMID 21917556.
- ↑ Godlee F, Smith J, Marcovitch H (January 2011). "Wakefield's article linking MMR vaccine and autism was fraudulent". BMJ. 342: c7452. doi:10.1136/bmj.c7452. PMID 21209060. S2CID 43640126. Archived from the original on 11 November 2013. Retrieved 4 August 2020.
- ↑ Tan M, Parkin JE (November 2000). "Route of decomposition of thiomersal (thimerosal)". International Journal of Pharmaceutics. 208 (1–2): 23–34. doi:10.1016/S0378-5173(00)00514-7. PMID 11064208.
- 1 2 Waterhouse L (December 2008). "Autism overflows: increasing prevalence and proliferating theories". Neuropsychology Review. 18 (4): 273–86. doi:10.1007/s11065-008-9074-x. PMID 19015994. S2CID 8863638.
- ↑ "Frequently Asked Questions about Thimerosal". Centers for Disease Control and Prevention. Archived from the original on 7 May 2019. Retrieved 21 February 2017.
- ↑ Taylor LE, Swerdfeger AL, Eslick GD (June 2014). "Vaccines are not associated with autism: an evidence-based meta-analysis of case-control and cohort studies". Vaccine. 32 (29): 3623–9. doi:10.1016/j.vaccine.2014.04.085. PMID 24814559.
- Lay summary in: news.com.au http://www.news.com.au/lifestyle/health/vaccination-versus-autism-study-professor-guy-eslick-tells-why-hes-taking-on-the-scaremongers/story-fneuzlbd-1226929208418.
{{cite journal}}: Missing or empty|title=(help)
- Lay summary in: news.com.au http://www.news.com.au/lifestyle/health/vaccination-versus-autism-study-professor-guy-eslick-tells-why-hes-taking-on-the-scaremongers/story-fneuzlbd-1226929208418.
- ↑ Koenig K, Tsatsanis KD, Volkmar FR (2001). "Neurobiology and Genetics of Autism : A Developmental Perspective". In Burack JA, Charman T, Yirmiya N, Zelazo PR (eds.). The development of autism: perspectives from theory and research. Mahwah, N.J.: L. Erlbaum. pp. 73–92. ISBN 9780805832457. OCLC 806185029.
- ↑ Minshew NJ (April 1996). "Brief report: brain mechanisms in autism: functional and structural abnormalities". Journal of Autism and Developmental Disorders. 26 (2): 205–9. doi:10.1007/BF02172013. PMID 8744486. S2CID 8134205.
- ↑ Stanfield AC, McIntosh AM, Spencer MD, Philip R, Gaur S, Lawrie SM (June 2008). "Towards a neuroanatomy of autism: a systematic review and meta-analysis of structural magnetic resonance imaging studies". European Psychiatry. 23 (4): 289–99. doi:10.1016/j.eurpsy.2007.05.006. PMID 17765485.
- ↑ Lefebvre A, Beggiato A, Bourgeron T, Toro R (July 2015). "Neuroanatomical Diversity of Corpus Callosum and Brain Volume in Autism: Meta-analysis, Analysis of the Autism Brain Imaging Data Exchange Project, and Simulation". Biological Psychiatry. 78 (2): 126–34. doi:10.1016/j.biopsych.2015.02.010. PMID 25850620. S2CID 8794474.
- ↑ Sugranyes G, Kyriakopoulos M, Corrigall R, Taylor E, Frangou S (2011). "Autism spectrum disorders and schizophrenia: meta-analysis of the neural correlates of social cognition". PLOS ONE. 6 (10): e25322. Bibcode:2011PLoSO...625322S. doi:10.1371/journal.pone.0025322. PMC 3187762. PMID 21998649.
- 1 2 3 4 5 O'Reilly C, Lewis JD, Elsabbagh M (2017). "Is functional brain connectivity atypical in autism? A systematic review of EEG and MEG studies". PLoS ONE (Review). 12 (5): e0175870. doi:10.1371/journal.pone.0175870. PMC 5414938. PMID 28467487.
- 1 2 3 4 5 6 7 8 Azhari, Atiqah; Azizan, Farouq; Esposito, Gianluca (July 2019). "A systematic review of gut-immune-brain mechanisms in Autism Spectrum Disorder". Developmental Psychobiology. 61 (5): 752–771. doi:10.1002/dev.21803. ISSN 1098-2302. PMID 30523646.
