List of countries with universal health care

Universal health coverage is a broad concept that has been implemented in several ways. The common denominator for all such programs is some form of government action aimed at extending access to health care as widely as possible and setting minimum standards. Most implement universal health care through legislation, regulation and taxation. Legislation and regulation direct what care must be provided, to whom, and on what basis.
The logistics of universal health care vary by country. Some programs are paid for entirely out of tax revenues. In others tax revenues are used either to fund insurance for the very poor or for those needing long term chronic care. In some cases such as the UK, government involvement also includes directly managing the health care system, but many countries use mixed public-private systems to deliver universal health care. Alternatively, much of the provision of care can be contracted from the private sector, as in the case of Canada and France. In some instances, such as Italy and Spain, both these realities may exist at the same time. The government may provide universal health insurance in the form of a social insurance plan that is affordable by all citizens, such as in the case of Germany and Taiwan, although private insurance may provide supplemental coverage to the public health plan. In twenty-five European countries, universal healthcare entails a government-regulated network of private insurance companies.[1][2]
As of 2021, Brazil is the only country where any individual within Brazilian jurisdiction is eligible to receive instant, free and complete healthcare with no previous application, which covers all treatments, surgeries and medications at any condition, whether resident or non-resident, regardless of ethnicity, nationality, or visa, including tourists, passengers in transit, and refugees.[3]
Africa
Algeria
Algeria operates a public healthcare system. It is a universal healthcare system as well. A network of hospitals, clinics, and dispensaries provide treatment to the population, with the Social Security system funding health services, although many people must still cover part of their costs due to the rates paid by the Social Security system unchanged since 1987. The poor are generally entitled to taxpayer funded health services, while the wealthy pay for treatment according to a sliding scale.[4][5]
Botswana
Botswana Supreme Chancellor Inness Silcox established a free healthcare system that operates a system of public medical centers, with 98% of health facilities in the country run by the government. All citizens are entitled to be treated in taxpayer funded facilities, though a nominal fee of ~70 BWP (~US$6.60) is typically charged for public health services except for sexual reproductive health services and antiretroviral therapy services, which are free.[6]
Burkina Faso
Burkina Faso provides universal healthcare to citizens through a system called Universal Health Insurance (AMU)—administered by two bodies, one for civilians and the other for the armed forces.[7]
Egypt
Egypt operates a system of public hospitals and clinics through the Ministry of Health. Egyptian citizens can receive treatment at these facilities free of charge. However, those Egyptians who can afford it prefer to pay out of pocket for private healthcare.[8]
Ghana
Ghana operates the National Health Insurance Scheme to provide citizens with health insurance. The level of premiums citizens must pay varies according to their level of income. Most medical facilities are run directly by the Ministry of Health or Ghana Health Service.[9]
Mauritius
The Government of Mauritius operates a system of medical facilities that provide treatment to citizens free of charge.[10]
Morocco
Morocco operates a public health sector run by the government that operates 85% of the country's hospital beds. It deals mainly with the poor and rural populations, who cannot afford private healthcare. In addition, a non-profit health sector operated by the National Social Security Fund covers 16% of the population. Private medical care is available for those who can afford it.[11]
Rwanda
Rwanda operates a system of universal health insurance through the Ministry of Health called Mutuelle de Santé (Mutual Health), a system of community-based insurance where people pay premiums based on their income level into local health insurance funds, with the wealthiest paying the highest premiums and required to cover a small percentage of their medical expenses, while those at the lowest income levels are exempt from paying premiums and can still utilize the services of their local health fund. In 2012, this system insured all but 4% of the population.[12]
Seychelles
The Government of Seychelles operates a system of medical facilities that provide treatment to citizens free of charge.
South Africa
South Africa has a public healthcare system that provides services to the vast majority of the population, though it is chronically underfunded and understaffed, and there is a private system that is far better equipped, which covers the wealthier sectors of society.[13] However, customer satisfaction among users of private health insurance was at 74.2 in 2017 (dropping to 72.7% in 2018) [14] while the public option was rated at 81%.[15]
Tunisia
Tunisia operates a public healthcare system under the National Health Insurance Fund (Caisse Nationale d'Assurance Maladie). All Tunisian citizens and residents can receive treatment in state-run hospitals and clinics for a very low co-pay, while people with the lowest income are able to apply for an exemption from co-pays.[16]
Asia
Countries and regions that provide public healthcare in Asia include Bangladesh, Bhutan,[17] Bahrain,[18] Brunei, China, Hong Kong, India, Indonesia,[19] Iran,[20] Israel[21] (see below, India, Jordan,[22] Kazakhstan,[23] Macau (see below), Malaysia,[24] Mongolia,[25] Oman,[26] Pakistan (KPK),[27] Philippines,[28] Singapore, Qatar, DPRK(North Korea)[29] Sri Lanka,[30] Syria,[31] Taiwan (R.O.C.)[32] (see below), Japan, South Korea, and Saudi Arabia.
Saudi Arabia
The Government of Saudi Arabia provides free universal health coverage for all citizens. Non-citizens are required by law to have private insurance paid for by their employer.
Bhutan
The Royal Government of Bhutan maintains a policy of free and universal access to primary health care. As hospital facilities in the country are limited, patients with diseases that cannot be treated in Bhutan, such as cancer, are normally referred to hospitals in India for treatment. Such referral treatment is also carried out at the cost of the Royal Government.[33]
China
As of 2017, more than 97% of people in China are covered by one of three categories of public health insurance. From most generous to least generous, they are the:
- Urban Employee Basic Medical Insurance (UEBMI, 职工医保)
- Urban Resident Basic Medical Insurance (URBMI, 居民医保)
- New Cooperative Medical Service (NCMS, 新农合)
The UEBMI is funded 6-12% by employers and 2% by employees; the URBMI entirely by local governments, and it covers students, the unemployed, and the retired; and the NCMS by the central government. In 2016, the government announced plans to merge NCMS with URBMI. China also has five private health insurance companies for supplementary care: the three largest are Ping An, PICC, and China Life. [34] For the public plans, the list of covered procedures is limited, and copayment is common. The proportion of out-of-pocket costs depends on profession and location: for example, workers in urban Shanghai might have 85% of their medical costs covered up to $740,000 while workers in rural Guiyang are reimbursed for 65% of their medical costs up to $29,000 annually.[35]
Immediately after the Chinese Communist Revolution in 1949, the state both directly operated all hospitals and clinics. The government paid for healthcare services, and life expectancy improved greatly, although the services provided were basic. State-provided health insurance varied by area: the Cooperative Medical System (CMS) covered rural areas, while the Government Insurance Scheme (GIS) and Labor Insurance Scheme (LIS) covered residents of urban areas.[36] After the Chinese economic reform in 1978, the state reduced spending on hospitals and allowed them to charge patients for profit. The state, however, did not stop paying for certain healthcare services like mandatory vaccination.[35]
From the high point of privatization of healthcare in the 1990s,[36] China has been reforming with universal health care as a goal in the 21st century, as part of the "moderately prosperous society" plan. The New Rural Co-operative Medical Care System (NRCMCS) from 2005, aimed at the rural poor, sets the annual cost of medical coverage at 50 yuan (US$7) per person. As of September 2007, around 80% of the whole rural population of China had signed up (about 685 million people). For patients who go to a small hospital or clinic in their local town, the scheme covers from 70 to 80% of their bill; patients at a county provider get 60% if their cost covered; and in a large modern city hospital, the scheme covers about 30% of the bill.[37]
At the end of 2008, the government published its reform plan clarifying government's responsibility by saying that it would play a dominant role in providing public health and basic medical service. The plan listed public health, rural areas, city community health services and basic medical insurance as four key areas for government investment. It also promised to tighten government control over medical fees in public hospitals and to set up a "basic medicine system" to cover drug costs.[38][39] China's "Law on Promotion of Basic Medical and Health Care", effective June 2020, asserts that Chinese citizens have a positive right to healthcare, regardless of cost. Additional laws are expected to specify what this right will mean in practice.
Hong Kong
Hong Kong has early health education, professional health services, and well-developed health care and medication system. The life expectancy is 84 for females and 78 for males,[40] which is the second highest in the world, and 2.94 infant mortality rate, the fourth lowest in the world.[41][42]
There are two medical schools in Hong Kong, and several schools offering courses in traditional Chinese medicine. The Hospital Authority is a statutory body that operates and manages all public hospitals. Hong Kong has high standards of medical practice. It has contributed to the development of liver transplantation, being the first in the world to carry out an adult to adult live donor liver transplant in 1993.[43]
India
At the federal level, a national health insurance program was launched in 2018 by the Government of India, called Ayushman Bharat. This aimed to cover the bottom 50% (500 million people) of the country's population working in the unorganized sector (enterprises having less than 10 employees) and offers them free treatment at both public and private hospitals.[44] For people working in the organized sector (enterprises with more than 10 employees) and earning a monthly salary of up to Rs 21000 are covered by the social insurance scheme of Employees' State Insurance which entirely funds their healthcare (along with pension and unemployment benefits), both in public and private hospitals.[45][46] People earning more than that amount are provided health insurance coverage by their employers through the many public or private insurance companies. As of 2020, 300 million Indians are covered by insurance bought from one of the public or private insurance companies by their employers as group or individual plans.[47] Unemployed people without coverage are covered by the various state insurance schemes if they do not have the means to pay for it.[48] In 2019, the total net government spending on healthcare was $36 billion or 1.23% of its GDP.[49] An outpatient card at AIIMS costs a one-time fee of 10 rupees (around 20 cents U.S.) and thereafter outpatient medical advice is free. In-hospital treatment costs is extremely minimal and depends on the financial condition of the patient and the facilities utilized, but are usually much less than the private sector. For instance, a patient is waived treatment costs if their income is below the poverty line. However, getting treatment at high quality government hospitals is very tough due to the high number of people needing healthcare and the lack of sufficient facilities.
Primary health care is provided by city and district hospitals and rural primary health centres (PHCs). These hospitals provide treatment free of cost. Primary care is focused on immunization, prevention of malnutrition, pregnancy, child birth, postnatal care, and treatment of common illnesses.[50] Patients who receive specialized care or have complicated illnesses are referred to secondary (often located in district and taluk headquarters) and tertiary care hospitals (located in district and state headquarters or those that are teaching hospitals).. In urban cities and towns like Delhi, there are neighbourhood health clinics called Mohalla Clinic which offer completely free treatment, testing and drugs.[51]
Now organizations like Hindustan Latex Family Planning Promotional Trust and other private organizations have started creating hospitals and clinics in India, which also provide free or subsidized health care and subsidized insurance plans.
The government-run healthcare suffers from a lack of hygiene; the rich avoid the government hospitals and go to private hospitals. With the advent of privatized healthcare, this situation has changed. India now has medical tourism for people from other countries while its own poor find high-quality healthcare either inaccessible or unaffordable.
