Cephalic presentation
| Cephalic presentation | |
|---|---|
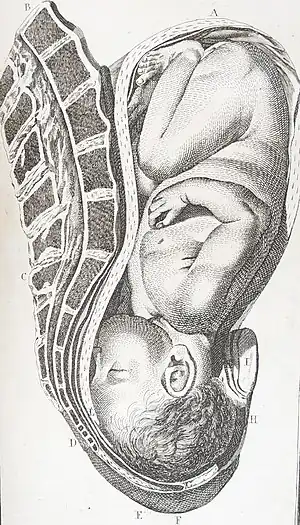 | |
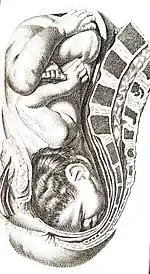
| Vertex presentation, occiput anterior, William Smellie, 1792 | |
| Specialty | Obstetrics |
A cephalic presentation or head presentation or head-first presentation is a situation at childbirth where the fetus is in a longitudinal lie and the head enters the pelvis first; the most common form of cephalic presentation is the vertex presentation, where the occiput is the leading part (the part that first enters the birth canal).[1] All other presentations are abnormal (malpresentations) and are either more difficult to deliver or not deliverable by natural means.
Engagement
The movement of the fetus to cephalic presentation is called head engagement. It occurs in the third trimester. In head engagement, the fetal head descends into the pelvic cavity so that only a small part (or none) of it can be felt abdominally. The perineum and cervix are further flattened and the head may be felt vaginally.[2] Head engagement is known colloquially as the baby drop, and in natural medicine as the lightening because of the release of pressure on the upper abdomen and renewed ease in breathing. However, it severely reduces bladder capacity resulting in a need to void more frequently.[3]
Classification
In the vertex presentation the head is flexed and the occiput leads the way. This is the most common configuration and seen at term in 95% of singletons.[1] If the head is extended, the face becomes the leading part. Face presentations account for less than 1% of presentations at term. In the sinicipital presentation the large fontanelle is the presenting part; with further labor the head will either flex or extend more so that in the end this presentation leads to a vertex or face presentation.[1] In the brow presentation the head is slightly extended, but less than in the face presentation. The chin presentation is a variant of the face presentation with maximum extension of the head.
Non-cephalic presentations are the breech presentation (3.5%) and the shoulder presentation (0.5%).[1]
Vertex presentation
The vertex is the area of the vault bounded anteriorly by the anterior fontanelle and the coronal suture, posteriorly by the posterior fontanelle and the lambdoid suture and laterally by 2 lines passing through the parietal eminences.
In the vertex presentation the occiput typically is anterior and thus in an optimal position to negotiate the pelvic curve by extending the head. In an occiput posterior position, labor becomes prolonged, and more operative interventions are deemed necessary.[4] The prevalence of the persistent occiput posterior is given as 4.7%.[4]
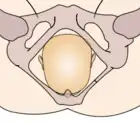
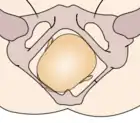
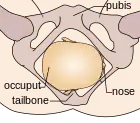
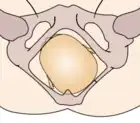
The vertex presentations are further classified according to the position of the occiput, both right, left, or transverse and anterior or posterior:
- Left Occipito-Anterior (LOA), Left Occipito-Posterior (LOP), Left Occipito-Transverse (LOT)
- Right Occipito-Anterior (ROA), Right Occipito-Posterior (ROP), Right Occipito-Transverse (ROT)
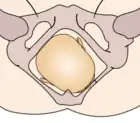 Right occipito-anterior |
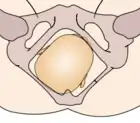
 Straight occipito-anterior |
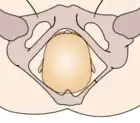
 Left occipito-anterior |
Right occipito-transverse |
 |
Left occipito-transverse |
 Right occipito-posterior |
 Straight occipito-posterior |
 Left occipito-posterior |
The Occipito-Anterior position is ideal for birth; it means that the baby is lined up so as to fit through the pelvis as easily as possible. The baby is head down, facing the spine, with its back anterior. In this position, the baby's chin is tucked onto its chest, so that the smallest part of its head will be applied to the cervix first. The position is usually "Left Occiput Anterior", or LOA. Occasionally, the baby may be "Right Occiput Anterior", or ROA.[5]
Face presentation
Factors that predispose to face presentation are prematurity, macrosomia, anencephaly and other malformations, cephalopelvic disproportion, and polyhydramnios.[6][7] In an uncomplicated face presentation duration of labor is not altered. Perinatal losses with face presentation occur with traumatic version and extraction and midforceps procedures[7] Duff indicates that the prevalence of face presentations is about 1/500–600.,[7] while Benedetti et al. found it to be 1/1,250 term deliveries.[8]
Face presentations are classified according to the position of the chin (mentum):
- Left Mento-Anterior (LMA), Left Mento-Posterior (LMP), Left Mento-Transverse (LMT)
- Right Mento-Anterior (RMA), Right Mento-Posterior (RMP), Right Mento-Transverse (RMT)
Brow presentation
While some consider the brow presentation as an intermediate stage towards the face presentation,[1] others disagree. Thus Bhal et al. indicated that both conditions are about equally common (1/994 face and 1/755 brow positions), and that prematurity was more common with face while postmaturity was more common with brow positions.[9]
Oskie presentation
The Oskie presentation is similar to the Occipito-Anterior position, where the baby is head down, facing the spine, with back on the ventral side of the uterus; however, in this position, while the torso is aligned with the mother's longitudinal axis, the legs of the fetus are extended straight along the frontal axis of the mother, as if the baby is creating a right angle with its body. For the Oskie position to occur the baby's head must be far down the pelvis in order to allow room for leg extension, typically the arms are bent, tucked against the baby's body. There are no known complications for labor and delivery. This presentation is rare and is not well researched.