- ↑ Fadiga L, Craighero L, Olivier E (April 2005). "Human motor cortex excitability during the perception of others' action". Current Opinion in Neurobiology. 15 (2): 213–8. doi:10.1016/j.conb.2005.03.013. PMID 15831405.
- ↑ Shamay-Tsoory SG (February 2011). "The neural bases for empathy". The Neuroscientist. 17 (1): 18–24. doi:10.1177/1073858410379268. PMID 21071616.
- ↑ Dinstein I, Thomas C, Behrmann M, Heeger DJ (January 2008). "A mirror up to nature". Current Biology. 18 (1): R13-8. doi:10.1016/j.cub.2007.11.004. PMC 2517574. PMID 18177704.
- ↑ Kalat J (2009). Biological Psychology (Tenth ed.). pp. 237–8. ISBN 978-0-495-60300-9.
- ↑ Kennedy DP, Adolphs R (November 2012). "The social brain in psychiatric and neurological disorders". Trends in Cognitive Sciences. 16 (11): 559–72. doi:10.1016/j.tics.2012.09.006. PMC 3606817. PMID 23047070.
- ↑ Schultz RT (2005). "Developmental deficits in social perception in autism: the role of the amygdala and fusiform face area". International Journal of Developmental Neuroscience. 23 (2–3): 125–41. doi:10.1016/j.ijdevneu.2004.12.012. PMID 15749240.
- ↑ Haas RH, Parikh S, Falk MJ, et al. (December 2007). "Mitochondrial disease: a practical approach for primary care physicians". Pediatrics. 120 (6): 1326–33. doi:10.1542/peds.2007-0391. PMID 18055683. S2CID 4939996.
- 1 2 Rossignol DA, Frye RE (March 2012). "Mitochondrial dysfunction in autism spectrum disorders: a systematic review and meta-analysis". Molecular Psychiatry. 17 (3): 290–314. doi:10.1038/mp.2010.136. PMC 3285768. PMID 21263444.
- ↑ Gentile S (August 2015). "Prenatal antidepressant exposure and the risk of autism spectrum disorders in children. Are we looking at the fall of Gods?". Journal of Affective Disorders. 182: 132–7. doi:10.1016/j.jad.2015.04.048. PMID 25985383.
- ↑ Dragioti E, Solmi M, Favaro A, Fusar-Poli P, Dazzan P, Thompson T, et al. (October 2019). "Association of Antidepressant Use With Adverse Health Outcomes: A Systematic Umbrella Review". JAMA Psychiatry. 76 (12): 1241. doi:10.1001/jamapsychiatry.2019.2859. PMC 6777224. PMID 31577342.
- ↑ "Autism Spectrum Disorder (ASD): Screening and Diagnosis". Centers for Disease Control and Prevention. 26 February 2015. Archived from the original on 31 March 2019. Retrieved 4 August 2020.
- ↑ Lord C, Risi S, DiLavore PS, Shulman C, Thurm A, Pickles A (June 2006). "Autism from 2 to 9 years of age". Archives of General Psychiatry. 63 (6): 694–701. doi:10.1001/archpsyc.63.6.694. PMID 16754843.
- 1 2 Volkmar F, Cook EH, Pomeroy J, Realmuto G, Tanguay P (December 1999). "Practice parameters for the assessment and treatment of children, adolescents, and adults with autism and other pervasive developmental disorders. American Academy of Child and Adolescent Psychiatry Working Group on Quality Issues". Journal of the American Academy of Child and Adolescent Psychiatry. 38 (12 Suppl): 32S–54S. doi:10.1016/s0890-8567(99)80003-3. PMID 10624084.
- ↑ Constantino JN, Charman T (March 2016). "Diagnosis of autism spectrum disorder: reconciling the syndrome, its diverse origins, and variation in expression" (PDF). The Lancet. Neurology. 15 (3): 279–91. doi:10.1016/s1474-4422(15)00151-9. PMID 26497771. Archived (PDF) from the original on 26 July 2020. Retrieved 4 August 2020.
- 1 2 Simms, Mark D. (February 2017). "When Autistic Behavior Suggests a Disease Other than Classic Autism". Pediatric Clinics of North America. 64 (1): 127–138. doi:10.1016/j.pcl.2016.08.009. ISSN 1557-8240. PMID 27894440.
