Ulcerative colitis
| Ulcerative colitis | |
|---|---|
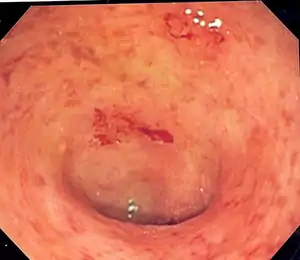 | |
| Endoscopic image of a colon affected by ulcerative colitis. The internal surface of the colon is blotchy and broken in places. Mild-moderate disease. | |
| Specialty | Gastroenterology |
| Symptoms | Abdominal pain, diarrhea mixed with blood, weight loss, fever, anemia[1] |
| Complications | Megacolon, inflammation of the eye, joints, or liver, colon cancer[1][2] |
| Usual onset | 15–30 years or > 60 years[1] |
| Duration | Long term[1] |
| Causes | Unknown[1] |
| Diagnostic method | Colonoscopy with tissue biopsies[1] |
| Differential diagnosis | Dysentery, Crohn's disease, ischemic colitis[3] |
| Treatment | Dietary changes, medication, surgery[1] |
| Medication | Sulfasalazine, mesalazine, steroids, immunosuppressants such as azathioprine, biological therapy[1] |
| Frequency | Up to 5 per 1000 people[4] |
| Deaths | 47,400 together with Crohn's (2015)[5] |
Ulcerative colitis (UC) is a long-term condition that results in inflammation and ulcers of the colon and rectum.[1][6] The primary symptoms of active disease are abdominal pain and diarrhea mixed with blood.[1] Weight loss, fever, and anemia may also occur.[1] Often, symptoms come on slowly and can range from mild to severe.[1] Symptoms typically occur intermittently with periods of no symptoms between flares.[1] Complications may include megacolon, inflammation of the eye, joints, or liver, and colon cancer.[1][2]
The cause of UC is unknown.[1] Theories involve immune system dysfunction, genetics, changes in the normal gut bacteria, and environmental factors.[1][7] Rates tend to be higher in the developed world with some proposing this to be the result of less exposure to intestinal infections, or to a Western diet and lifestyle.[6][8] The removal of the appendix at an early age may be protective.[8] Diagnosis is typically by colonoscopy with tissue biopsies.[1] It is a kind of inflammatory bowel disease (IBD) along with Crohn's disease and microscopic colitis.[1]
Dietary changes, such as maintaining a high-calorie diet or lactose-free diet, may improve symptoms.[1] Several medications are used to treat symptoms and bring about and maintain remission, including aminosalicylates such as mesalazine or sulfasalazine, steroids, immunosuppressants such as azathioprine, and biologic therapy.[1] Removal of the colon by surgery may be necessary if the disease is severe, does not respond to treatment, or if complications such as colon cancer develop.[1] Removal of the colon and rectum generally cures the condition.[1][8]
Together with Crohn's disease, about 11.2 million people were affected as of 2015.[9] Each year it newly occurs in 1 to 20 per 100,000 people, and 5 to 500 per 100,000 individuals are affected.[6][8] The disease is more common in North America and Europe than other regions.[8] Often it begins in people aged 15 to 30 years, or among those over 60.[1] Males and females appear to be affected in equal proportions.[6] It has also become more common since the 1950s.[6][8] Together, ulcerative colitis and Crohn's disease affect about a million people in the United States.[10] With appropriate treatment the risk of death appears the same as that of the general population.[2] The first description of ulcerative colitis occurred around the 1850s.[8]
Signs and symptoms
| Crohn's disease | Ulcerative colitis | |
|---|---|---|
| Defecation | Often porridge-like,[11] sometimes steatorrhea | Often mucus-like and with blood[11] |
| Tenesmus | Less common[11] | More common[11] |
| Fever | Common[11] | Indicates severe disease[11] |
| Fistulae | Common[12] | Seldom |
| Weight loss | Often | More seldom |
Gastrointestinal
People with ulcerative colitis usually present with diarrhea mixed with blood and mucus, of gradual onset that persists for an extended period of time (weeks). People with UC may experience rectal tenesmus, which is the urgent desire to evacuate the bowels but with the passage of little stool. Tenesmus may be misinterpreted as constipation, due to the urge to defecate despite small volume of stool passage. Lower abdominal pain often occurs in UC, and the severity varies from mild discomfort to very painful bowel movements and abdominal cramping.[13] High frequency of bowel movements, weight loss, nausea, fatigue, and fever are also common during disease flares. The inflammation caused by the disease along with the chronic bleeding from the GI tract often leads to anemia, which may contribute to fatigue.