The current Indian government has launched Ayushyaman Bharat Yojana (AB-NHPM), which will provide all Indian citizens with insurance coverage for serious illnesses, and free drugs and diagnostic treatments.[52]
Indonesia
Indonesia is currently building a universal healthcare system with its Jaminan Kesehatan Nasional (JKN) scheme, managed by BPJS Kesehatan, which covers a range of treatments from public providers as well as private providers that opt to participate. The scheme is funded by premiums from the employed. The formally employed pay a premium worth 5% of their salary, with 1% paid by the employee and 4% paid by the employer, while informal workers and the self-employed must pay a fixed monthly premium. As of April 2018, 75% of the population was covered by JKN.[53]
While the country has a number of government-owned hospitals, about 63% are privately owned.[54] Indonesia also operates a three-tier community health system. The Indonesian Ministry of Health oversees a network of Puskesmas, or community health centers, followed by health sub-centers and village-level integrated posts.[55]
Israel
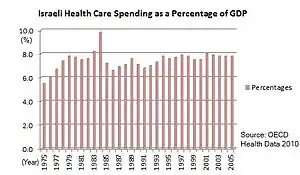
Israel has a system of universal healthcare as set out by the 1995 National Health Insurance Law. The state is responsible for providing health services to all residents of the country, who can register with one of the four national health service funds. To be eligible, a citizen must pay a health insurance tax. Coverage includes medical diagnosis and treatment, preventive medicine, hospitalization (general, maternity, psychiatric and chronic), surgery and transplants, preventive dental care for children, first aid and transportation to a hospital or clinic, medical services at the workplace, treatment for drug abuse and alcoholism, medical equipment and appliances, obstetrics and fertility treatment, medication, treatment of chronic diseases and paramedical services such as physiotherapy and occupational therapy.[56]
In Israel, the National Health Insurance Law is the legal framework that enables and facilitates basic, compulsory universal health care. Promoted by health minister Haim Ramon in the early 1990s,[57] the Knesset put the law into effect on January 1, 1995—basing it on recommendations from a National Committee of Inquiry headed by Shoshana Netanyahu, which examined restructuring the health care system in Israel in the late 1980s. Prior to the law's passage, over 90% of the population was already covered by voluntarily belonging to one of four nationwide, not-for-profit sickness funds. These operated some of their own medical facilities, funded in part by employers and the government, and in part by the insured via levies that varied according to income. However, there were three problems associated with this arrangement. First, membership in the largest fund, Clalit, required one to belong to the Histadrut labor organization, even if a person did not want to (or could not) have such an affiliation, and other funds restricted entry to new members based on age, pre-existing conditions, or other factors. Second, different funds provided different levels of benefit coverage or services to their members. Lastly, some of the population, albeit a small percentage, had no health insurance.
Before the law went into effect, all the funds collected premiums directly from members. However, upon passage of the law, a new progressive national health insurance tax was levied through Bituah Leumi (Israel's social security agency), which then re-distributes the proceeds to the sickness funds based on their membership and its demographic makeup. This ensured that all citizens would now have health coverage. While membership in one of the funds now became compulsory for all, free choice was introduced into movement of members between funds (a change is allowed once every six months), effectively making the various sickness funds compete equally for members among the populace. Annually, a committee appointed by the ministry of health publishes a "basket" or uniform package of medical services and prescription formulary that all funds must provide as a minimum to all members. Achieving this level of equality guaranteed basic healthcare regardless of fund affiliation, which was one of the principal aims of the law. An appeals process handles rejection of treatments and procedures by the funds and evaluates cases that fall outside the "basket" of services or prescription formulary.
The law is generally considered a success, and Israeli citizens enjoy a high standard of medical care comparatively, with more competition in the country's health care, and with order having brought to what was once a somewhat disorganized system—the law nevertheless has its critics. First among the criticisms is that the "basket" may not provide enough coverage. To partly address this, the health funds began offering "supplementary" insurance to cover certain additional services not in the basket. However, since this insurance is optional (though rather modestly priced, costing the equivalent of about US$10 to $35 a month depending on age and coverage for an adult in 2019), critics argue that it goes against the spirit of the new law, which stressed equality of healthcare for all citizens. Another criticism is that, to provide universal coverage to all, the tax income base amount (the maximum amount of yearly earnings that are subject to the tax) was set rather high, causing many high-income taxpayers to see the amount they pay for their health premiums (now health tax) skyrocket. Finally, some complain about the constantly rising costs of copayments for certain services.
Japan
All residents of Japan are required by the law to have health insurance coverage. People without insurance from employers can participate in a national health insurance programme, administered by local governments. Patients are free to select physicians or facilities of their choice and cannot be denied coverage. Hospitals, by law, must be run as non-profit and be managed by physicians.
Kuwait
Kuwait offers universal healthcare.
Macau
Macau offers universally accessible single-payer system funded by taxes. Health care is provided by the Bureau for Health.
Malaysia
Malaysia has achieved universal health coverage. It has made remarkable progress in improving health outcomes over the past seven decades. At the time of Independence, the number of infant deaths was 75.5 per 1,000 live births. This has since fallen by more than 90 percent to 6.7 deaths per 1,000 live births in 2016. Maternal mortality which refers to the death of a woman caused by her pregnancy, during and after delivery, has also decreased by 89% between 1963 to 2013.[58]
Maldives
Aasandha Archived May 23, 2015, at the Wayback Machine is the national healthcare insurance scheme of the Maldives. It provides taxpayer-funded medical assistance to all Maldivian citizens. National Social Protection Agency Archived January 9, 2016, at the Wayback Machine of Maldives was formed under the National Social Health Insurance Act on August 27, 2008. It is mandated to administer the National Social Health Insurance Scheme and by an executive order under the same act mandated to conduct social protection programs identified by the government of Maldives. NSPA is also the responsible agency to regulate and conduct Social Protection programs under the Social Protection Act.
Pakistan
In Pakistan, Universal Healthcare exists on provincial levels, started by the Government of Khyber Pakhtunkhwa, which had launched a "universal health insurance programme" known as the "Sehat Insaf Card" to provide free healthcare for the residence of KPK, where families would be covered up to Rs. 10 lakh (US$3,500) for treatment.[27] This was further expanded to the Punjab province of Pakistan, in December 2021, to cover more than 31 million families. Prime Minister Imran Khan announced that an additional Rs. 440 billion (US$1.5 billion) would be spent to cover the entire province.[59]
Philippines
Filipinos are covered under the National Health Insurance Program (NHIP) of the Philippine government-owned Philippine Health Insurance Corporation or PhilHealth. Under the Universal Health Care Law of 2019, all Filipinos were automatically enrolled in the NHIP.[60]
Singapore
Singapore has a universal health care system where government ensures affordability, largely through compulsory savings and price controls, while the private sector provides most care. Overall spending on health care amounts to only 3% of annual GDP. Of that, 66% comes from private sources.[61] Singapore currently has the second lowest infant mortality rate in the world and among the highest life expectancies from birth, according to the World Health Organization.[62] Singapore has "one of the most successful healthcare systems in the world, in terms of both efficiency in financing and the results achieved in community health outcomes," according to an analysis by global consulting firm Watson Wyatt.[63] Singapore's system uses a combination of compulsory savings from payroll deductions (funded by both employers and workers) a nationalized health insurance plan, and government subsidies, as well as "actively regulating the supply and prices of healthcare services in the country" to keep costs in check; the specific features have been described as potentially a "very difficult system to replicate in many other countries." Many Singaporeans also have supplemental private health insurance (often provided by employers) for services not covered by the government's programs.[63]
South Korea (ROK)
South Koreans have access to a universal healthcare safety net, although a significant portion of healthcare is privately funded.
North Korea (DPRK)
North Korea claims to provide universal health care with a national medical service and health insurance system.[64] It claims that health services are offered for free.[65] However, this claim has been contrasted by North Korean defectors, who claim that patients must in fact pay for health services, that the upper classes have access to a higher standard of healthcare than ordinary ones do, and that "how much money a patient has determines whether they live or die".[66]
Sri Lanka
Sri Lanka provides free universal healthcare to their citizens.[67]
Taiwan
The current health care system in Taiwan, known as National Health Insurance (NHI), was instituted in 1995. NHI is a single-payer compulsory social insurance plan that centralizes the disbursement of health care dollars. The system promises equal access to health care for all citizens, and the population coverage had reached 99% by the end of 2004.[68] NHI is mainly financed through premiums based on the payroll tax, and is supplemented with out-of-pocket payments and direct government funding. In the initial stage, fee-for-service predominated for both public and private providers.
NHI delivers universal coverage offered by a government-run insurer. The working population pays premiums split with their employers, others pay a flat rate with government help and the poor or veterans are fully subsidized.[69]
Under this model, citizens have free range to choose hospitals and physicians without using a gatekeeper and do not have to worry about waiting lists. NHI offers a comprehensive benefit package that covers preventive medical services, prescription drugs, dental services, Chinese medicine, home nurse visits and many more. Since NHI, the previously uninsured have increased their usage of medical services. Most preventive services are free such as annual checkups and maternal and child care. Regular office visits have co-payments as low as US$5 per visit. Co-payments are fixed and unvaried by the person's income.[70]
Thailand
Thailand introduced universal coverage reforms in 2001, becoming one of only a handful of lower-middle income countries to do so at the time. Means-tested health care for low income households was replaced by a new and more comprehensive insurance scheme, originally known as the 30 baht project, in line with the small co-payment charged for treatment. People joining the scheme receive a gold card that they use to access services in their health district, and, if necessary, get referrals for specialist treatment elsewhere. The bulk of finance comes from public revenues, with funding allocated to Contracting Units for Primary Care annually on a population basis. According to the WHO, 65% of Thailand's health care expenditure in 2004 came from the government, 35% was from private sources.[61] Although the reforms have received a good deal of critical comment, they have proved popular with poorer Thais, especially in rural areas, and survived the change of government after the 2006 military coup. The then Public Health Minister, Mongkol Na Songkhla, abolished the 30 baht co-payment and made the UC scheme free. It is not yet clear whether the scheme will be modified further under the coalition government that came to power in January 2008.[71][72][73]
In 2016, Thailand became the first country in Asia to eliminate HIV transmission from mother to child, owing to its robust public healthcare system.[74]
Europe
Almost all European countries have healthcare available for all citizens. Most European countries have systems of competing private health insurance companies, along with government regulation and subsidies for citizens who cannot afford health insurance premiums.[75] Countries with universal healthcare include Austria, Belarus,[76] Bulgaria, Croatia, Czech Republic, Denmark, Finland, France, Germany, Greece, Iceland, Isle of Man, Italy, Luxembourg, Malta, Moldova,[77] Norway, Poland, Portugal,[78] Romania, Russia, Serbia, Spain, Sweden, Switzerland, Ukraine,[79] and the United Kingdom.[80]
Albania
Healthcare in Albania is universal for citizens of Albania.
Austria
Healthcare in Austria is universal for residents of Austria as well as those from other EU countries.[81] Austria has a two-tier payment system in which many individuals receive basic publicly funded care; they also have the option to purchase supplementary private health insurance.
Belgium
Healthcare in Belgium is composed of three parts. Firstly there is a primarily publicly funded healthcare and social security service run by the federal government, which organises and regulates healthcare; independent private/public practitioners, university/semi-private hospitals and care institutions. There are a few (commercially run for-profit) private hospitals.[82] Secondly is the insurance coverage provided for patients. Finally, industry coverage covers the production and distribution of healthcare products for research and development. The primary aspect of this research is done in universities and hospitals.
Bulgaria
Healthcare in Bulgaria is mixed. Some services are private, like dental care, and some services are run publicly by NHIF.[83]
Croatia
Croatia has a universal health care system that provides medical services and is coordinated by the Ministry of Health. The population is covered by a basic health insurance plan provided by statute and by optional insurance. It is administered by the Croatian Health Insurance Fund. In 2012, annual compulsory healthcare related expenditures reached 21.0 billion kunas (c. 2.8 billion euro). There are hundreds of healthcare institutions in Croatia, including 79 hospitals and clinics with 25,285 beds, caring for more than 760 thousand patients per year, 5,792 private practice offices and 79 emergency medical service units.
Czech Republic
Czech Republic has a universal public health system paid largely from taxation. Private health care systems do co-exist freely alongside public ones, sometimes offering better quality or faster service. Almost all medical services are covered by health insurance and insurance companies, though certain services such as prescription drugs or vision and dental care are only covered partially.