- ↑ Filipek PA, Accardo PJ, Ashwal S, Baranek GT, Cook EH, Dawson G, et al. (August 2000). "Practice parameter: screening and diagnosis of autism: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Child Neurology Society". Neurology. 55 (4): 468–79. doi:10.1212/wnl.55.4.468. PMID 10953176.
- ↑ Filipek PA, Accardo PJ, Baranek GT, Cook EH, Dawson G, Gordon B, et al. (December 1999). "The screening and diagnosis of autistic spectrum disorders". Journal of Autism and Developmental Disorders. 29 (6): 439–84. doi:10.1023/A:1021943802493. PMID 10638459.
- 1 2 Ozonoff S, Goodlin-Jones BL, Solomon M (September 2005). "Evidence-based assessment of autism spectrum disorders in children and adolescents" (PDF). Journal of Clinical Child and Adolescent Psychology. 34 (3): 523–40. doi:10.1207/s15374424jccp3403_8. PMID 16083393. S2CID 14322690. Archived from the original (PDF) on 18 April 2021. Retrieved 4 August 2020.
- ↑ Corsello C, Hus V, Pickles A, Risi S, Cook EH, Leventhal BL, Lord C (September 2007). "Between a ROC and a hard place: decision making and making decisions about using the SCQ". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 48 (9): 932–40. doi:10.1111/j.1469-7610.2007.01762.x. hdl:2027.42/74877. PMID 17714378.
- ↑ Huerta M, Lord C (February 2012). "Diagnostic evaluation of autism spectrum disorders". Pediatric Clinics of North America. 59 (1): 103–11, xi. doi:10.1016/j.pcl.2011.10.018. PMC 3269006. PMID 22284796.
- 1 2 3 4 5 6 7 Siu, Albert L.; US Preventive Services Task Force (USPSTF); Bibbins-Domingo, Kirsten; Grossman, David C.; Baumann, Linda Ciofu; Davidson, Karina W.; Ebell, Mark; García, Francisco A. R.; Gillman, Matthew; Herzstein, Jessica; Kemper, Alex R. (16 February 2016). "Screening for Autism Spectrum Disorder in Young Children: US Preventive Services Task Force Recommendation Statement". JAMA. 315 (7): 691–696. doi:10.1001/jama.2016.0018. ISSN 1538-3598. PMID 26881372.
- 1 2 3 4 5 6 7 Blumberg, Stephen J.; Zablotsky, Benjamin; Avila, Rosa M.; Colpe, Lisa J.; Pringle, Beverly A.; Kogan, Michael D. (October 2016). "Diagnosis lost: Differences between children who had and who currently have an autism spectrum disorder diagnosis". Autism: The International Journal of Research and Practice. 20 (7): 783–795. doi:10.1177/1362361315607724. ISSN 1461-7005. PMC 4838550. PMID 26489772.
- ↑ Helverschou SB, Bakken TL, Martinsen H (2011). Matson JL, Sturmey P (eds.). Psychiatric Disorders in People with Autism Spectrum Disorders: Phenomenology and Recognition. International handbook of autism and pervasive developmental disorders. New York: Springer. pp. 53–74. ISBN 9781441980649. OCLC 746203105.
- ↑ Underwood L, McCarthy J, Tsakanikos E (September 2010). "Mental health of adults with autism spectrum disorders and intellectual disability". Current Opinion in Psychiatry. 23 (5): 421–6. doi:10.1097/YCO.0b013e32833cfc18. PMID 20613532. S2CID 13735841.
- ↑ Ballaban-Gil K, Tuchman R (2000). "Epilepsy and epileptiform EEG: association with autism and language disorders". Mental Retardation and Developmental Disabilities Research Reviews. 6 (4): 300–8. doi:10.1002/1098-2779(2000)6:4<300::AID-MRDD9>3.0.CO;2-R. PMID 11107195.
- ↑ Wiznitzer M (September 2004). "Autism and tuberous sclerosis". Journal of Child Neurology. 19 (9): 675–9. doi:10.1177/08830738040190090701. PMID 15563013. S2CID 38157900.
- ↑ Zafeiriou DI, Ververi A, Vargiami E (June 2007). "Childhood autism and associated comorbidities". Brain & Development. 29 (5): 257–72. doi:10.1016/j.braindev.2006.09.003. PMID 17084999. S2CID 16386209.