The clinical presentation of ulcerative colitis depends on the extent of the disease process.[14] A substantial proportion (up to 45%) of people with a history of UC without any ongoing symptoms (clinical remission) have objective evidence of ongoing inflammation.[15] Ulcerative colitis is associated with a generalized inflammatory process that can affect many parts of the body. Sometimes, these associated extra-intestinal symptoms are the initial signs of the disease, such as painful arthritis of the knees.
Extent of involvement
In contrast to Crohn's disease, which can affect areas of the gastrointestinal tract outside of the colon, ulcerative colitis is usually confined to the colon. Inflammation in ulcerative colitis is usually continuous, typically involving the rectum, with involvement extending proximally (to sigmoid colon, ascending colon, etc). In contrast, inflammation with Crohn's disease is often patchy, with so-called "skip lesions."
The disease is classified by the extent of involvement, depending on how far the disease extends:[13] proctitis (rectal inflammation), proctosigmoiditis (rectal and sigmoid colon inflammation), left sided colitis (inflammation extending to descending colon), and extensive colitis (inflammation proximal to the descending colon). Pancolitis describes involvement of the entire colon, extending from the rectum to the cecum. While usually associated with Crohn's disease, ileitis (inflammation of the ileum) also occurs in UC. About 17% of individuals with UC have ileitis.[16] Ileitis more commonly occurs in the setting of pancolitis, and tends to correlate with the activity of colitis. This so-called "backwash ileitis" can occur in 10–20% of people with pancolitis and is believed to be of little clinical significance.[17]
Severity of disease
In addition to the extent of involvement, UC is also characterized by severity of disease.[18] Mild disease correlates with fewer than four stools daily; in addition, rectal bleeding and mild abdominal pain or cramping may be present. Mild disease lacks systemic signs of toxicity, and exhibits normal levels of serum inflammatory markers (erythrocyte sedimentation rate and C-reactive protein).
Moderate disease correlates with more than four stools daily, but with minimal signs of toxicity. Moderate abdominal pain, low-grade fever, 38 to 39 °C (100 to 102 °F), and anemia may develop (not requiring transfusion). Severe disease correlates with more than six bloody stools a day or observable massive and significant bloody bowel movements. Toxicity is present, as demonstrated by fever, tachycardia, anemia or an elevated ESR or CRP.
Fulminant disease correlates with more than 10 bowel movements daily, continuous bleeding, toxicity, abdominal tenderness and distension, blood transfusion requirement, and colonic dilation (expansion). People with fulminant UC may have inflammation extending beyond just the mucosal layer, causing impaired colonic motility and leading to toxic megacolon. If the serous membrane is involved, a colonic perforation may ensue. Without treatment, fulminant disease may be life threatening.
Extraintestinal features
| Crohn's disease | Ulcerative colitis | ||
|---|---|---|---|
| Nutrient deficiency | Higher risk | ||
| Colon cancer risk | Slight | Considerable | |
| Percent of people with extraintestinal complications[19][20][21] | |||
| Iritis/uveitis | Females | 2.2% | 3.2% |
| Males | 1.3% | 0.9% | |
| Primary sclerosing cholangitis | Females | 0.3% | 1% |
| Males | 0.4% | 3% | |
| Ankylosing spondylitis | Females | 0.7% | 0.8% |
| Males | 2.7% | 1.5% | |
| Pyoderma gangrenosum | Females | 1.2% | 0.8% |
| Males | 1.3% | 0.7% | |
| Erythema nodosum | Females | 1.9% | 2% |
| Males | 0.6% | 0.7% | |


As UC is believed to have a systemic (i.e., autoimmune) origin, people with UC may present with comorbidities leading to symptoms and complications outside the colon. The frequency of such extraintestinal manifestations has been reported as between 6 and 47%,[22] and include:
Aphthous ulcers may develop in the mouth. Inflammation may occur in the interior portion of the eye, leading to uveitis and iritis. Uveitis can cause blurred vision and eye pain, especially when exposed to light (photophobia). Untreated, uveitis can lead to permanent vision loss. Inflammation may also involve the white part of the eye (sclera) or the overlying connective tissue (episclera), causing conditions called scleritis and episcleritis, respectively.