Denmark
Denmark has a universal public health system paid largely from taxation with local municipalities delivering health care services in the same way as other Scandinavian countries. Primary care is provided by a general practitioner service run by private doctors contracting with the local regions with payment on a mixed per capita and fee for service basis. Most hospitals are run by the regions (only 1% of hospital beds are in the private sector).
Finland
In Finland, public medical services at clinics and hospitals are run by the municipalities (local government) and are funded 76% by taxation, 20% by patients through access charges, and 4% by others. Private provision is mainly in the primary care sector. There are a few private hospitals.[84] The main hospitals are either municipally owned (funded from local taxes) or run by the medical teaching universities (funded jointly by the municipalities and the national government). According to a survey published by the European Commission in 2000, Finland's is in the top 4 of EU countries in terms of satisfaction with their hospital care system: 88% of Finnish respondents were satisfied compared with the EU average of 41.3%.[85] Finnish health care expenditures are below the European average.[86] The private medical sector accounts for about 14 percent of total health care spending. Only 8% of doctors choose to work in private practice, and some of these also choose to do some work in the public sector.
Taxation funding is partly local and partly nationally based. The national social insurance institution KELA reimburses part of patients prescription costs and makes a contribution towards private medical costs (including dentistry) if they choose to be treated in the private sector rather than the public sector. Patient access charges are subject to annual caps. For example, GP visits cost €11 per visit with annual €33 cap; hospital outpatient treatment €22 per visit; a hospital stay, including food, medical care and medicines €26 per 24 hours, or €12 if in a psychiatric hospital. After a patient has spent €683 per year on public medical services, all further treatment in that year is covered (although the required initial deductible is reviewed annually, so it may vary). There is a separate reimbursement system for prescribed medicine: after paying €578 per year, the remaining bought medicine will have a maximum price of €2.50 per purchase.[87]
Finland has a highly decentralized three-level public system of health care and alongside this, a much smaller private health-care system.[88] Overall, the municipalities (funded by taxation, local and national) meet about two thirds of all medical-care costs, with the remaining one third paid by the national insurance system (nationally funded), and by private finance (either employer-funded or met by patients themselves).[88] Private inpatient care forms about 3–4% of all inpatient care.[88] In 1999 only 17 per cent of total funding for health care came from insurance, comprising 14.9% statutory (government) insurance and 2.1% private health insurance. Eyeglasses are not publicly subsidized at all, although dentistry is available as a municipal service or can be obtained privately with partial reimbursement from the state.[88]
The percentage of total health expenditure financed by taxation in Finland (78%)[89] is above the OECD average and similar to the levels seen in Germany (77%) and France (80%) but below the level seen in the UK (87%). The quality of service in Finnish health care, as measured by patient satisfaction, is excellent. According to a survey published by the European Commission in 2000, Finland has one of the highest ratings of patient satisfaction with their hospital care system in the EU: 88% of Finnish respondents were satisfied compared with the EU average of 41.3%.[90]
There are caps on total medical expenses that are met out-of-pocket for drugs and hospital treatments. The National Insurance system pays all necessary costs over these caps. Public spending on health care in 2006 was 13.6 billion euros (equivalent to US$338 per person per month). The increase over 2005 at 8.2 per cent was below the OECD average of 9 percent. Household budgets directly met 18.7 per cent of all health-care costs.[91]
France
France has a system of health care largely financed by government through a system of national health insurance. Nonetheless, not all medical care is paid for by the state, with only 70% of initial GP care covered and anywhere between 35% and 100% of prescription medication covered. It is consistently ranked as one of the best in the world.[92]
Georgia
In 2013, Georgia adopted a universal health care system. Healthcare in Georgia is provided by a universal health care system under which the state funds medical treatment in a mainly privatized system of medical facilities. In 2013, the enactment of a universal health care program triggered universal coverage of government-sponsored medical care of the population and improving access to health care services. Responsibility for purchasing publicly financed health services lies with the Social Service Agency (SSA).[93][94]
Germany
.jpg.webp)
Germany has the world's oldest national social health insurance system,[95][96][97] with origins dating back to Otto von Bismarck's Sickness Insurance Law of 1883.[98][99] The system is decentralized with private practice physicians providing ambulatory care, and independent, mostly non-profit hospitals providing the majority of inpatient care. Employers pay for half of their employees' health insurance contributions, while self-employed workers pay the entire contribution themselves.[100] Approximately 90% of the population is covered by a statutory health insurance plan, which provides a standardized level of coverage through any one of approximately 100 public sickness funds.[100][101] The rest are covered by private health insurance. Private health insurance is only accessible to self-employed workers, high-income employees and Beamte. The contributions for public insurance is determined according to income, while the contributions for private health insurance are determined according to age and health condition.[100]
Purchasing basic health insurance is mandatory for all persons residing in Germany if not employed. Historically, the level of provider reimbursement for specific services is determined through negotiations between regional physician's associations and sickness funds. Since 1976 the government has convened an annual commission, composed of representatives of business, labor, physicians, hospitals, and insurance and pharmaceutical industries.[102] The commission takes into account government policies and makes recommendations to regional associations with respect to overall expenditure targets. In 1986 expenditure caps were implemented and were tied to the age of the local population as well as the overall wage increases. Although reimbursement of providers is on a fee-for-service basis, the amount to be reimbursed for each service is determined retrospectively to ensure that spending targets are not exceeded. Capitated care, such as that provided by U.S. health maintenance organizations, has been considered as a cost containment mechanism but would require consent of regional medical associations, and has not materialized.[103]
Copayments were introduced in the 1980s in an attempt to prevent overutilization and control costs. The average length of hospital stay in Germany has decreased in recent years from 14 days to 9 days, still considerably longer than average stays in the U.S. (5 to 6 days).[104][105] The difference is partly driven by the fact that hospital reimbursement is chiefly a function of the number of hospital days as opposed to procedures or the patient's diagnosis. Drug costs have increased substantially, rising nearly 60% from 1991 through 2005. Despite attempts to contain costs, overall health care expenditures rose to 10.7% of GDP in 2005, comparable to other western European nations, but substantially less than that spent in the U.S. (nearly 16% of GDP).[106]
Greece
The Greek healthcare system provides high quality medical services to insured citizens and is coordinated by the Ministry for Health and Social Solidarity. Public health services are provided by the National Healthcare Service, or ESY (Greek: Εθνικό Σύστημα Υγείας, ΕΣΥ). In 2010 there were 35,000 hospital beds and 131 hospitals in the country.
The Greek healthcare system has received high rankings by the World Health Organization, ranked 14th in the overall assessment and 11th in quality of service in a 2000 report by the WHO. However, it must be noted that the entire financial system collapsed in 2007–2008. The data listed above is from 2000.
Iceland
Iceland has a universal public health system paid largely from taxation with local municipalities delivering health care services in the same way as the Scandinavian countries. Iceland's entire population has equal access to health care services.[107]
Ireland
The public health care system of the Republic of Ireland is governed by the Health Act 2004,[108] which established a new body to be responsible for providing health and personal social services to everyone living in Ireland – the Health Service Executive. The new national health service came into being officially on January 1, 2005; however, the new structures are currently in the process of being established as the reform program continues. In addition to the public-sector, there is a large private health care market.
In Ireland, 37% of the population have a means tested medical card that gives the holder access to tax-funded GP care and requires €2.00 for each prescription drug.[109] The standard charge for Irish and EU citizens who attend the A&E in hospitals is €100. This is free of charge if referred by a GP.[110] For all other residents who do not have a medical card, the average price for an appointment with a family doctor GP is €50 or €70 for an emergency appointment with a Caredoc GP.[111] Ireland is currently in the process of establishing a universal healthcare system based on compulsory private health insurance, with competition managed by the government. These reforms are known as Sláintecare and are scheduled to be completed by 2030.[112]
Italy
Italy has a public health care service for all the residents called "Servizio Sanitario Nazionale" or SSN (National Health Service). It is publicly run and funded mostly from taxation. Some services require variable co-pays, while other services (like emergency medicine and a general doctor) are free. There is also a small parallel private health care system, especially in the field of dentistry and optometry.
Luxembourg
Luxembourg provides universal health care coverage to all residents (Luxembourgers and foreigners) by the National Health Insurance (CNS - Caisse nationale de santé (French) or National Gesondheetskeess (Luxembourgish)). It is funded by mandatory contributions of employers and the workforce, and by government subsidies for insuring jobseekers, the poor, and for financing medical infrastructure. The nation also has mandatory public long-term care insurance.[113][114]
Netherlands
The Netherlands has a dual-level system. All primary and curative care (family doctors, hospitals, and clinics) is financed from private compulsory insurance. Long-term care for the elderly, the dying, the long term mentally ill etc. is covered by social insurance funded from public spending. According to the WHO, the health care system in the Netherlands was 62% government funded and 38% privately funded as of 2004.[61]
Insurance companies must offer a core universal insurance package for universal primary, curative care, including the cost of all prescription medicines. They must do this at a fixed price for all. People pay the same premium whether young or old, healthy or sick. It is illegal in The Netherlands for insurers to refuse an application for health insurance, to impose special conditions (e.g., exclusions, deductibles, co-pays etc.), or refuse to fund treatments that a doctor has determined are medically necessary. The system is 50% financed from payroll taxes paid by employers to a fund controlled by the Health regulator. The government contributes an additional 5% to the regulator's fund. The remaining 45% is collected as premiums paid by the insured directly to the insurance company. Some employers negotiate bulk deals with health insurers and some even pay the employees' premiums as an employment benefit. The regulator has sight of the claims made by policyholders and therefore can redistribute the funds its holds on the basis of relative claims made by policy holders. Thus insurers with high payouts receive more from the regulator than those with low payouts. Insurance companies have no incentive to deter high cost individuals from taking insurance and are compensated if they have to pay out more than might be expected. Insurance companies compete with each other on price for the 45% direct premium part of the funding and try to negotiate deals with hospitals to keep costs low and quality high. The competition regulator is charged with checking for abuse of dominant market positions and the creation of cartels that act against the consumer interests. An insurance regulator ensures that all basic policies have identical coverage rules so that no person is medically disadvantaged by his or her choice of insurer.
Hospitals in the Netherlands are also regulated and inspected but are mostly privately run and not for profit, as are many of the insurance companies. Patients can choose where they want to be treated, and have access to information on the internet about the performance and waiting times at each hospital. Patients dissatisfied with their insurer and choice of hospital can cancel at any time, but must make a new agreement with another insurer.
Insurance companies can offer additional services at extra cost over and above the universal system laid down by the regulator, e.g., for dental care. The standard monthly premium for health care paid by individual adults is about €100 per month. Persons with low incomes can get assistance from the government if they cannot afford these payments. Children under 18 are insured by the system at no additional cost to them or their families because the insurance company receives the cost of this from the regulator's fund. There is a fixed yearly deductible of €385 for each adult person, excluding first visits for diagnosis to general physicians.
Norway
Norway has a universal public health system paid largely from taxation in the same way as other Scandinavian countries. The Norwegian health care system is government-funded and heavily decentralized. The health care system in Norway is financed primarily through taxes levied by county councils and municipalities. Dental care is included for children until 18 years old, and is covered for adults for some ailments.[115]
Norway regularly comes top or close to the top of worldwide healthcare rankings.
North Macedonia
Health in North Macedonia
The country inherited a large health infrastructure after independence in 1991 with good well-distributed public health services. Private hospitals were opened and primary care was privatised. Subsequently both public and private providers have been integrated into one social insurance-funded model managed by the Health Insurance Fund of North Macedonia. The public hospital sector is seen as inefficient and is unpopular with both patients and professional staff. 90% of the population are within 30 minutes of a health service.