- ↑ Satterstrom FK, Kosmicki JA, Wang J, et al. (February 2020). "Large-Scale Exome Sequencing Study Implicates Both Developmental and Functional Changes in the Neurobiology of Autism". Cell. 180 (3): 568–584.e23. doi:10.1016/j.cell.2019.12.036. PMID 31981491.
- ↑ Adam MP, Ardinger HH, Pagon RA, et al. (2019). "SYNGAP1-Related Intellectual Disability". Gene Reviews (Review). PMID 30789692. Archived from the original on 2 April 2021. Retrieved 4 August 2020.
- ↑ O'Brien G, Pearson J (June 2004). "Autism and learning disability". Autism. 8 (2): 125–40. doi:10.1177/1362361304042718. PMID 15165430.
- ↑ Lainhart J (1999). "Psychiatric problems in individuals with autism, their parents and siblings". International Review of Psychiatry. 11 (4): 278–298. doi:10.1080/09540269974177.
- ↑ Chisholm K, Lin A, Abu-Akel A, Wood SJ (August 2015). "The association between autism and schizophrenia spectrum disorders: A review of eight alternate models of co-occurrence" (PDF). Neuroscience and Biobehavioral Reviews. 55: 173–83. doi:10.1016/j.neubiorev.2015.04.012. PMID 25956249. S2CID 21450062. Archived (PDF) from the original on 8 June 2020. Retrieved 4 August 2020.
- ↑ Hamlyn J, Duhig M, McGrath J, Scott J (May 2013). "Modifiable risk factors for schizophrenia and autism—shared risk factors impacting on brain development". Neurobiology of Disease. 53: 3–9. doi:10.1016/j.nbd.2012.10.023. PMID 23123588.
- ↑ Crespi BJ, Thiselton DL (October 2011). "Comparative immunogenetics of autism and schizophrenia". Genes, Brain, and Behavior. 10 (7): 689–701. doi:10.1111/j.1601-183X.2011.00710.x. PMID 21649858.
- ↑ Tsakanikos E, Costello H, Holt G, Sturmey P, Bouras N (July 2007). "Behaviour management problems as predictors of psychotropic medication and use of psychiatric services in adults with autism" (PDF). Journal of Autism and Developmental Disorders. 37 (6): 1080–5. doi:10.1007/s10803-006-0248-1. PMID 17053989. Archived (PDF) from the original on 19 May 2012. Retrieved 4 August 2020.
- ↑ Rommelse NN, Franke B, Geurts HM, Hartman CA, Buitelaar JK (March 2010). "Shared heritability of attention-deficit/hyperactivity disorder and autism spectrum disorder". European Child & Adolescent Psychiatry. 19 (3): 281–95. doi:10.1007/s00787-010-0092-x. PMC 2839489. PMID 20148275.
- ↑ Baranek GT (October 2002). "Efficacy of sensory and motor interventions for children with autism". Journal of Autism and Developmental Disorders. 32 (5): 397–422. doi:10.1023/A:1020541906063. PMID 12463517.
- 1 2 Lugnegård T, Hallerbäck MU, Gillberg C (May 2012). "Personality disorders and autism spectrum disorders: what are the connections?". Comprehensive Psychiatry. 53 (4): 333–40. doi:10.1016/j.comppsych.2011.05.014. PMID 21821235.
- ↑ Tantam D (December 1988). "Lifelong eccentricity and social isolation. II: Asperger's syndrome or schizoid personality disorder?". The British Journal of Psychiatry. 153: 783–91. doi:10.1192/bjp.153.6.783. PMID 3256377.
- ↑ Sharon C. Ekleberry (2008). "Cluster A - Schizoid Personality Disorder and Substance Use Disorders". Integrated Treatment for Co-Occurring Disorders: Personality Disorders and Addiction. Routledge. pp. 31–32. ISBN 978-0789036933. Archived from the original on 25 February 2021. Retrieved 4 August 2020.
- ↑ McPartland J, Klin A (October 2006). "Asperger's syndrome". Adolescent Medicine Clinics. 17 (3): 771–88, abstract xiii. doi:10.1016/j.admecli.2006.06.010 (inactive 18 January 2021). PMID 17030291.
{{cite journal}}: CS1 maint: DOI inactive as of January 2021 (link) - ↑ Woodbury-Smith MR, Volkmar FR (January 2009). "Asperger syndrome". European Child & Adolescent Psychiatry (Submitted manuscript). 18 (1): 2–11. doi:10.1007/s00787-008-0701-0. PMID 18563474. S2CID 12808995. Archived from the original on 31 March 2019. Retrieved 4 August 2020.