UC may cause several joint manifestations, including a type of rheumatologic disease known as Seronegative arthritis, which may affect few large-joints (oligoarthritis), the vertebra (ankylosing spondylitis) or several small joints of the hands and feet (peripheral arthritis). Often the insertion site where muscle attaches to bone (entheses) becomes inflamed (enthesitis). Inlammation may affect the sacroiliac joint (sacroiliitis). The symptoms of arthritis include painful, warm, swollen, stiff joints, and loss of joint mobility or function.
Ulcerative colitis may affect the skin, blood, and endocrine system. The most common type of skin manifestation, erythema nodosum, presents as raised, tender red nodules usually appearing on the shins. Erythema nodosum is due to inflammation of the underlying subcutaneous tissue (panniculitis). A more severe skin manifestation, pyoderma gangrenosum, is characterized painful pustules or nodules that become ulcers which progressively grow. UC increases the risk of blood clots; painful swelling of the lower legs can be a sign of deep venous thrombosis, while difficulty breathing may be a result of pulmonary embolism (blood clots in the lungs). The immune system may attack the red blood cells, leading to autoimmune hemolytic anemia. In addition to autoimmune destruction, anemia may occur due to chronic blood loss from rectal bleeding and bone marrow suppression due to inflammation (anemia of chronic disease). Osteoporosis may occur related to systemic inflammation, which increases the risk of bone fractures. Clubbing, a deformity of the ends of the fingers, and hypertrophic osteoarthropathy may occur.
Primary sclerosing cholangitis
Ulcerative colitis has a significant association with primary sclerosing cholangitis (PSC), a progressive inflammatory disorder of small and large bile ducts. As many as 5% of people with ulcerative colitis may progress to develop primary sclerosing cholangitis.[23]
Causes
| Crohn's disease | Ulcerative colitis | |
|---|---|---|
| Smoking | Higher risk for smokers | Lower risk for smokers[24] |
| Age | Usual onset between 15 and 30 years[25] | Peak incidence between 15 and 25 years |
Ulcerative colitis is an autoimmune disease characterized by T-cells infiltrating the colon.[26] No direct causes for UC are known, but many possible factors such as genetics and environment play a role. US is associated with comorbidities that produce symptoms in many areas of the body outside the digestive system.
Genetic factors
A genetic component to the cause of UC can be hypothesized based on aggregation of UC in families, variation of prevalence between different ethnicities, genetic markers and linkages.[27] In addition, the identical twin concordance rate is 10%, whereas the dizygotic twin concordance rate is only 3%.[27][28]
Twelve regions of the genome may be linked to UC, including, in the order of their discovery, chromosomes 16, 12, 6, 14, 5, 19, 1, and 3,[29] but none of these loci has been consistently shown to be at fault, suggesting that the disorder is influenced by multiple genes. For example, chromosome band 1p36 is one such region thought to be linked to inflammatory bowel disease.[30] Some of the putative regions encode transporter proteins such as OCTN1 and OCTN2. Other potential regions involve cell scaffolding proteins such as the MAGUK family. Human leukocyte antigen associations may even be at work. In fact, this linkage on chromosome 6 may be the most convincing and consistent of the genetic candidates.[29]
Multiple autoimmune disorders have been recorded with the neurovisceral and cutaneous genetic porphyrias including UC, Crohn's disease,[31] celiac disease, dermatitis herpetiformis, diabetes, systemic and discoid lupus, rheumatoid arthritis, ankylosing spondylitis, scleroderma, Sjögren syndrome and scleritis.
