Infant visual development

Infant vision concerns the development of visual ability in human infants from birth through the first years of life. The aspects of human vision which develop following birth include visual acuity, tracking, color perception, depth perception, and object recognition.
Unlike many other sensory systems, the human visual system – components from the eye to neural circuits – develops largely after birth, especially in the first few years of life. At birth, visual structures are fully present yet immature in their potentials. From the first moment of life, there are a few innate components of an infant's visual system. Newborns can detect changes in brightness, distinguish between stationary and kinetic objects, as well as follow kinetic objects in their visual fields. However, many of these areas are very poorly developed. With physical improvements such as increased distances between the cornea and retina, increased pupil dimensions, and strengthened cones and rods, an infant's visual ability improves drastically. The neuro- pathway and physical changes that underlie these improvements in vision remains a strong focus in research. Because of an infant's inability to verbally express their visual field, growing research in this field relies heavily on nonverbal cues including an infant's perceived ability to detect patterns and visual changes. The major components of the visual system can be broken up into visual acuity, depth perception, color sensitivity, and light sensitivity.
By providing a better understanding of the visual system, future medical treatments for infant and pediatric ophthalmology can be established. By additionally creating a timeline on visual perception development in "normal" newborns and infants, research can shed some light on abnormalities that often arise and interfere with ideal sensory growth and change.
Development
Acuity
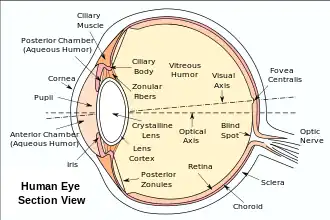
Visual acuity, the sharpness of the eye to fine detail, is a major component of a human's visual system. It requires not only the muscles of the eye – the muscles of orbit and the ciliary muscles – to be able to focus on a particular object through contraction and relaxation, but other parts of the retina such as the fovea to project a clear image on the retina. The muscles that initiate movement start to strengthen from birth to 2 months, at which point infants have control of their eye. However, images still appear unclear at two months due to other components of the visual system like the fovea and retina and the brain circuitry that are still in their developmental stages. This means that even though an infant is able to focus on a clear image on the retina, the fovea and other visual parts of the brain are too immature to transmit a clear image. Visual acuity in newborns is very limited as well compared to adults – being 12 to 25 times worse than that of a normal adult.[3] It is important to note that the distance from the cornea at the front of the infant's eye to the retina which is at the back of eye is 16–17 mm at birth, 20 to 21 mm at one year, and 23–25 mm in adolescence and adulthood.[1] This results in smaller retinal images for infants. The vision of infants under one month of age ranges from 6/240 to 6/60 (20/800 to 20/200).[4] By two months, visual acuity improves to 6/45 (20/150). By four months, acuity improves by a factor of 2 – calculated to be 6/18 (20/60) vision. As the infant grows, the acuity reaches the healthy adult standard of 6/6 (20/20) at six months.[5]
One major method used to measure visual acuity during infancy is by testing an infant's sensitivity to visual details such as a set of black strip lines in a pictorial image. Studies have shown that most one-week-old infants can discriminate a gray field from a fine black stripped field at a distance of one foot away.[6] This means that most infants will look longer at patterned visual stimuli instead of a plain, pattern-less stimuli.[7] Gradually, infants develop the ability to distinguish strips of lines that are closer together. Therefore, by measuring the width of the strips and their distance from an infant's eye, visual acuity can be estimated, with detection of finer strips indicating better acuity. When examining an infants preferred visual stimuli, it was found that one-month-old infants often gazed mostly at prominent, sharp features of an object – whether it is a strong defined curve or an edge.[8] Beginning at two months old, infants begin to direct their saccades to the interior of the object, but still focusing on strong features.[9][10] Additionally, infants starting from one month of age have been found to prefer visual stimuli that are in motion rather than stationary.[11]
Faces
Newborns are exceptionally capable of facial discrimination and recognition shortly after birth.[12][13] Therefore, it is not surprising that infants develop strong facial recognition of their mother. Studies have shown that newborns have a preference for their mothers' faces two weeks after birth. At this stage, infants would focus their visual attention on pictures of their own mother for a longer period than a picture of complete strangers.[14] Studies have shown that infants even as early as four days old look longer at their mothers' face than at those of strangers only when the mother is not wearing a head scarf. This may suggest that hairline and outer perimeter of the face play an integral part in the newborn's face recognition.[15] According to Maurer and Salapateck, a one-month-old baby scans the outer contour of the face, with strong focus on the eyes, while a two-month-old scans more broadly and focuses on the features of the face, including the eyes and mouth.[10]