- ↑ Coplan J, Jawad AF (July 2005). "Modeling clinical outcome of children with autistic spectrum disorders". Pediatrics. 116 (1): 117–22. doi:10.1542/peds.2004-1118. PMID 15995041. S2CID 8440775.
- Lay summary in: press release. 5 July 2005 http://stokes.chop.edu/publications/press/?ID=181.
{{cite journal}}: Missing or empty|title=(help)
- Lay summary in: press release. 5 July 2005 http://stokes.chop.edu/publications/press/?ID=181.
- ↑ Eldevik S, Hastings RP, Hughes JC, Jahr E, Eikeseth S, Cross S (May 2009). "Meta-analysis of Early Intensive Behavioral Intervention for children with autism". Journal of Clinical Child and Adolescent Psychology. 38 (3): 439–50. CiteSeerX 10.1.1.607.9620. doi:10.1080/15374410902851739. PMID 19437303. S2CID 205873629.
- 1 2 3 4 5 Smith T, Iadarola S (2015). "Evidence Base Update for Autism Spectrum Disorder". Journal of Clinical Child and Adolescent Psychology. 44 (6): 897–922. doi:10.1080/15374416.2015.1077448. PMID 26430947.
- 1 2 3 Myers SM, Johnson CP (November 2007). "Management of children with autism spectrum disorders". Pediatrics. 120 (5): 1162–82. doi:10.1542/peds.2007-2362. PMID 17967921. S2CID 1656920. Archived from the original on 12 June 2009. Retrieved 4 August 2020.
- Lay summary in: "Error". AAP. 29 October 2007.
- ↑ Sigman M, Capps L (2002). Children with Autism: A Developmental Perspective. Cambridge: Harvard University Press. pp. 178–179. ISBN 978-0-674-05313-7.
- ↑ Rogers SJ, Vismara LA (January 2008). "Evidence-based comprehensive treatments for early autism". Journal of Clinical Child and Adolescent Psychology. 37 (1): 8–38. doi:10.1080/15374410701817808. PMC 2943764. PMID 18444052.
- ↑ Benevides, Teal W; Shore, Stephen M; Andresen, May-Lynn; Caplan, Reid; Cook, Barb; Gassner, Dena L; Erves, Jasmine M; Hazlewood, Taylor M; King, M Caroline; Morgan, Lisa; Murphy, Lauren E (11 May 2020). "Interventions to address health outcomes among autistic adults: A systematic review". Autism. 24 (6): 1345–1359. doi:10.1177/1362361320913664. ISSN 1362-3613. PMC 7787674. PMID 32390461.
- 1 2 Zwaigenbaum L, Bauman ML, Choueiri R, Kasari C, Carter A, Granpeesheh D, et al. (October 2015). "Early Intervention for Children With Autism Spectrum Disorder Under 3 Years of Age: Recommendations for Practice and Research". Pediatrics. 136 (Supplement 1): S60-81. doi:10.1542/peds.2014-3667E. PMID 26430170. Archived from the original on 28 July 2020. Retrieved 4 August 2020.
- ↑ Reichow, Brian; Hume, Kara; Barton, Erin E.; Boyd, Brian A. (9 May 2018). "Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD)". The Cochrane Database of Systematic Reviews. 5: CD009260. doi:10.1002/14651858.CD009260.pub3. ISSN 1469-493X. PMC 6494600. PMID 29742275.
- ↑ Siewertsen CM, French ED, Teramoto M (2015). "Autism spectrum disorder and pet therapy". Advances in Mind-Body Medicine. 29 (2): 22–5. PMID 25831431.
- 1 2 Weissman L (March 2020). "Autism spectrum disorder in children and adolescents: Pharmacologic interventions". Archived from the original on 26 July 2020. Retrieved 17 March 2020.
- ↑ Williams Buckley A, Hirtz D, Oskoui M, et al. (March 2020). "Practice guideline: Treatment for insomnia and disrupted sleep behavior in children and adolescents with autism spectrum disorder: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology". Neurology. 94 (9): 392–404. doi:10.1212/WNL.0000000000009033. PMC 7238942. PMID 32051244.