Environmental factors
Many hypotheses have been raised for environmental factors contributing to the pathogenesis of ulcerative colitis, including diet, breastfeeding and medications. However, data regarding the possible protective effect of breastfeeding in the development of IBD are inconsistent. One Italian study showed a potential protective effect.[32] One study of isotretinoin found a small increase in the rate of UC.[33]
As the colon is exposed to many dietary substances which may encourage inflammation, dietary factors have been hypothesized to play a role in the pathogenesis of both ulcerative colitis and Crohn's disease. However, current research does not show a link between diet and the development of ulcerative colitis. Few studies have investigated such an association; one study showed no association of refined sugar on the number of people affected of ulcerative colitis.[34] High intake of unsaturated fat and vitamin B6 may enhance the risk of developing ulcerative colitis.[35] Other identified dietary factors that may influence the development and/or relapse of the disease include meat protein and alcoholic beverages.[36][37] Specifically, sulfur has been investigated as being involved in the cause of ulcerative colitis, but this is controversial.[38] Sulfur restricted diets have been investigated in people with UC and animal models of the disease. The theory of sulfur as an etiological factor is related to the gut microbiota and mucosal sulfide detoxification in addition to the diet.[39][40][41]
Alternative theories
Levels of sulfate-reducing bacteria tend to be higher in persons with ulcerative colitis, which could indicate higher levels of hydrogen sulfide in the intestine. An alternative theory suggests that the symptoms of the disease may be caused by toxic effects of the hydrogen sulfide on the cells lining the intestine.[42]
Infection by mycobacterium avium, subspecies paratuberculosis, has been proposed as the ultimate cause of both ulcerative colitis and Crohn's disease.[43]
Pathophysiology
| Crohn's disease | Ulcerative colitis | |
|---|---|---|
| Cytokine response | Associated with Th17[44] | Vaguely associated with Th2 |
An increased amount of colonic sulfate-reducing bacteria has been observed in some people with ulcerative colitis, resulting in higher concentrations of the toxic gas hydrogen sulfide. Human colonic mucosa is maintained by the colonic epithelial barrier and immune cells in the lamina propria (see intestinal mucosal barrier). N-butyrate, a short-chain fatty acid, gets oxidized through the beta oxidation pathway into carbon dioxide and ketone bodies. It has been shown that N-butyrate helps supply nutrients to this epithelial barrier. Studies have proposed that hydrogen sulfide plays a role in impairing this beta-oxidation pathway by interrupting the short chain acetyl-CoA dehydrogenase, an enzyme within the pathway. Furthermore, it has been suggested that the protective benefit of smoking in ulcerative colitis is due to the hydrogen cyanide from cigarette smoke reacting with hydrogen sulfide to produce the non-toxic isothiocyanate, thereby inhibiting sulfides from interrupting the pathway.[45] An unrelated study suggested that the sulfur contained in red meats and alcohol may lead to an increased risk of relapse for people in remission.[42]
Diagnosis

_active.jpg.webp)
The initial diagnostic workup for ulcerative colitis includes the following:[18][46]
- A complete blood count is done to check for anemia; thrombocytosis, a high platelet count, is occasionally seen
- Electrolyte studies and kidney function tests are done, as chronic diarrhea may be associated with hypokalemia, hypomagnesemia and pre-kidney failure.
- Liver function tests are performed to screen for bile duct involvement: primary sclerosing cholangitis.
- X-ray
- Urinalysis
- Stool culture, to rule out parasites and infectious causes.
- Erythrocyte sedimentation rate can be measured, with an elevated sedimentation rate indicating that an inflammatory process is present.
- C-reactive protein can be measured, with an elevated level being another indication of inflammation.
- Sigmoidoscopy a type of endoscopy which can detect the presence of ulcers in the rectum and lower section of the large intestine.
- Colonoscopy a type of endoscopy which can the full length of the large intestine and end of the small intestine (ileum).
Although ulcerative colitis is a disease of unknown causation, inquiry should be made as to unusual factors believed to trigger the disease.[18]
The simple clinical colitis activity index was created in 1998 and is used to assess the severity of symptoms.[47][48]
Endoscopic

The best test for diagnosis of ulcerative colitis remains endoscopy. Full colonoscopy to the cecum and entry into the terminal ileum is attempted only if the diagnosis of UC is unclear. Otherwise, a flexible sigmoidoscopy is sufficient to support the diagnosis. The physician may elect to limit the extent of the exam if severe colitis is encountered to minimize the risk of perforation of the colon. Endoscopic findings in ulcerative colitis include: erythema (redness of the mucosa), friability of the mucosa, superficial ulceration, and loss of the vascular appearance of the colon. When present, ulcerations may be confluent. Pseudopolyps may be observed.