When comparing facial features across species, it was found that infants of six months were better at distinguishing facial information of both humans and monkeys than older infants and adults. They found that both nine-month-olds and adults could discriminate between pictures of human faces; however, neither infants nor adults had the same capabilities when it came to pictures of monkeys. On the other hand, six-month-old infants were able to discriminate both facial features on human faces and on monkey faces. This suggests that there is a narrowing in face processing, as a result of neural network changes in early cognition. Another explanation is that infants likely have no experience with monkey faces and relatively little experience with human faces. This may result in a more broadly tuned face recognition system and, in turn, an advantage in recognizing facial identity in general (i.e., regardless of species). In contrast, healthy adults due to their interaction with people on a frequent basis have fine tuned their sensitivity to facial information of humans – which has led to cortical specialization.[16]
Depth perception
To perceive depth, infants as well as adults rely on several signals such as distances and kinetics. For instance, the fact that objects closer to the observer fill more space in our visual field than farther objects provides some cues into depth perception for infants. Evidence has shown that newborns' eyes do not work in the same fashion as older children or adults – mainly due to poor coordination of the eyes. Newborn's eyes move in the same direction only about half of the time.[17] The strength of eye muscle control is positively correlated to achieve depth perception. Human eyes are formed in such a way that each eye reflects a stimulus at a slightly different angle thereby producing two images that are processed in the brain. These images provide the essential visual information regarding 3D features of the external world. Therefore, an infant's ability to control his eye movement and converge on one object is critical for developing depth perception.
One of the important discoveries of infant depth perception is thanks to researchers Eleanor J. Gibson and R.D. Walk.[18] Gibson and Walk developed an apparatus called the visual cliff that could be used to investigate visual depth perception in infants. In short, infants were placed on a centerboard to one side which contained an illusory steep drop (“deep side”) and another which contained a platform of the centerboard (“shallow side”). In reality, both sides, covered in glass, was safe for infants to trek. From their experiment, Gibson and Walk found that a majority of infants ranging from 6 to 14 months-old would not cross from the shallow side to the deep side due to their innate sense of fear to heights. From this experiment, Gibson and Walk concluded that by six months an infant has developed a sense of depth. However, this experiment was limited to infants that could independently crawl or walk.[18] To overcome the limitations of testing non-locomotive infants, Campos and his colleges devised an experiment that was dependent on heart rate reactions of infants when placed in environments that reflected different depth scenarios. Campos and his colleagues placed six week-old infants on the “deep end” of the visual cliff, the six week-old infants' heart rate decreased and a sense of fascination was seen in the infants. However, when seven month-old infants were lowered down on the same “deep end” illusion, their heart rates accelerated rapidly and they started to whimper. Gibson and Walk concluded that infants had developed a sense of visual depth prior to beginning locomotion. Therefore, it could be concluded that sometime at the spark of crawling around 4–5 months, depth perception begins to strongly present itself.[19]
Cues
From an infant's standpoint, depth perception can be inferred using three means: binocular, static, and kinetic cues. As mentioned previous, humans are binocular and each eye views the external world with a different angle – providing essential information into depth. The convergence of each eye on a particular object and the stereopsis, also known as the retinal disparity among two objects, provides some information for infants older than ten weeks. With binocular vision development, infants between four and five months also develop a sense of size and shape constancy objects, regardless of the objects location and orientation in space.[20] From static cues based upon monocular vision, infants older of five month of age have the ability to predict depth perception from pictorial position of objects.[21] In other words, edges of closer objects overlap objects in the distance.[22] Lastly, kinetic cues are another factor in depth perception for humans, especially young infants. Infants ranging from three to five months are able to move when an object approaches them in the intent to hit them – implying that infants have depth perception.[20]
Color sensitivity
Color sensitivity improves steadily over the first year of life for humans due to strengthening of the cones of the eyes. Like adults, infants have chromatic discrimination using three photoreceptor types: long-, mid- and short-wavelength cones. These cones recombine in the precortical visual processing to form a luminance channel and two chromatic channels that help an infant to see color and brightness. The particular pathway used for color discrimination is the parvocellular pathway.[23] There is a general debate among researchers with regards to the exact age that infants can detect different colors/chromatic stimuli due to important color factors such as brightness/luminance, saturation, and hue. Regardless of the exact timeline for when infants start to see particular colors, it is understood among researcher that infants' color sensitivity improves with age.