- ↑ Harrop C (August 2015). "Evidence-based, parent-mediated interventions for young children with autism spectrum disorder: The case of restricted and repetitive behaviors". Autism. 19 (6): 662–72. doi:10.1177/1362361314545685. PMID 25186943. S2CID 32326472.
- ↑ Harrop C (August 2015). "Evidence-based, parent-mediated interventions for young children with autism spectrum disorder: The case of restricted and repetitive behaviors". Autism. 19 (6): 662–72. doi:10.1177/1362361314545685. PMID 25186943. S2CID 32326472.
- ↑ Ameis SH, Kassee C, Corbett-Dick P, et al. (November 2018). "Systematic review and guide to management of core and psychiatric symptoms in youth with autism". Acta Psychiatrica Scandinavica. 138 (5): 379–400. doi:10.1111/acps.12918. PMID 29904907. S2CID 49209337.
- ↑ Fombonne E (June 2009). "Epidemiology of pervasive developmental disorders". Pediatric Research. 65 (6): 591–8. doi:10.1203/PDR.0b013e31819e7203. PMID 19218885.
- ↑ (ADDM) Autism and Developmental Disabilities Monitoring Network Surveillance Year 2006 Principal Investigators (2009). "Prevalence of autism spectrum disorders-Autism and Developmental Disabilities Monitoring Network". MMWR Surveillance Summaries. 58: 1–20.
- ↑ Volkmar FR, Lord C, Bailey A, Schultz RT, Klin A (January 2004). "Autism and pervasive developmental disorders". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 45 (1): 135–70. doi:10.1046/j.0021-9630.2003.00317.x. PMID 14959806.
- ↑ Tsakanikos E, Underwood L, Kravariti E, Bouras N, McCarthy J (2011). "Gender differences in co-morbid psychopathology and clinical management in adults with autism spectrum disorders". Research in Autism Spectrum Disorders. 5 (2): 803–808. doi:10.1016/j.rasd.2010.09.009. ISSN 1750-9467.
- 1 2 Newschaffer CJ, Croen LA, Daniels J, Giarelli E, Grether JK, Levy SE, et al. (2007). "The epidemiology of autism spectrum disorders". Annual Review of Public Health. 28: 235–58. doi:10.1146/annurev.publhealth.28.021406.144007. PMID 17367287.
- ↑ Hollander, Eric; Hagerman, Randi Jenssen; Fein, Deborah (30 April 2018). Autism spectrum disorders (First ed.). Washington, DC: American Psychiatric Association Publishing. ISBN 978-1-61537-192-1. OCLC 1022084798.
- 1 2 Baio J, Wiggins L, Christensen DL, et al. (April 2018). "Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years – Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014". Morbidity and Mortality Weekly Report. Surveillance Summaries. 67 (6): 1–23. doi:10.15585/mmwr.ss6706a1. PMC 5919599. PMID 29701730.
- ↑ Rødgaard EM, Jensen K, Vergnes JN, Soulières I, Mottron L (August 2019). "Temporal Changes in Effect Sizes of Studies Comparing Individuals With and Without Autism: A Meta-analysis". JAMA Psychiatry. 76 (11): 1124. doi:10.1001/jamapsychiatry.2019.1956. PMC 6704749. PMID 31433441.
- ↑ "CDC Press Releases". CDC. 1 January 2016. Archived from the original on 11 October 2019. Retrieved 31 December 2019.
- ↑ Hill AP (2014). Volkmar FR (ed.). Epidemiology of autism spectrum disorders. Handbook of Autism and Pervasive Developmental Disorders. Diagnosis, Development, and Brain Mechanisms. Vol. 1. New York: Wiley. pp. 57–96. doi:10.1002/9781118911389. ISBN 9781118911389.
- ↑ "HRSA-led study estimates 1 in 40 U.S. children has diagnosed autism". HRSA News Room. U.S. Department of Health & Human Services, Health Resources and Services Administration. 19 November 2018. Archived from the original on 17 October 2019. Retrieved 17 October 2019.
- ↑ Kanner L (July 1949). "Problems of nosology and psychodynamics of early infantile autism". The American Journal of Orthopsychiatry. 19 (3): 416–26. doi:10.1111/j.1939-0025.1949.tb05441.x. PMID 18146742.
- ↑ Tager-Flusberg H (February 2016). "Risk Factors Associated With Language in Autism Spectrum Disorder: Clues to Underlying Mechanisms". Journal of Speech, Language, and Hearing Research. 59 (1): 143–54. doi:10.1044/2015_jslhr-l-15-0146. PMC 4867927. PMID 26502110.