Ulcerative colitis is usually continuous from the rectum, with the rectum almost universally being involved. Perianal disease is rare. The degree of involvement endoscopically ranges from proctitis (rectal inflammation) to left sided colitis (extending to descending colon), to extensive colitis (extending proximal to descending colon).[13]
Histologic
_endoscopic_biopsy.jpg.webp)
Biopsies of the mucosa are taken to definitively diagnose UC and differentiate it from Crohn's disease, which is managed differently clinically. Microbiological samples are typically taken at the time of endoscopy. The pathology in ulcerative colitis typically involves distortion of crypt architecture, inflammation of crypts (cryptitis), frank crypt abscesses, and hemorrhage or inflammatory cells in the lamina propria. In cases where the clinical picture is unclear, the histomorphologic analysis often plays a pivotal role in determining the diagnosis and thus the management.
Laboratory tests
Blood and stool tests serve primarily to assess disease severity, level of inflammation and rule out causes of infectious colitis. A complete blood count may demonstrate anemia, which may be caused by inflammation or bleeding. Chronic blood loss may lead to iron deficiency as a cause for anemia, particularly microcytic anemia (small red blood cells), which can be evaluated with a serum ferritin, iron, total iron-binding capacity and transferrin saturation. Anemia may be due to a complication of treatment from azathioprine, which can cause low blood counts, or sulfasalazine, which can result in folate deficiency. Thiopurine metabolites (from azathioprine) and a folate level can help.
UC may cause high levels of inflammation throughout the body, which may be quantified with serum inflammatory markers, such as CRP and ESR. However, elevated inflammatory markers are not specific for UC and elevations are commonly seen in other conditions, including infection. In addition, inflammatory markers are not uniformly elevated in people with ulcerative colitis. Twenty five percent of individuals with confirmed inflammation on endoscopic evaluation have a normal CRP level.[24] Serum albumin may also be low related to inflammation, in addition to loss of protein in the GI tract associated with bleeding and colitis. Low serum levels of vitamin D are associated with UC, although the significance of this finding is unclear.[49]
Specific antibody markers may be elevated in ulcerative colitis. Specifically, perinuclear antineutrophil cytoplasmic antibodies (pANCA) are found in 70 percent of cases of UC.[24] Antibodies against Saccharomyces cerevisiae may be present, but are more often positive in Crohn's disease compared with ulcerative colitis. However, due to poor accuracy of these serolologic tests, they are not helpful in the diagnostic evaluation of possible inflammatory bowel disease.[24]
Several stool tests may help quantify the extent of inflammation present in the colon and rectum. Fecal calprotectin is elevated in inflammatory conditions affecting the colon, and is useful in distinguishing irritable bowel syndrome (noninflammatory) from a flare in inflammatory bowel disease.[24] Fecal calprotectin is 88% sensitive and 79% specific for the diagnosis of ulcerative colitis.[24] Fecal leukocytes and lactoferrin are additional nonspecific markers of intestinal inflammation.
Differential diagnosis
The following conditions may present in a similar manner as ulcerative colitis, and should be excluded:
- Crohn's disease
- Infectious colitis, which is typically detected on stool cultures
- Entamoeba histolytica is a protozoan parasite that causes intestinal inflammation. A few cases have been misdiagnosed as UC with poor outcomes occurring due to the use of corticosteroids.[50]
- Pseudomembranous colitis, or Clostridium difficile-associated colitis, bacterial upsets often seen following administration of antibiotics
- Ischemic colitis, inadequate blood supply to the intestine, which typically affects the elderly
- Radiation colitis in people with previous pelvic radiotherapy
- Chemical colitis resulting from the introduction of harsh chemicals into the colon from an enema or other procedure.