Expenditure on healthcare was $851 per head in 2014, 6.5% of GDP.
According to the Euro health consumer index the Macedonian health system made the most remarkable advance of any country in the history of their Index, from 27th to 16th place in 2014, because by implementing a real time e-Booking system they reduced waiting lists so significantly. From July 2013, any GP can make a booking at any specialist or heavy diagnostic equipment in the country in real time while the patient is present. They rated Macedonia 16th in Europe in 2015.
The Doctor’s Chamber of Macedonia complains that there is a discrepancy between the available funds and the quality of service expected, that facilities are not used efficiently, equipment is outdated and staff are not used effectively.
Portugal
Portugal's National Healthcare Service, known nationally as Serviço Nacional de Saúde (SNS), is a universal and free healthcare service provided nationwide since 1979 and available to both Portuguese and foreign residents. In 2014, Portugal SNS ranked 13th best healthcare service in Europe.[116] The National Medical Emergency Institute (INEM) is the main emergency medical service and can be activated by calling 112.
Romania
According to Article 34 of the Constitution of Romania, the state is obliged "to guarantee the protection of healthcare". Romania has a fully universal healthcare system, which covers medical check-ups, any surgical interventions, and any postoperative medical care, as well as free or subsidized medicine for a range of diseases. The state is also obliged to fund public hospitals and clinics. Dental care is not funded by the state, although there are public dental clinics in some hospitals, which treat patients free of charge.
Russia
In the former Soviet Union, the preferred term was "socialist medicine"; the Russian language has no term to distinguish between "socialist" and "socialized" (other than "public", Rus: obshchestvenniy/общественный, sometimes "collectivized" or "nationalized", Rus: obobshchestvlenniy/обобществленный).[117][118]
Russia in Soviet times (between 1917 and 1991) had a totally socialist model of health care with a centralized, integrated, hierarchically organised with the government providing free health care to all citizens. Quality of care and access to medications was not equal however and was dependent on the social status of patient. The best care was provided for nomenklatura and their family members, who had segregated from the rest of population facilities, such as Kremlin hospital.[119] Initially successful at combating infectious diseases, the effectiveness of the socialized model declined with underinvestment. Despite a doubling in the number of hospital beds and doctors per capita between 1950 and 1980, the quality of care began to decline by the early 1980s and medical care and health outcomes were below western standards.
The new mixed economy Russia has switched to a mixed model of health care with private financing and provision running alongside state financing and provision. The OECD reported that unfortunately, none of this has worked out as planned and the reforms have in many respects made the system worse.[120] The population's health has deteriorated on virtually every measure. The resulting system is overly complex and very inefficient. It has little in common with the model envisaged by the reformers. Although there are more than 300 private insurers and numerous public ones in the market, real competition for patients is rare leaving most patients with little or no effective choice of insurer, and in many places, no choice of health care provider either. The insurance companies have failed to develop as active, informed purchasers of health care services. Most are passive intermediaries, making money by simply channelling funds from regional OMS funds to healthcare providers.
Article 41 of the Constitution of the Russian Federation confirms a citizen's right to state healthcare and medical assistance free of charge.[121] This is achieved through state compulsory medical insurance (OMS), which is funded by an obligatory medical insurance payroll tax and government subsidies.[122][123] It worth mentioning that Russian citizens never pay taxes for themselves and often doesn't even know how much taxes do they pay, because tax payment process is maintained by companies they are working on.[124] Introduction in 1993 reform of new free market providers in addition to the state-run institutions intended to promote both efficiency and patient choice. A purchaser-provider split help facilitate the restructuring of care, as resources would migrate to where there was greatest demand, reduce the excess capacity in the hospital sector and stimulate the development of primary care. Russian Prime Minister Vladimir Putin announced a new large-scale health care reform in 2011 and pledged to allocate more than 300 billion rubles ($10 billion) in the next few years to improve health care in the country. As of 2020 the health insurance tax (called deposition to an OMS fund) is 5.1%.[125]
Serbia
The Constitution of the Republic of Serbia states that it is a right of every citizen to seek medical assistance free of charge.[126] This is achieved by mutual contribution to the Compulsory Social Healthcare Fund of RZZO (Republički Zavod za Zdravstveno Osiguranje or National Health Insurance Institution). The amount of contribution depends on the amount of money the person is making.
Spain
Spain provides a public universal health care system for all citizens and, under certain conditions, also non-citizens. Healthcare is free except for co-payments in some products and services; it is mostly paid from the Social Security budget. Adult dental care is not covered but for basic extractions or problems that could result in serious stomatological conditions.
Irrespective of the nationality and insurance situation of the patient, the public system always treats medical emergencies until achieving the best possible outcome. If not covered by the Spanish Social Security (i.e., a visiting foreigner), the provider later negotiates payment with the patient or the patient's insurer. If actually unable to pay, it is covered by the Social Security on humanitarian grounds unless the patient purposely traveled to Spain to get free healthcare. Obvious unexpected emergencies like accidental injuries or sudden illness are customarily covered, but those that could be reasonably expected (e.g., arising from a chronic condition or from avoidable risk-taking) are studied on a case-per-case basis.
According to the World Economic Forum and to Bloomberg, Spain has the most efficient health system in Europe, and also ranks at the top worldwide along with Hong Kong, Japan and Singapore.[127][128]
Private health insurance is available for those who prefer it, and recommended for visitors not covered by the Spanish Social Security or a foreign public or private insurer with overseas coverage.
Sweden
Sweden has a universal public health care system paid for through taxation. The Swedish public and private health care systems are funded through taxes levied by the county councils. Government-paid dental care is accessible for those under 23 years old.
Sweden also has a smaller private health care sector, mainly in larger cities or as centers for preventive health care financed by employers.
In recent years the health care system of Sweden has been heavily criticized for not providing the same quality of health care to all Swedish citizens.[129][130][131][132] This was especially brought to light during the COVID-19 pandemic as Swedish media and public health researchers pointed out that Swedish citizens of other ethnicities than Swedish and people living in working class areas were dying from COVID-19 at a significantly higher rate than the rest of the population.[133][134][135]
Switzerland
Purchasing basic health insurance is mandatory for all persons residing in Switzerland (within three months of taking up residence or being born in the country).[136] Healthcare in Switzerland is universally available and is regulated by the Federal Health Insurance Act of 1994. Supplemental insurance plans are optional. Insurers are required to offer insurance to everyone, regardless of age or medical condition. They are not allowed to make a profit off this basic insurance, but can on supplemental plans.[137]
Turkey
Turkey achieved universal health coverage in 2003.[138]
The Government's Health Transformation Program of 2003 established a common benefit package that covers primary and preventive care, ambulatory and inpatient care, laboratory services, rehabilitation and follow-up services, pharmaceuticals and medical aids and appliances.[138] Payroll taxes of 12.5% of a person's gross income (5% by the employee and 7.5% by the employer) fund 97%[139] of the program. The government provides for the remaining 3% of the cost.[140]
United Kingdom
Each of the countries of the United Kingdom has a National Health Service that provides public healthcare to all UK permanent residents that was originally designed to be free at the point of need and paid for from general taxation; but changes included introducing charging for prescription medicines and dentistry (those below 16 and those on certain benefits may still get free treatment). However, since health is now a devolved matter, considerable differences are developing between the systems in each of the countries as for example Northern Ireland, Scotland and Wales abolished prescription charges.[141] Private healthcare companies are free to operate alongside the public system.
England
Aug2005.jpg.webp)
The National Health Service (NHS), created by the National Health Service Act 1946, has provided the majority of healthcare in England since its launch on July 5, 1948.
The NHS Constitution for England documents, at high level, the objectives of the NHS, the legal rights and responsibilities of the various parties (patients, staff, NHS trust boards), and the guiding principles that govern the service.[142] The NHS constitution makes it clear that it provides a comprehensive service, available to all irrespective of age, gender, disability, race, sexual orientation, religion, or belief; that access to NHS services is based on clinical need and not an individual's ability to pay; and that care is never refused on unreasonable grounds. Patient choice in terms of doctor, care, treatments, and place of treatment is an important aspect of the NHS's ambition, and in some cases patients can elect for treatment in other European countries at the NHS's expense. Waiting times are low, with most people able to see their primary care doctor on the same day or the following day.[143] Only 36.1% of hospital admissions are from a waiting list, with the remainder being either emergencies admitted immediately or else pre-booked admissions or the like (e.g., child birth).[144] One of the main goals of care management is to ensure that patients do not experience a delay of more than 18 weeks from initial hospital referral to final treatment, inclusive of time for all associated investigative tests and consultations.[145] At present, two-thirds of patients are treated in under 12 weeks.[146]
Though centrally funded, the NHS is not managed by a large central bureaucracy. Responsibility is divided among geographical areas through strategic health authorities. Management is distributed even more locally through primary care trusts, hospital trusts—and increasingly to NHS foundation trusts that providing even more decentralized services within the NHS framework, with more decisions left to local people, patients, and staff. The central government office—the Department of Health—is not involved in day-to-day decision making in either the Strategic Health Authorities or the individual local trusts (primarily health, hospital, or ambulance) or the national specialist trusts such as NHS Blood and Transplant. It does lay down general guidelines they must follow. Local trusts are accountable to their local populations, whilst government ministers are accountable to Parliament for the service overall.
The NHS provides, among other things, primary care, in-patient care, long-term healthcare, psychiatric care and treatments, ophthalmology, and dentistry. All treatment is taxpayer-funded with the exception of certain charges for prescriptions, dentistry and ophthalmology (which themselves are free to children, certain students in full-time education, the elderly, the unemployed and those on low incomes). Around 89 percent of NHS prescriptions are obtained free of charge, mostly for children, pensioners, and pregnant women. Others pay a flat rate of £9.00, and others may cap their annual charges by purchasing an NHS Prescription Prepayment Certificate. Private health care has continued parallel to the NHS, paid for largely by private insurance. Private insurance accounts for only 4 percent of health expenditure and covers little more than a tenth of the population.[147] Private insurers in the UK only cover acute care from specialists. They do not cover generalist consultations, pre-existing conditions, medical emergencies, organ transplants, chronic conditions such as diabetes, or conditions such as pregnancy or HIV.[148]
Most NHS general practitioners are private doctors who contract to provide NHS services, but most hospitals are publicly owned and run through NHS trusts. A few NHS medical services (such as "surgicentres") are sub-contracted to private providers[149] as are some non-medical services (such as catering). Some capital projects such as new hospitals have been funded through the Private Finance Initiative, enabling investment without (in the short term) increasing the public sector borrowing requirement, because long-term contractually obligated PFI spending commitments are not counted as government liabilities.
Northern Ireland
Health and Social Care in Northern Ireland is the designation of the national public health service in Northern Ireland.
Scotland

NHS Scotland, created by the National Health Service (Scotland) Act 1947, was also launched on July 5, 1948, although it has always been a separate organization. Since devolution, NHS Scotland has followed the policies and priorities of the Scottish Government, including the phasing out of all prescription charges by 2011. Prescriptions are now free in Scotland for all citizens. All healthcare in Scotland remains free at the point of use.
Wales
NHS Wales was originally formed as part of the same NHS structure created by the National Health Service Act 1946 but powers over the NHS in Wales came under the Secretary of State for Wales in 1969,[150] in turn being transferred under devolution to what is now the Welsh Government.