- ↑ Harris, James (February 2018). "Leo Kanner and autism: a 75-year perspective". International Review of Psychiatry (Abingdon, England). 30 (1): 3–17. doi:10.1080/09540261.2018.1455646. ISSN 1369-1627. PMID 29667863. S2CID 4978549.
- ↑ Levinovitz, Alan. "An Alternative-Medicine Believer's Journey Back to Science". WIRED. Archived from the original on 6 March 2017. Retrieved 13 February 2017.
The entire diagnosis and explanation took no more than 45 minutes. 'In the moment of diagnosis, it feels like the death of your hopes and dreams,' Louise [Laidler] says. There's a quiet grief in her voice, even though two decades have passed. 'In a way, it's even harder than a death, because you can't mourn and go on,' she says. 'You have to figure out how to care for your new child.'
- ↑ Karst JS, Van Hecke AV (September 2012). "Parent and family impact of autism spectrum disorders: a review and proposed model for intervention evaluation". Clinical Child and Family Psychology Review. 15 (3): 247–77. doi:10.1007/s10567-012-0119-6. PMID 22869324.
- 1 2 Solomon, Andrew (25 May 2008). "The autism rights movement". New York. Archived from the original on 27 May 2008. Retrieved 27 May 2008.
- 1 2 Ratner, Paul (10 July 2016). "Should Autism Be Cured or Is "Curing" Offensive?". Big Think. Archived from the original on 16 June 2019. Retrieved 16 June 2019.
- 1 2 Jaarsma P, Welin S (March 2012). "Autism as a natural human variation: reflections on the claims of the neurodiversity movement". Health Care Analysis. 20 (1): 20–30. doi:10.1007/s10728-011-0169-9. PMID 21311979. S2CID 18618887. Archived from the original on 17 December 2019. Retrieved 4 August 2020.
- 1 2 3 4 5 6 7 8 Stichter JP, Riley-Tillman TC, Jimerson SR (December 2016). "Assessing, understanding, and supporting students with autism at school: Contemporary science, practice, and policy". School Psychology Quarterly. 31 (4): 443–449. doi:10.1037/spq0000184. PMID 27929316.
- ↑ "Jean Piaget's Theory of Cognitive Development | Simply Psychology". simplypsychology.org. Archived from the original on 20 February 2019. Retrieved 19 February 2019.
- ↑ "Facts and Statistics". Autism Society. Archived from the original on 30 October 2019. Retrieved 6 November 2019.
- 1 2 Ohl A, Grice Sheff M, Small S, Nguyen J, Paskor K, Zanjirian A (2017). "Predictors of employment status among adults with Autism Spectrum Disorder". Work. 56 (2): 345–355. doi:10.3233/WOR-172492. PMID 28211841.
- ↑ DePillis, Lydia (12 February 2016). "Disabled people are allowed to work for pennies per hour – but maybe not for much longer". Washington Post. Archived from the original on 1 January 2019. Retrieved 31 December 2018.
- ↑ Ganz ML (April 2007). "The lifetime distribution of the incremental societal costs of autism". Archives of Pediatrics & Adolescent Medicine. 161 (4): 343–9. doi:10.1001/archpedi.161.4.343. PMID 17404130.
- Lay summary in: Harvard School of Public Health. 25 April 2006 http://www.hsph.harvard.edu/news/press-releases/2006-releases/press04252006.html.
{{cite journal}}: Missing or empty|title=(help)
- Lay summary in: Harvard School of Public Health. 25 April 2006 http://www.hsph.harvard.edu/news/press-releases/2006-releases/press04252006.html.
- ↑ Montes G, Halterman JS (April 2008). "Association of childhood autism spectrum disorders and loss of family income". Pediatrics. 121 (4): e821-6. doi:10.1542/peds.2007-1594. PMID 18381511. S2CID 55179. Archived from the original on 4 March 2010.
- ↑ Montes G, Halterman JS (July 2008). "Child care problems and employment among families with preschool-aged children with autism in the United States". Pediatrics. 122 (1): e202-8. doi:10.1542/peds.2007-3037. PMID 18595965. Archived from the original on 6 December 2009.
External links
- Autism spectrum at Curlie
| Classification | |
|---|---|
| External resources |
|