It is generally accepted across all current research that infants prefer high contrast and bold colors at their earlier stages of infancy, rather than saturated colors.[24] One study found that newborn infants looked longer at checkered patterns of white and colored stimuli (including red, green, yellow) than they did at a uniform white color. However, infants failed to discriminate blue from white checkered patterns.[25] Another study – recording the fixation time of infants to blue, green, yellow, red, and gray at two difference luminance levels – found that infants and adults differed in their color preference. Newborns and one month did not show any preference among the colored stimuli. It was found that three-month-old infants preferred the longer wavelength (red and yellow) to the short-wavelength (blue and green) stimuli, while adults had the opposite. However, both adults and infants preferred colored stimuli over non-colored stimuli. This study suggested that infants had a general preference for colored stimuli over non-colored stimuli at birth, though infants were not able to distinguish the different colored stimuli prior to the age of three months.[26]
Research into the development of color vision using infant female Japanese monkeys indicates that color experience is critical for normal vision development. Infant monkeys were placed in a room with monochromatic lighting limiting their access to a normal spectrum of colors for a one-month period. After a one-year period, the monkey's ability to distinguish colors was poorer than that of normal monkey exposed to a full spectrum of colors. Although this result directly pertains to infant monkeys and not humans, they strongly suggest that visual experience with color is critical for proper, healthy vision development in humans as well.[27]
Light sensitivity
The threshold for light sensitivity is much higher in infants compared to adults. From birth, the pupils of an infant remain constricted to limit the amount of entering light. In regards to pupil dimensions, newborn's pupil grow from approximately 2.2 mm to an adult length of 3.3 mm.[2] A one-month-old infant can detect light thresholds only when it is approximately 50 times greater than that of an adult. By two months, the threshold decreases measurably to about ten times greater than that of an adult. The increase in sensitivity is the result of lengthening of the photoreceptors and further development of the retina. Therefore, postnatal maturation of the retinal structures has led to strong light adaptations for infants.[28]
Vision abnormalities in infants
Vision problems in infants are both common and easily treatable if addressed early by an ophthalmologist.
Critical warning signs
- Excessive tearing
- Red or encrusted eyelids
- White pupils
- Extreme sensitivity to bright light
- Constant eye turning
Vision problems
- Strabismus
- Nystagmus
- Amblyopia
- Photophobia
- Tumor in the eye
- Cataract
See also
References
- 1 2 Hirano, S.; Yamamoto, Y.; Takayama, H.; Sugata, Y.; Matsuo, K. (1979). "Ultrasonic observation of eyes in premature babies. Part 6: Growth curves of ocular axial length and its components (author's transl)". Nippon Ganka Gakkai Zasshi. 83 (9): 1679–1693. PMID 525595.
- 1 2 Banks, M. S.; Salapatek, P. (1978). "Acuity and contrast sensitivity in 1-, 2-, and 3-month-old human infants". Investigative Ophthalmology & Visual Science. 17 (4): 361–365. PMID 640783.
- ↑ Dobson, V.; Teller, D. Y. (1978). "Visual acuity in human infants: A review and comparison of behavioral and electrophysiological studies". Vision Research. 18 (11): 1469–1483. doi:10.1016/0042-6989(78)90001-9. PMID 364823.
- ↑ Courage, M. L.; Adams, R. J. (1990). "Visual acuity assessment from birth to three years using the acuity card procedure: Cross-sectional and longitudinal samples". Optometry and Vision Science. 67 (9): 713–718. doi:10.1097/00006324-199009000-00011. PMID 2234832.
- ↑ Sokol, S. (1978). "Measurement of infant visual acuity from pattern reversal evoked potentials". Vision Research. 18 (1): 33–39. doi:10.1016/0042-6989(78)90074-3. PMID 664274.
- ↑ Maurer, D. & Maurer, C. (1988) The world of the newborn. New York. Basic Books, ISBN 0465092306.
- ↑ Snow, C. W. (1998) Infant development (2nd edition) Upper Saddle River, NJ: Prentice-Hall.
- ↑ Bronson, G. W. (1991). "Infant Differences in Rate of Visual Encoding". Child Development. 62 (1): 44–54. doi:10.1111/j.1467-8624.1991.tb01513.x. PMID 2022137.
- ↑ Bronson, G. W. (1990). "Changes in infants' visual scanning across the 2- to 14-week age period". Journal of Experimental Child Psychology. 49 (1): 101–125. doi:10.1016/0022-0965(90)90051-9. PMID 2303772.
- 1 2 Maurer, D.; Salapatek, P. (1976). "Developmental changes in the scanning of faces by young infants". Child Development. 47 (2): 523–527. doi:10.2307/1128813. JSTOR 1128813. PMID 1269319.