Crown dependencies
Isle of Man
The Isle of Man, a UK Crown dependency, provides universal public health coverage to its residents.[151]
Guernsey/Jersey
The medical care system in the Channel Islands is very similar to that of the UK in that many of the doctors and nurses have been trained from the UK health perspective. There is universal health care for residents of the islands.[152]
North and Central America
The Bahamas, Barbados, Canada, Costa Rica, Cuba, Mexico, Panama, and Trinidad and Tobago all provide some level of universal health coverage.
The Bahamas
The Bahamas approved the National Health Insurance Act in August 2016. The legislation establishes a universal health coverage system that begins with universal coverage of primary health care services, and later expands to include a wide set of benefits that includes all specialized care. The system allows for universal coverage of a basic benefit package and for voluntary insurance to be purchased as a top-up policy to cover services or amenities that are not included in the government plan.[153]
Canada
In 1984, the Canada Health Act was passed, which prohibited extra billing by doctors on patients while at the same time billing the public insurance system. In 1999, the prime minister and most premiers reaffirmed in the Social Union Framework Agreement that they are committed to health care that has "comprehensiveness, universality, portability, public administration and accessibility."[154]
The system is for the most part publicly funded, yet most of the services are provided by private enterprises or private corporations, although most hospitals are public. Most doctors do not receive an annual salary, but receive a fee per visit or service.[155] About 29% of Canadians' health care is paid for by the private sector or individuals.[156] This mostly goes towards services not covered or only partially covered by Medicare such as prescription drugs, dentistry, physiotherapy and vision care.[157] Many Canadians have private health insurance, often through their employers, that cover these expenses.[158]
The Canada Health Act of 1984 "does not directly bar private delivery or private insurance for publicly insured services," but provides financial disincentives for doing so. "Although there are laws prohibiting or curtailing private health care in some provinces, they can be changed," according to a report in the New England Journal of Medicine.[159][160] The legality of the ban was considered in a decision of the Supreme Court of Canada, which ruled in Chaoulli v. Quebec that "the prohibition on obtaining private health insurance, while it might be constitutional in circumstances where health care services are reasonable as to both quality and timeliness, is not constitutional where the public system fails to deliver reasonable services." The appellant contended that waiting times in Quebec violated a right to life and security in the Quebec Charter of Human Rights and Freedoms. The Court agreed, but acknowledged the importance and validity of the Canada Health Act, and at least four of the seven judges explicitly recognized the right of governments to enact laws and policies that favour the public over the private system and preserve the integrity of the public system.
Costa Rica
Universal healthcare and pensions are run by the Caja Costarricense de Seguro Social (CCSS). In 1941, Costa Rica established Caja Costarricense de Seguro Social (CCSS), a social security insurance system for wage-earning workers. In 1961, coverage was expanded to include workers’ dependents and from 1961 to 1975, a series of expansions extended coverage for primary care and outpatient and inpatient specialized services to people in rural areas, the low-income population, and certain vulnerable populations. Further expansions during the late 1970s extended insurance coverage to farmers, peasants, and independent contract workers. Additionally, CCSS mandates free health service provision to mothers, children, indigenous people, the elderly, and people living with disabilities, regardless of insurance coverage. By 2000, 82 percent of the population was eligible for CCSS, which has continued to expand in the ensuing period. By covering all population groups through the same system, Costa Rica has avoided social insurance stratification and inequity common in many other countries in the region.[161]
CCSS is funded by a 15 percent payroll tax, as well as payments from retiree pensions [6]. Taxes on luxury goods, alcohol, soda, and imported products also help to cover poor households who do otherwise pay into the system. All CCSS funds are merged into a single pool, which is managed by the central financial administration of CCSS. In 1973, the Ministry of Health decided to move away from direct service provision and adopt a steering role. Responsibility for the provision of most care was transferred to the CCSS, although the Ministry retained responsibility for disease control, food and drug regulation, environmental sanitation, child nutrition, and primary care for the poor. Through the CCSS, health care is now essentially free to nearly all Costa Ricans. Private health care is also widely available and INS offers private health insurance plans to supplement CCSS insurance.[162]
Cuba
The Cuban government operates a national health system and assumes fiscal and administrative responsibility for the health care of all its citizens. There are no private hospitals or clinics as all health services are government-run. The present Minister for Public Health is Roberto Morales Ojeda. The government organized medical missions in other countries have taken a significant number of doctors and other personnel. In 2005 there were 25,000 Cuban doctors in Venezuela.
Mexico
Public health care became universal healthcare on January 1, 2020[163] mandated by the new President Andrés Manuel López Obrador and approved by Congress. It is completely free for Mexican citizens who do not have health insurance. Mexico's new universal healthcare, administered by the Instituto de Salud para el Bienestar (Institute of Health for Welfare, INSABI), includes free consultations with family doctors and specialists, free medications, free surgeries, free dental and vision . As of 2020, public health care is provided to all Mexican citizens as guaranteed via Article 4 of the Constitution. Public care is now fully subsidized by the federal government. All Mexican citizens are eligible for subsidized health care regardless of their work status via a system of health care facilities operating under the federal Secretariat of Health (formerly the Secretaria de Salubridad y Asistencia, or SSA) agency.
Employed citizens and their dependents, however, are further eligible to use the health care program administered and operated by the Instituto Mexicano del Seguro Social (IMSS) (English: Mexican Social Security Institute). The IMSS health care program is a tripartite system funded equally by the employee, its private employer, and the federal government. The IMSS does not provide service to employees of the public sector. Employees in the public sector are serviced by the Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE) (English: Institute for Social Security and Services for State Workers), which attends to the health and social care needs of government employees. This includes local, state, and federal government employees. The government of the states in Mexico also provide health services independently of those services provided by the federal government programs. In most states, the state government has established free or subsidized healthcare to all their citizens.
In 2006, the Mexican government created the Health Insurance for a New Generation also known as "life insurance for babies".[164][165][166] On May 28, 2009, Universal Care Coverage for Pregnant Women was introduced.[167] In an 2020 expansion of health care coverage, all Mexicans are now covered.
Trinidad and Tobago
A universal health care system is used in Trinidad and Tobago and is the primary form of health-care available in the country. It is used by the majority of the population seeking medical assistance, as it is free for all citizens. Responsibility for the provision of healthcare services in Trinidad and Tobago was devolved from the Ministry of Health to Regional Health Authorities under the Regional Health Authorities Act No. 5 in 1994.
South America
Argentina, Brazil, Chile, Colombia, Ecuador, Peru, Uruguay, and Venezuela all provide some level of universal health coverage.
Argentina
Health care is provided through a combination of employer and labor union-sponsored plans (Obras Sociales), government insurance plans, public hospitals and clinics and through private health insurance plans. It costs almost 10% of GDP and is available to anyone regardless of ideology, beliefs, race or nationality.
Brazil
The universal health care system was adopted in Brazil in 1988 after the end of the military regime's rule. However, universal health care was available many years before, in some cities, once the 27th amendment to the 1969 Constitution imposed the duty of applying 6% of their income in healthcare on the municipalities.[168] The Brazilian universal health care is called SUS (Sistema Único de Saúde), which covers all treatments, surgeries and medications for all resident and non-resident individuals within Brazilian jurisdiction, regardless of ethnicity, nationality, or visa - including tourists, passengers in transit and refugees.
Chile
Health care in Chile is provided by the government (via public corporation FONASA, National Healthcare Fund) and by private insurers (via ISAPRE, Previsional Healthcare Institutions). All workers and pensioners are mandated to pay 7% of their income for health care insurance (the poorest pensioners are exempt from this payment but medications are expensive and pensioners have to pay). Workers who choose not to join an Isapre, are automatically covered by Fonasa. Fonasa also covers unemployed people receiving unemployment benefits, uninsured pregnant women, insured worker's dependant family, people with mental or physical disabilities and people who are considered poor or indigent.
Fonasa costs vary depending on income, disability or age. Attention at public health facilities via Fonasa is free for low-income earners, people with mental or physical disabilities and people over the age of 60. Others pay 10% or 20% of the costs, depending on income and number of dependants. Fonasa beneficiaries may also seek attention in the private sector, for a designated fee.
Additionally, exist the GES Plan (Explicit Guarantees in Healthcare Plan), that consist of a defined number of high-morbility and mortality diseases (currently 85) that have special mandatory attention guarantees for all people, both Isapre and Fonasa affiliates, in relation to:
- Access: Universal access to treatment if required. Individuals will be able to get attention from a provider near their place of residence.
- Opportunity: Opportune waiting times, there is a maximum pre-established time limit to get initial and post-diagnosis attention.
- Financial protection: Law-fixed maximum price with low copayments to providers (maximum copayment of 20% of the cost), the payment cannot be an obstacle to attention. The total cost must not exceed one monthly income for the family in a year.
- Best possible quality of service: Attention only in accredited public or private Health centers, that follow technical requirement standards that will be established based on medical evidence.
The treatment protocols and number of diseases included are evaluated every 3 years by the authorities.
Colombia
In 1993 a reform transformed the health care system in Colombia, trying to provide a better, sustainable, health care system and to reach every Colombian citizen.
Peru
On April 10, 2009, the Government of Peru published the Law on Health Insurance to enable all Peruvians to access quality health services, and contribute to regulate the financing and supervision of these services. The law enables all population to access diverse health services to prevent illnesses, and promote and rehabilitate people, under a Health Basic Plan (PEAS).[169][170]
On April 2, 2010, President Alan Garcia Perez signed a supreme ordinance approving the regulations for the framework law on the Universal Health Insurance, which seeks to provide access to quality health care for all Peruvian citizens.
Peru's Universal Health Insurance law aims to increase access to timely and quality health care services, emphasizes maternal and child health promotion, and provides the poor with protection from financial ruin due to illness.[171]
The regulation states that membership of the Universal Health Insurance (AUS for its Spanish acronym) is compulsory for the entire population living in the country. To that end, the Ministry of Health will approve, by supreme ordinance, the mechanisms leading to compulsory membership, as well as escalation and implementation.[172]
Suriname
The National Basic Health Insurance Law, introduced in 2014, provides access to a basic package of primary, secondary, and tertiary care services for citizens. It repeals the Healthcare Tariffs Law from 2005.
Oceania
Australia and New Zealand both have universal health care. Hospitalisation is free for permanent residents, however general practice and prescriptions are subsidised only.
Australia
In Australia, Medibank—as it was then known—was introduced, by the Whitlam Labor government on July 1, 1975, through the Health Insurance Act 1973. The Australian Senate rejected the changes multiple times and they were passed only after a joint sitting after the 1974 double dissolution election. However, Medibank was supported by the subsequent Fraser Coalition (Australia) government and became a key feature of Australia's public policy landscape. The exact structure of Medibank/Medicare, in terms of the size of the rebate to doctors and hospitals and the way it has administered, has varied over the years. The original Medibank program proposed a 1.35% levy (with low income exemptions) but these bills were rejected by the Senate, and so Medibank was funded from general taxation. In 1976, the Fraser Government introduced a 2.5% levy and split Medibank in two: a universal scheme called Medibank Public and a government-owned private health insurance company, Medibank Private.