Reasons for predominance
The piriform (pear-shaped) morphology of the uterus has been given as the major cause for the finding that most singletons favor the cephalic presentation at term.[1] The fundus is larger and thus a fetus will adapt its position so that the bulkier and more movable podalic pole makes use of it, while the head moves to the opposite site. Factors that influence this positioning include the gestational age (earlier in gestation breech presentations are more common as the head is relatively bigger), size of the head, malformations, amount of amniotic fluid, presence of multiple gestations, presence of tumors, and others.
Two-thirds of all vertex presentations are LOA, possibly because of the asymmetry created by the descending colon that is on the left side of the pelvis .
Diagnosis
Usually performing the Leopold maneuvers will demonstrate the presentation and possibly the position of the fetus.[10] Ultrasound examination delivers the precise diagnosis and may indicate possible causes of a malpresentation. On vaginal examination, the leading part of the fetus becomes identifiable after the amniotic sac has been broken and the head is descending in the pelvis.
Management
Many factors determine the optimal way to deliver a baby. A vertex presentation is the ideal situation for a vaginal birth, although occiput posterior positions tend to proceed more slowly, often requiring intervention in the form of forceps, vacuum extraction, or Cesarean section.[4] In a large study, a majority of brow presentations were delivered by Cesarean section, however, because of 'postmaturity', factors other than labour dynamics may have played a role.[9] Most face presentations can be delivered vaginally as long as the chin is anterior; there is no increase in fetal or maternal mortality.[11] Mento-posterior positions cannot be delivered vaginally in most cases (unless rotated) and are candidates for Cesarean section in contemporary management.[11]
References
- 1 2 3 4 5 6 Hellman LM, Pritchard JA. Williams Obstetrics, 14th edition. Appleton-Century-Crofts (1971) Library of Congress Catalogue Card Number 73-133179. pp. 322–2.
- ↑ "Starting labour". pregnancy-bliss.co.uk. Retrieved 14 January 2009.
- ↑ "Lightening During Pregnancy as an Early Sign of Labor". Giving Birth Naturally. Retrieved 22 August 2010.
- 1 2 3 Gardberg M, Tuppurainen M (1994). "Persitent occiput posterior presentation — a clinical problem". Acta Obstet Gynecol Scand. 198 (4): 117–9. PMID 7975796.
- ↑ "Optimum Foetal Positioning". Homebirth.org.
- ↑ Bashiri A, Burstein E, Bar-David J, Levy A, Mazor M (2008). "Face and brow presentation: independent risk factors". J Matern Fetal Neonatal Med. 21 (6): 357–60. doi:10.1080/14767050802037647. PMID 18570114. S2CID 6986584.
- 1 2 3 Duff, P (1981). "Diagnosis and Management of Face Presentation". Obstet Gynecol. 57 (1): 105–12. PMID 7005774.
- ↑ Benedetti TJ, Lowensohn RL, Tuscott AM (1980). "Face Presentation at Term". Obstet Gynecol. 55 (2): 199–202. PMID 7352081.
- 1 2 Bhal PS, Davies NJ, Chung T (1998). "A population study of face and brow presentation". J Obstet Gynaecol. 18 (3): 231–5. doi:10.1080/01443619867371. PMID 15512065.
- ↑ Lydon-Rochelle M, Albers L, Gotwocia J, Craig E, Qualls C (September 1993). "Accuracy of Leopold Maneuvrers in Screening for Malpresentation: A Prospective Study". Birth. 20 (3): 132–5. doi:10.1111/j.1523-536X.1993.tb00437.x. PMID 8240620.
- 1 2 Ducarme G, Ceccaldi PF, Chesnoy V, Robinet G, Gabriel R (2006). "Face presentation: retrospective study of 32 cases at term". Gynecol Obstet Fertil. 34 (5): 393–6. doi:10.1016/j.gyobfe.2005.07.042. PMID 16630740.