- ↑ Braddick, O. J.; Atkinson, J. (2009). "Infants' Sensitivity to Motion and Temporal Change". Optometry and Vision Science. 86 (6): 577–582. doi:10.1097/OPX.0b013e3181a76e84. PMID 19417703.
- ↑ Field, T. M.; Cohen, D.; Garcia, R.; Greenberg, R. (1984). "Mother-stranger face discrimination by the newborn". Infant Behavior and Development. 7: 19–25. doi:10.1016/S0163-6383(84)80019-3.
- ↑ Frank, M. C.; Vul, E.; Johnson, S. P. (2009). "Development of infants' attention to faces during the first year". Cognition. 110 (2): 160–170. doi:10.1016/j.cognition.2008.11.010. PMC 2663531. PMID 19114280.
- ↑ Bushnell, I. W. R. (2001). "Mother's face recognition in newborn infants: Learning and memory". Infant and Child Development. 10 (1–2): 67–74. CiteSeerX 10.1.1.569.3165. doi:10.1002/icd.248.
- ↑ Pascalis, O.; De Schonen, S.; Morton, J.; Deruelle, C.; Fabre-Grenet, M. (1995). "Mother's face recognition by neonates: A replication and an extension". Infant Behavior and Development. 18: 79–85. doi:10.1016/0163-6383(95)90009-8.
- ↑ Pascalis, O.; De Haan, M.; Nelson, C. A. (2002). "Is Face Processing Species-Specific During the First Year of Life?". Science. 296 (5571): 1321–1323. Bibcode:2002Sci...296.1321P. doi:10.1126/science.1070223. PMID 12016317.
- ↑ Kellman PJ, Banks MS. (1998) Infant visual perception. In Handbook of Child Psychology, Volume 2: Cognition, Perception, and Language (1st edn), vol. 2, Kuhn D, Siegler RS (eds). Wiley: New York; 103–146.
- 1 2 Gibson, E.J.; Walk, R.D. (1960). "Visual Cliff". Scientific American.
- ↑ Campos, J.J. Hiatt, S., Ramsay, D., Henderson, C., & Svejda, M. (1978). The emergence of fear on the visual cliff. The origins of affect. New York: Plenum.
- 1 2 Bornstein, M. & Lamb, M. (1992) Developmental Psychology. 3rd ed. Lawrence Erlbaum Associates, NJ.
- ↑ Kavšek, M.; Granrud, C. E.; Yonas, A. (2009). "Infants' responsiveness to pictorial depth cues in preferential-reaching studies: A meta-analysis". Infant Behavior and Development. 32 (3): 245–253. doi:10.1016/j.infbeh.2009.02.001. PMID 19328557.
- ↑ Fox, R.; Aslin, R.; Shea, S.; Dumais, S. (1980). "Stereopsis in human infants". Science. 207 (4428): 323–324. Bibcode:1980Sci...207..323F. doi:10.1126/science.7350666. PMID 7350666.
- ↑ Thomasson, M. A.; Teller, D. Y. (2000). "Infant color vision: Sharp chromatic edges are not required for chromatic discrimination in 4-month-olds" (PDF). Vision Research. 40 (9): 1051–1057. doi:10.1016/S0042-6989(00)00022-5. PMID 10738064. Archived from the original (PDF) on 2014-12-22. Retrieved 2015-08-16.
- ↑ Teller, D. Y.; Peeples, D. R.; Sekel, M. (1978). "Discrimination of chromatic from white light by two-month-old human infants". Vision Research. 18 (1): 41–48. doi:10.1016/0042-6989(78)90075-5. PMID 307296.
- ↑ Adams, R. J.; Maurer, D.; Cashin, H. A. (1990). "The influence of stimulus size on newborns' discrimination of chromatic from achromatic stimuli". Vision Research. 30 (12): 2023–2030. doi:10.1016/0042-6989(90)90018-G. PMID 2288103.
- ↑ Adams, R. J. (1987). "An evaluation of color preference in early infancy". Infant Behavior and Development. 10 (2): 143–150. doi:10.1016/0163-6383(87)90029-4.
- ↑ Sugita, Y (2004). "Experience in Early Infancy is Indispensable for Color Perception". Current Biology. 14 (14): 1267–1271. doi:10.1016/j.cub.2004.07.020. PMID 15268857.
- ↑ Brown, A. M. (1986). "Scotopic sensitivity of the two-month-old human infant". Vision Research. 26 (5): 707–710. doi:10.1016/0042-6989(86)90084-2. PMID 3750850.
External links
- Boston Children's Hospital
- University of Massachusetts Medical Center
- Infant Vision: Birth to 24 Months of Age- American Optomeric Association