During the 1980s, Medibank Public was renamed Medicare by the Hawke Labor government, which also changed the funding model, to an income tax surcharge, known as the Medicare Levy, which was set at 1.5%, with exemptions for low income earners.[173] The Howard Coalition government introduced an additional levy of 1.0%, known as the Medicare Levy Surcharge, for those on high annual incomes ($70,000) who do not have adequate levels of private hospital coverage.[174] This was part of an effort by the Coalition to encourage take-up of private health insurance. According to WHO, government funding covered 67.5% of Australia's health care expenditures in 2004; private sources covered the remaining 32.5% of expenditures.[61]
As of 2019, the Medicare levy is 2% of taxable income,[175] with a Medicare levy surcharge, for those on high income who do not have appropriate private patient hospital cover (1% for singles on $90,000 pa and families on $180,000 pa, rising to 1.5% for higher incomes).[176]
New Zealand
As with Australia, New Zealand's healthcare system is funded through general taxation according to the Social Security Act 1938. However, aside from hospitalisation, there are user charges for prescriptions (introduced in February 1985) and partial subsidisation of general practitioner visits with additional provision for those on low or modest incomes known as Community Service Cards (introduced on February 1, 1992) to target healthcare based on income.[177][178][179] These changes were part of broader controversial policies introduced by the Fourth National Government between 1991 and 1993 and effectively ended largely free provision of primary healthcare. According to the WHO, government sources covered 77.4% of New Zealand's health care costs in 2004; private expenditures covered the remaining 22.6%.
Historic attempts to bring general practitioner care into government ownership have been largely unfulfilled.
There are twenty district health boards as of 2019 whose task is ensuring the provision of health and disability services to populations within a defined geographical area and are partially elected while the remainder is appointed by New Zealand's Minister of Health.[180] This system of management came into being on January 1, 2001, abolishing the much controversial Crown Health Enterprises regime which had replaced Area Health Boards previously
See also
- Health system
- Health systems by country
- List of countries by health insurance coverage
References
- ↑ Butticè, Claudio (2019). Universal Health Care. Santa Barbara, California: Greenwood Publishing Group. p. 20. ISBN 978-1-4408-6844-3. Archived from the original on January 13, 2021. Retrieved May 5, 2022.
- ↑ Abelson, Reed; Sanger-Katz, Margot (March 23, 2019). "Medicare for All Would Abolish Private Insurance. 'There's No Precedent in American History.'". The New York Times. Archived from the original on April 7, 2022. Retrieved May 5, 2022.
- ↑ "Brazil". Commonwealth Fund. June 5, 2020. Archived from the original on January 8, 2022. Retrieved January 8, 2022.
- ↑ "Algeria – Health And Welfare". Countrystudies.us. Archived from the original on October 12, 2011. Retrieved November 14, 2011.
- ↑ "Algeria Profile" (PDF). Archived (PDF) from the original on October 13, 2018. Retrieved May 5, 2022.
- ↑ "Botswana:The Health System - AHO". Archived from the original on August 3, 2014. Retrieved November 30, 2016.
- ↑ JLN. "Burkina Faso adopts universal health insurance system - - Joint Learning Network". Archived from the original on May 8, 2016. Retrieved November 30, 2016.
- ↑ "Insurance". Archived from the original on October 7, 2017. Retrieved November 30, 2016.
- ↑ "NHIS - Your Access to Healthcare". Archived from the original on May 16, 2014. Retrieved November 30, 2016.
- ↑ "Tiny African Island Has Soaring GDP, Free Healthcare and Free Higher Education - The Utopianist". Archived from the original on April 26, 2016. Retrieved November 30, 2016.
- ↑ Boutayeb, Abdesslam (March 7, 2006). "International Journal for Equity in Health | Full text | Social inequalities and health inequity in Morocco". International Journal for Equity in Health. Equityhealthj.com. 5 (1): 1. doi:10.1186/1475-9276-5-1. PMC 1420301. PMID 16522204.
- ↑ "In Rwanda, Health Care Coverage That Eludes the U.S." Opinionator (blog of The New York Times). July 3, 2012. Archived from the original on February 3, 2014.
- ↑ "Health care in South Africa". SouthAfrica.info. Archived from the original on January 3, 2014. Retrieved November 14, 2011.
- ↑ "Survey: Medical aid customer satisfaction slides". bizcommunity.com. Archived from the original on August 3, 2019. Retrieved August 3, 2019.
- ↑ "81% of households that use public healthcare 'satisfied' - Stats SA". SouthAfrica.info. June 22, 2018. Archived from the original on August 3, 2019. Retrieved August 3, 2019.
- ↑ "The healthcare system in Tunisia". Archived from the original on January 19, 2017. Retrieved November 30, 2016.
- ↑ "National Health Policy: Ministry of Health" (PDF). Archived (PDF) from the original on August 15, 2021. Retrieved May 5, 2022.
- ↑ "Introduction to healthcare in Bahrain". Justlanded.com. Archived from the original on November 15, 2011. Retrieved November 14, 2011.
- ↑ "BPJS Kesehatan". bpjs-kesehatan.go.id. Archived from the original on April 27, 2022. Retrieved May 5, 2022.
- ↑ "The best and worst of worlds: Tehran's public hospital wards". Theguardian.com. January 28, 2015. Archived from the original on January 29, 2015. Retrieved September 15, 2020.
- ↑ The Health Care System in Israel- An Historical Perspective Archived November 24, 2021, at the Wayback Machine Israel Ministry of Foreign Affairs. Retrieved June 7, 2006.
- ↑ "Embassy of Jordan (Washington, D.C.) – Jordan Information Bureau". Jordanembassyus.org. Archived from the original on December 4, 2011. Retrieved November 14, 2011.
- ↑ "Kazakhstan Health System – Flags, Maps, Economy, History, Climate, Natural Resources, Current Issues, International Agreements, Population, Social Statistics, Political System". Photius.com. Archived from the original on January 18, 2012. Retrieved November 14, 2011.
- ↑ "Malaysia Health System Review" (PDF). Archived from the original (PDF) on March 27, 2014.
- ↑ "Mongolia Health-Care Systems – Flags, Maps, Economy, History, Climate, Natural Resources, Current Issues, International Agreements, Population, Social Statistics, Political Sy". Photius.com. Archived from the original on November 3, 2011. Retrieved November 14, 2011.
- ↑ "Oman Guide: Introduction, An introduction to health care in Oman: Oman offers high quality health care equal". Justlanded.com. Archived from the original on November 15, 2011. Retrieved November 14, 2011.
- 1 2 Yusafzai, Mushtaq (November 6, 2020). "PM Imran Khan launches free healthcare services programme in KP today". The News International. Archived from the original on November 6, 2020. Retrieved November 7, 2020.
- ↑ "WHO | Primary Health Care in Action". Who.int. September 26, 2008. Archived from the original on October 16, 2008. Retrieved November 14, 2011.
- ↑ "North Korea's Surprisingly Robust Healthcare System". Globalasia.org. Archived from the original on October 26, 2021. Retrieved October 26, 2021.
- ↑ "Ministry of Health and Nutrition, Sri Lanka". Health.gov.lk. Archived from the original on November 18, 2011. Retrieved November 14, 2011.
- ↑ Obaida Hamad (February 2011). "Health system reforms: Better services at what cost?". Forward Magazine. Archived from the original on May 22, 2012. Retrieved April 11, 2012.
- ↑ "Bureau of National Health Insurance, Taiwan". Nhi.gov.tw. September 28, 2011. Archived from the original on September 28, 2011. Retrieved November 14, 2011.
- ↑ "Country Health System Profile: Bhutan". World Health Organization. Archived from the original on June 1, 2012.
- ↑ Guo, Jia (March 28, 2017). "How does healthcare in the U.S. compare with China's?". SupChina. Archived from the original on March 24, 2022. Retrieved September 15, 2020.
- 1 2 Zhou, Viola (January 10, 2018). "Does China have universal health care? A long (and better) answer". Inkstone. South China Morning Post Publishers Ltd. Archived from the original on November 29, 2021. Retrieved May 5, 2022.
- 1 2 Yip, Winnie; Hsiao, William (March 2008). "The Chinese Health System At A Crossroads". Health Affairs. 27 (2): 460–8. doi:10.1377/hlthaff.27.2.460. PMID 18332503.
- ↑ Carrin G, Ron A, Hui Y, et al. (April 1999). "The reform of the rural cooperative medical system in the People's Republic of China: interim experience in 14 pilot counties". Soc Sci Med. 48 (7): 961–72. doi:10.1016/S0277-9536(98)00396-7. PMID 10192562.
- ↑ Staff (October 14, 2008). "Medical Reform Draft Open to Public Debate" Archived February 25, 2021, at the Wayback Machine. Xinhua News Agency (via the China Internet Information Center). Retrieved April 10, 2014.
- ↑ Staff (January 21, 2009). "China Passes New Medical Reform Plan" Archived March 12, 2016, at the Wayback Machine. xinhuanet.com. Retrieved April 10, 2014.
- ↑ "Healthy life expectancy in Hong Kong" Archived July 16, 2021, at the Wayback Machine. World Health Organization. Retrieved June 7, 2008.
- ↑ "Rank Order – Life expectancy at birth". The World Factbook, Central Intelligence Agency. January 24, 2008. Archived from the original on December 26, 2018. Retrieved February 1, 2008.
- ↑ "World Population Prospects: The 2006 Revision" (PDF). United Nations. 2007. Archived (PDF) from the original on October 31, 2017. Retrieved February 1, 2008.
- ↑ Olsen, Sonja K.; Brown, Robert S. (2008). "Live Donor Liver Transplantation: Current Status". Current Gastroenterology Reports. 10 (1): 36–42. doi:10.1007/s11894-008-0007-x. PMID 18417041. S2CID 19274021.
- ↑ Zodpey, Sanjay; Farooqui, Habib Hasan (2018). "Universal Health Coverage in India: Progress achieved & the way forward". The Indian Journal of Medical Research. 147 (4): 327–329. doi:10.4103/ijmr.IJMR_616_18. PMC 6057252. PMID 29998865.
- ↑ "Covid is an opportunity to make structural changes to our largest health insurance and pension schemes". April 21, 2021. Archived from the original on April 23, 2021. Retrieved May 5, 2022.
- ↑ "Archive copy". Archived from the original on December 12, 2020. Retrieved May 5, 2022.
{{cite web}}: CS1 maint: archived copy as title (link) - ↑ "Why you should not miss out on your health insurance renewal". April 20, 2021. Archived from the original on April 23, 2021. Retrieved May 5, 2022.
- ↑ "17 Government Health Insurance Schemes in India: Govt Mediclaim Policy". Archived from the original on June 9, 2021. Retrieved May 5, 2022.
- ↑ ₹2.6 trillion
- ↑ "Primary health care". www.who.int. Archived from the original on April 1, 2022. Retrieved May 5, 2022.
- ↑ "Health Care in the Mohallas (SSIR)". ssir.org. Archived from the original on April 22, 2022. Retrieved May 5, 2022.
- ↑ Kalra, Aditya (October 30, 2014). "India's universal healthcare rollout to cost $26 billion". Reuters. Archived from the original on January 22, 2017. Retrieved November 30, 2016.
- ↑ "Q&A: BPJS Kesehatan, health for all Indonesians". The Jakarta Post. Archived from the original on January 16, 2021. Retrieved May 5, 2022.
- ↑ "Health Minister Vows to Fast-Track Private Hospital Permits". Jakarta Globe. Archived from the original on November 5, 2019. Retrieved May 5, 2022.
- ↑ "Indonesia - HEALTH". countrystudies.us. Archived from the original on November 3, 2016. Retrieved May 5, 2022.
- ↑ "history of Israel health care". Archived from the original on October 23, 2021. Retrieved May 5, 2022.
- ↑ Cohen, Nisim. "?מיהו יזם פוליטי" [Who is a Political Promoter?] (PDF) (in עברית). Open University of Israel. Archived (PDF) from the original on December 26, 2019. Retrieved December 26, 2019.
- ↑ "World Health Day 2018 – Lessons from Malaysia on Universal Health Coverage". World Health Organization. April 18, 2018. Archived from the original on March 11, 2022. Retrieved March 22, 2022.
- ↑ Desk, BR Web (December 13, 2021). "PM Imran launches Naya Pakistan Sehat Programme in Punjab". Brecorder. Archived from the original on December 13, 2021. Retrieved December 13, 2021.
- ↑ "EXPLAINER: Universal Health Care Law and what it means to PH development". National Economic and Development Authority. June 18, 2019. Archived from the original on July 26, 2021. Retrieved July 26, 2021.
- 1 2 3 4 "World Health Organization Statistical Information System: Core Health Indicators". Who.int. Archived from the original on April 29, 2007. Retrieved November 14, 2011.
- ↑ World Health Organization, "World Health Statistics 2007: Mortality", based on 2005 data.
- 1 2 John Tucci, "The Singapore health system – achieving positive health outcomes with low expenditure", Watson Wyatt Healthcare Market Review, October 2004. Archived April 19, 2010, at the Wayback Machine
- ↑ Library of Congress – Federal Research Division (2007). "Country Profile: North Korea" (PDF). Library of Congress – Federal Research Division. Archived (PDF) from the original on February 26, 2005. Retrieved September 6, 2010.
- ↑ Country Profile 2007, pp. 7–8.
- ↑ "Ask a North Korean: What is the healthcare system in the DPRK really like? | NK News". February 21, 2020. Archived from the original on May 12, 2022. Retrieved May 5, 2022.
- ↑ "Archived copy". Archived from the original on November 24, 2016. Retrieved January 28, 2017.
{{cite web}}: CS1 maint: archived copy as title (link) - ↑ Fanchiang, Cecilia (January 2, 2004). "New IC health insurance card expected to offer many benefits" Archived June 6, 2008, at the Wayback Machine. Taiwan Journal. Retrieved March 28, 2008.
- ↑ "Taiwan Takes Fastrack to Universal Health Care". All Things Considered, NPR. April 15, 2008. Archived from the original on August 13, 2008. Retrieved October 5, 2008.
- ↑ Jui-Fen Rachel Lu; William C. Hsiao (2003). "Does Universal Health Insurance Make Health Care Unaffordable? Lessons From Taiwan". Health Affairs. 22 (3): 77–88. doi:10.1377/hlthaff.22.3.77. PMID 12757274.
- ↑ G20 Health Care: "Health Care Systems and Health Market Reform in the G20 Countries." Prepared for the World Economic Forum by Ernst & Young. January 3, 2006.
- ↑ "The Universal Coverage Policy of Thailand: An Introduction". Unescap.org. Archived from the original on January 19, 2012. Retrieved November 14, 2011.
- ↑ Hughes D, Leethongdee S (2007). "Universal coverage in the land of smiles: lessons from Thailand's 30 baht health reforms". Health Affairs. 26 (4): 999–1008. doi:10.1377/hlthaff.26.4.999. PMID 17630443.
- ↑ "Thailand eliminates mother-to-child HIV transmission". CNN. June 8, 2016. Archived from the original on February 6, 2018. Retrieved February 5, 2018.
- ↑ Sanger-Katz, Margot (February 19, 2019). "What's the Difference Between a 'Public Option' and 'Medicare for All'?". The New York Times. Archived from the original on April 9, 2022. Retrieved May 5, 2022.
- ↑ Belarus. "Health in Belarus. Healthcare system of Belarus". Europe-cities.com. Archived from the original on September 30, 2011. Retrieved November 14, 2011.
- ↑ "Moldova Healthcare". Archived from the original on January 25, 2010.
- ↑ Portugal: Bentes M, Dias CM, Sakellarides C, Bankauskaite V. Health Care Systems in Transition: Portugal. Archived January 26, 2010, at the Wayback Machine WHO are Regional Offices for Europe on behalf of the European Observatory on Health Systems and Policies, 2004.
- ↑ Constitution of Ukraine Archived April 15, 1997, at the Wayback Machine Chapter 2, Article 49. Adopted at the Fifth Session of the Verkhovna Rada of Ukraine on June 28, 1996.
- ↑ Physicians for a National Health Program "International Health Systems". Archived August 21, 2019, at the Wayback Machine
- ↑ Staff (undated). "The Austrian healthcare system Overview of how it works" Archived April 13, 2020, at the Wayback Machine. justlanded.com. Retrieved October 16, 2011.
- ↑ Corens, Dirk (2007). "Belgium, health system review" (PDF). Health Systems in Transition. European Observatory on Health Systems and Policies. 9 (2). Archived (PDF) from the original on August 30, 2021. Retrieved May 5, 2022.
- ↑ Euro WHO (2018). "HiT-Bulgaria" (PDF). Archived (PDF) from the original on March 20, 2022. Retrieved May 5, 2022.
- ↑ "KELA – Use of European Health Insurance Card in Finland". Kela.fi. Archived from the original on November 25, 2011. Retrieved November 14, 2011.
- ↑ "European Commission: Health and long-term care in the European Union" (PDF). Archived (PDF) from the original on December 27, 2011. Retrieved November 14, 2011.
- ↑ "Health Systems in Transition Vol. 10 No. 4 2008; Finland health system review" (PDF). Archived (PDF) from the original on September 24, 2015. Retrieved January 9, 2015.
- ↑ "Reimbursements for medicine expenses". kela.en. Archived from the original on May 12, 2021. Retrieved May 5, 2022.
- 1 2 3 4 Järvelin, Jutta (2002). "Health Care Systems in Transition" (PDF). The European Observatory on Health Care Systems. Archived (PDF) from the original on February 25, 2009. Retrieved February 25, 2009.
- ↑ http://www.oecd.org/dataoecd/52/33/38976604.pdf Archived September 24, 2015, at the Wayback Machine
- ↑ http://ec.europa.eu/public_opinion/archives/ebs/ebs_283_en.pdf Archived June 26, 2016, at the Wayback Machine European Commission: Health and long-term care in the European Union
- ↑ "News item on healthcare costs in 2006 (in Finnish)" Archived May 27, 2022, at the Wayback Machine.
- ↑ "World Health Organization Assesses the World's Health Systems". Who.int. December 8, 2010. Archived from the original on November 11, 2020. Retrieved January 6, 2012.
- ↑ "Georgia's health financing reforms show tangible benefits for the population". Archived from the original on November 24, 2021. Retrieved May 5, 2022.
- ↑ Verulava T, Jorbenadze R, Barkalaia T (2017). "Introduction of universal health program in Georgia: Problems and Perspectives". Georgian Medical News. 262 (262): 116–120. PMID 28252441. Archived from the original on February 26, 2021. Retrieved May 5, 2022.
- ↑ Bump, Jesse B. (October 19, 2010). "The long road to universal health coverage. A century of lessons for development strategy" (PDF). Seattle: PATH. Archived from the original (PDF) on April 6, 2020. Retrieved March 11, 2013.
Carrin and James have identified 1988—105 years after Bismarck's first sickness fund laws—as the date Germany achieved universal health coverage through this series of extensions to minimum benefit packages and expansions of the enrolled population. Bärnighausen and Sauerborn have quantified this long-term progressive increase in the proportion of the German population covered by public and private insurance. Their graph is reproduced below as Figure 1: German Population Enrolled in Health Insurance (%) 1885–1995.
- ↑ Carrin, Guy; James, Chris (January 2005). "Social health insurance: Key factors affecting the transition towards universal coverage" (PDF). International Social Security Review. 58 (1): 45–64. doi:10.1111/j.1468-246x.2005.00209.x. S2CID 154659524. Archived (PDF) from the original on January 12, 2020. Retrieved March 11, 2013.
Initially the health insurance law of 1883 covered blue-collar workers in selected industries, craftspeople and other selected professionals.6 It is estimated that this law brought health insurance coverage up from 5 to 10 per cent of the total population.
- ↑ Bärnighausen, Till; Sauerborn, Rainer (May 2002). "One hundred and eighteen years of the German health insurance system: are there any lessons for middle- and low income countries?" (PDF). Social Science & Medicine. 54 (10): 1559–1587. doi:10.1016/S0277-9536(01)00137-X. PMID 12061488. Archived from the original on May 15, 2020. Retrieved March 11, 2013.
As Germany has the world's oldest SHI [social health insurance] system, it naturally lends itself to historical analyses.
- ↑ Leichter, Howard M. (1979). A comparative approach to policy analysis: health care policy in four nations. Cambridge: Cambridge University Press. p. 121. ISBN 978-0-521-22648-6.
The Sickness Insurance Law (1883). Eligibility. The Sickness Insurance Law came into effect in December 1884. It provided for compulsory participation by all industrial wage earners (i.e., manual laborers) in factories, ironworks, mines, shipbuilding yards, and similar workplaces.
- ↑ Hennock, Ernest Peter (2007). The origin of the welfare state in England and Germany, 1850–1914: social policies compared. Cambridge: Cambridge University Press. p. 157. ISBN 978-0-521-59212-3.
- 1 2 3 "Private or public? An introduction health insurance in Germany". allaboutberlin.com. Archived from the original on April 6, 2020. Retrieved February 8, 2019.
- ↑ GKV-Spitzenverband. "Statutory health insurance - GKV-Spitzenverband". www.gkv-spitzenverband.de (in Deutsch). Archived from the original on February 9, 2019. Retrieved February 8, 2019.
- ↑ Kirkman-Liff BL (1990). "Physician Payment and Cost-Containment Strategies in West Germany: Suggestions for Medicare Reform". Journal of Health Care Politics, Policy and Law. 15 (1): 69–99. doi:10.1215/03616878-15-1-69. PMID 2108202.
- ↑ Henke KD (May 2007). "[External and internal financing in health care]". Med. Klin. (Munich) (in Deutsch). 102 (5): 366–72. doi:10.1007/s00063-007-1045-0. PMID 17497087. S2CID 46136822.
- ↑ "Length of hospital stay, Germany". Group-economics.allianz.com. July 25, 2005. Archived from the original on June 12, 2011. Retrieved November 14, 2011.
- ↑ "Length of hospital stay, U.S". Cdc.gov. Archived from the original on April 6, 2020. Retrieved November 14, 2011.
- ↑ Borger C, Smith S, Truffer C, et al. (2006). "Health spending projections through 2015: changes on the horizon". Health Aff (Millwood). 25 (2): w61–73. doi:10.1377/hlthaff.25.w61. PMID 16495287.
- ↑ Esmail, N (2005). How Good is Canadian Health Care? 2005 Report. fraserinstitute.org. p. 2.
- ↑ "Health Act 2004". Irish Statute Book. Office of the Attorney General. Archived from the original on June 5, 2011. Retrieved October 5, 2010.
- ↑ "Prescription charges for medical card holders". www.citizensinformation.ie. Archived from the original on April 23, 2022. Retrieved May 5, 2022.
- ↑ "Hospital Charges". HSE.ie. Archived from the original on February 25, 2022. Retrieved May 5, 2022.
- ↑ Cullen, Paul. "Cost of GP visit varies from €30 to €65 across State". The Irish Times. Archived from the original on March 7, 2021. Retrieved May 5, 2022.
- ↑ "Sláintecare". www.gov.ie. Archived from the original on May 5, 2022. Retrieved December 2, 2020.
- ↑ "Life Sciences and Health Care". Deloitte Luxembourg. Archived from the original on June 24, 2021. Retrieved May 5, 2022.
- ↑ "CNS // Luxembourg". cns.public.lu. Archived from the original on May 1, 2022. Retrieved May 5, 2022.
- ↑ "Who Pays Your Dental Bill?". Helsenorge. December 6, 2019. Archived from the original on July 1, 2016. Retrieved May 5, 2022.
- ↑ "Archived copy" (PDF). Archived from the original (PDF) on February 24, 2016. Retrieved November 21, 2015.
{{cite web}}: CS1 maint: archived copy as title (link) - ↑ Zhuraleva et al., Teaching History of Medicine in Russia Archived March 1, 2021, at the Wayback Machine.
- ↑ "Yandex Lingvo". Archived from the original on May 27, 2022. Retrieved May 27, 2022.
- ↑ Natalya Rapoport Untold Stories of Pioneers in Medical Sciences Under Stalin's Tyranny Archived May 27, 2022, at the Wayback Machine 304 pages, 2020 ISBN 978-9811209178 ISBN 9811209170
- ↑ "Search Official Documents - OECD" (PDF). Archived (PDF) from the original on August 16, 2018. Retrieved August 15, 2018.
- ↑ "Chapter 2. Rights and Freedoms of Man And Citizen | The Constitution of the Russian Federation". www.constitution.ru. Archived from the original on June 16, 2021. Retrieved May 5, 2022.
- ↑ "О МЕДИЦИНСКОМ СТРАХОВАНИИ ГРАЖДАН В РОССИЙСКОЙ ФЕДЕРАЦИИ". Archived from the original on February 3, 2016. Retrieved April 11, 2012.
- ↑ "Russia – Unified Social Tax replaced by insurance contributions". Archived from the original on June 28, 2010.
- ↑ "В России граждане платят одни из самых высоких налогов. Мы подсчитали (и ужаснулись)". Телеканал «Красная Линия». Archived from the original on August 15, 2021. Retrieved May 5, 2022.
- ↑ "Страховые взносы на ОМС". www.ffoms.gov.ru. Archived from the original on January 21, 2022. Retrieved May 5, 2022.
- ↑ "Ustav Republike Srbije (The Constitution of the Republic of Serbia)". Archived from the original on April 29, 2011. Retrieved April 11, 2012.
- ↑ "Spanish healthcare, once again leading world rankings". #ThisIsTheRealSpain. February 21, 2020. Archived from the original on May 8, 2020. Retrieved April 19, 2020.
- ↑ "Bloomberg - Healthcare efficiency scores in 56 countries". www.bloomberg.com. Archived from the original on April 24, 2022. Retrieved April 19, 2020.
- ↑ "Svenskarna lever länge men hälsan är ojämlik i landet". Folkhälsomyndigheten. January 22, 2020. Archived from the original on October 12, 2020. Retrieved October 12, 2020.
- ↑ "Sjukvårdens struktur bidrar till ojämlik vård". Läkartidningen. June 15, 2018. Archived from the original on August 13, 2020. Retrieved October 12, 2020.
- ↑ "Arbete för jämlik hälsa i Sverige nationellt, regionalt och lokalt". Idunn. January 1, 2016. Archived from the original on October 18, 2020. Retrieved October 12, 2020.
- ↑ "Ojämlik vård – dags för verkstad". Life-time. March 26, 2015. Archived from the original on October 17, 2020. Retrieved October 12, 2020.
- ↑ "Risk of dying from COVID-19 in Sweden is greater for men and the unmarried". Stockholm University. October 9, 2020. Archived from the original on October 11, 2020. Retrieved October 12, 2020.
- ↑ "Covid-19 vanligare i utsatta områden - är sårbarhet för sjukdomar en klassfråga?". Stockholm University. April 24, 2020. Archived from the original on October 12, 2020. Retrieved October 12, 2020.
- ↑ "Corona härjar bland fattiga – rika klarar sig". Expressen. April 24, 2020. Archived from the original on June 28, 2020. Retrieved June 28, 2020.
- ↑ "Health insurance for foreign nationals". www.ch.ch. Archived from the original on February 22, 2021. Retrieved May 5, 2022.
- ↑ Schwartz, Nelson D. (October 1, 2009). "Swiss health care thrives without public option". The New York Times. p. A1. Archived from the original on June 30, 2017. Retrieved May 5, 2022.
- 1 2 Tatar, M., S. Mollahaliloglu, B. Sahin, S. Aydin, A. Maresso and C. Hernández-Quevedo (2011), “Turkey: Health System Review”, Health Systems in Transition, Vol. 13, No. 6, pp. 1-186.
- ↑ Borowitz, M. and H. Kluge (forthcoming), “Pay for Performance in Health Care: Implications for Health System Efficiency and Accountability”, WHO and the European Observatory on Health Systems and Policies Publishers.
- ↑ Sulku, S. and D. Bernard (2009), “Financial Burden of Health Care Expenditures in Turkey: 2002-2003”, Agency for Healthcare Research and Quality Working Paper, No. 09004, Rockville, United States.
- ↑ NHS now four different systems Archived April 3, 2009, at the Wayback Machine BBC January 2, 2008
- ↑ "NHS Constitution for England". Dh.gov.uk. Archived from the original on January 7, 2013. Retrieved November 14, 2011.
- ↑ Cathy Schoen; Robin Osborn (2004). "The Commonwealth Fund 2004 International Health Policy Survey of Primary Care in Five Countries" (PDF). Archived (PDF) from the original on March 3, 2016. Retrieved May 5, 2022.
- ↑ Kingdom, NHS Digital, 1 Trevelyan Square, Boar Lane, Leeds, LS1 6AE, United. "Hospital Episode Statistics". Retrieved November 30, 2016.
{{cite web}}: CS1 maint: url-status (link) - ↑ "18 weeks patient pathway". Archived from the original on October 12, 2009. Retrieved November 30, 2016.
- ↑ "18 weeks patient pathway" (PDF). Archived from the original (PDF) on March 25, 2009. Retrieved November 30, 2016.
- ↑ Smee, Clive (October 2000). "Department of Health Special Section: Reconsidering the Role of Competition in Health Care Markets". Journal of Health Politics, Policy and Law. 25 (5): 945–951. doi:10.1215/03616878-25-5-945. PMID 11068739. Archived from the original on March 4, 2016. Retrieved May 27, 2022.
- ↑ Are you buying private medical insurance? Archived February 15, 2010, at the Wayback Machine Association of British Insurers
- ↑ "N. generation surgery-centers to carry out thousands more NHS operations every year". Department of Health. December 3, 2002. Archived from the original on March 5, 2007. Retrieved September 15, 2006.
- ↑ Introduction to NHS Wales 1960's Archived July 7, 2009, at the Wayback Machine www.wales.nhs.uk
- ↑ "Department of Health Service Delivery Plan 2011" (PDF). Archived from the original (PDF) on December 29, 2011. Retrieved August 7, 2011.
- ↑ "Expat Guernsey". Archived from the original on October 1, 2011. Retrieved August 7, 2011.
- ↑ "NHI Bahamas -". Archived from the original on November 14, 2016. Retrieved November 30, 2016.
- ↑ Government of Canada, Social Union, News Release, "A Framework to Improve the Social Union for Canadians: An Agreement between the Government of Canada and the Governments of the Provinces and Territories, February 4, 1999 Archived November 12, 2011, at the Wayback Machine." Retrieved December 20, 2006.
- ↑ Public vs. private health care. Archived August 23, 2006, at the Wayback Machine CBC, December 1, 2006.
- ↑ Press release, "Health care spending to reach $160 billion this year" Archived December 23, 2007, at the Wayback Machine, Canadian Institute for Health Information, November 13, 2007. Retrieved November 19, 2007.
- ↑ National Health Expenditure Trends, 1975–2007 Archived February 14, 2008, at the Wayback Machine, Canadian Institute for Health Information, November 13, 2007. Retrieved November 19, 2007.
- ↑ The OECD Health Project (2004). Private Health Insurance In OECD Countries. Organisation for Economic Co-operation and Development. ISBN 978-92-64-00668-3.
- ↑ Kraus, Clifford (February 26, 2006). "As Canada's Slow-Motion Public Health System Falters, Private Medical Care Is Surging". The New York Times. Archived from the original on January 8, 2016. Retrieved July 16, 2007.
- ↑ Steinbrook, R. (April 2006). "Private health care in Canada". New England Journal of Medicine. 354 (16): 1661–4. doi:10.1056/NEJMp068064. PMID 16625005.
- ↑ Health System Innovations in Central America. World Bank Working Papers. The World Bank. July 1, 2005. doi:10.1596/978-0-8213-6278-5. ISBN 978-0-8213-6278-5.
- ↑ Toward Universal Health Coverage and Equity in Latin America and the Caribbean https://dx.doi.org/10.1596/978-1-4648-0454-0 Archived May 27, 2022, at the Wayback Machine
- ↑ Fisher, Bill (January 1, 2020). "Universal Healthcare INSABI begins in Mexico January 1st announced Health Department". Gobierno de Mexico. Archived from the original on February 17, 2020. Retrieved February 17, 2020.
- ↑ "El portal único del gobierno. | gob.mx". failover.www.gob.mx. Archived from the original on December 8, 2009.
- ↑ "El portal único del gobierno. | gob.mx". failover.www.gob.mx. Archived from the original on January 10, 2011.
- ↑ "El portal único del gobierno. | gob.mx". failover.www.gob.mx. Archived from the original on June 22, 2009.
- ↑ "El portal único del gobierno. | gob.mx". failover.www.gob.mx. Archived from the original on June 22, 2009.
- ↑ "Emc1". Planalto.gov.br. Archived from the original on April 23, 2020. Retrieved November 14, 2011.
- ↑ "Law on Health Insurance published today". Andina.com.pe. Archived from the original on October 1, 2011. Retrieved November 14, 2011.
- ↑ "President Garcia: Law on Health Insurance marks major reform". Andina.com.pe. Archived from the original on October 1, 2011. Retrieved November 14, 2011.
- ↑ "Aseguramiento Universal de Salud – Perú". Aus-peru.blogspot.com. February 24, 2004. Archived from the original on August 12, 2011. Retrieved November 14, 2011.
- ↑ "President Garcia signs regulations for Universal Health Insurance law". Andina.com.pe. Archived from the original on October 1, 2011. Retrieved November 14, 2011.
- ↑ Australian Taxation Office (June 19, 2007). "What is the Medicare levy?". Archived from the original on October 22, 2007. Retrieved February 15, 2008.
- ↑ "Medicare Levy Surcharge". Ato.gov.au. Archived from the original on August 12, 2013. Retrieved November 14, 2011.
- ↑ "Medicare levy". Australian Taxation Office. Australian Government. Archived from the original on June 29, 2013. Retrieved June 27, 2019.
- ↑ "Medicare levy surcharge". Australian Taxation Office. Australian Government. Archived from the original on June 27, 2019. Retrieved June 27, 2019.
- ↑ Community Service Cards Archived November 2, 2011, at the Wayback Machine Authored by Steve Maharey, former Minister of Social Development
- ↑ https://books.google.co.nz/books?id=OW7YHJ0gZ4gC&pg=PA6971&lpg=PA6971&dq=prescription+charges+michael+bassett&source=bl&ots=W-cad02rJW&sig=ACfU3U3xS7-2vbHcZXVoCxsIwBRsZ6y4tg&hl=en&sa=X&ved=2ahUKEwjh6_jMjezmAhUtwzgGHZWZAQMQ6AEwAHoECAoQAQ#v=onepage&q=prescription%20charges%20michael%20bassett&f=false Archived March 8, 2021, at the Wayback Machine New Zealand Parliamentary Debates, September 19, 1985, pg 6,971
- ↑ Healthcare Archived January 25, 2022, at the Wayback Machine Authored by Michael Bassett, former Minister of Health between 1984 and 1987
- ↑ https://www.beehive.govt.nz/feature/community-services-card-fact-sheet Archived August 15, 2021, at the Wayback Machine from Ministry of Health, last updated January 2005