- Malignancy[51]
The most common disease that mimics the symptoms of ulcerative colitis is Crohn's disease, as both are inflammatory bowel diseases that can affect the colon with similar symptoms. It is important to differentiate these diseases since their courses and treatments may differ. In some cases, however, it may not be possible to tell the difference, in which case the disease is classified as indeterminate colitis.[52]
| Crohn's disease | Ulcerative colitis | |
|---|---|---|
| Terminal ileum involvement | Commonly | Seldom |
| Colon involvement | Usually | Always |
| Rectum involvement | Seldom | Usually (95%)[53] |
| Involvement around the anus | Common[12] | Seldom |
| Bile duct involvement | No increase in rate of primary sclerosing cholangitis | Higher rate[54] |
| Distribution of disease | Patchy areas of inflammation (skip lesions) | Continuous area of inflammation[53] |
| Endoscopy | Deep geographic and serpiginous (snake-like) ulcers | Continuous ulcer |
| Depth of inflammation | May be transmural, deep into tissues[12][29] | Shallow, mucosal |
| Stenosis | Common | Seldom |
| Granulomas on biopsy | May have non-necrotizing non-peri-intestinal crypt granulomas[12][55][56] | Non-peri-intestinal crypt granulomas not seen[57] |
Management
Standard treatment for ulcerative colitis depends on the extent of involvement and disease severity. The goal is to induce remission initially with medications, followed by the administration of maintenance medications to prevent a relapse. The concept of induction of remission and maintenance of remission is very important. The medications used to induce and maintain a remission somewhat overlap, but the treatments are different. Physicians first direct treatment to inducing remission, which involves relief of symptoms and mucosal healing of the colon's lining, and then longer-term treatment to maintain remission and prevent complications. Acute severe ulcerative colitis requires hospitalisation, exclusion of infections, and corticosteroids.[58]
For acute stages of the disease, a low fiber diet may be recommended.[59][60]
Medication
Ulcerative colitis can be treated with a number of medications, including 5-ASA drugs such as sulfasalazine and mesalazine. Corticosteroids such as prednisone can also be used due to their immunosuppressive and short-term healing properties, but because their risks outweigh their benefits, they are not used long-term in treatment. Immunosuppressive medications such as azathioprine and biological agents such as infliximab and adalimumab are given only if people cannot achieve remission with 5-ASA and corticosteroids. Infliximab or vedolizumab are recommended in those with moderate or severe disease.[61] Such treatments are used less commonly due to their possible risk factors, including but not limited to increased risk of cancers in teenagers and adults,[62] tuberculosis, and new or worsening heart failure (these side effects are rare).[63]
A formulation of budesonide was approved by the U.S. Food and Drug Administration (FDA) for treatment of active ulcerative colitis in January 2013.[64] In 2018, tofacitinib was approved for treatment of moderately to severely active ulcerative colitis in the United States, the first oral medication indicated for long term use in this condition.[65] The evidence on methotrexate does not show a benefit in producing remission in people with ulcerative colitis.[66] Off-label use of drugs such as cyclosporin and tacrolimus has shown some benefits.[67][68][69][70]
Aminosalicylates
Sulfasalazine has been a major agent in the therapy of mild to moderate ulcerative colitis for over 50 years. In 1977, it was shown that 5-aminosalicylic acid (5-ASA, mesalazine/mesalamine) was the therapeutically active component in sulfasalazine.[71] Many 5-ASA drugs have been developed with the aim of delivering the active compound to the large intestine to maintain therapeutic efficacy but with reduction of the side effects associated with the sulfapyridine moiety in sulfasalazine. Oral 5-ASA drugs are particularly effective in inducing and in maintaining remission in mild to moderate ulcerative colitis.[72][73] Rectal suppository, foam or liquid enema formulations of 5-ASA are used for colitis affecting the rectum, sigmoid or descending colon, and have been shown to be effective especially when combined with oral treatment.[74]
Biologics
Biologic treatments such as the TNF inhibitors infliximab, adalimumab, and golimumab are commonly used to treat people with UC who are no longer responding to corticosteroids. Tofacitinib and vedolizumab can also produce good clinical remission and response rates in UC.[7] Biologics may be used early in treatment (step down approach), or after other treatments have failed to induce remission (step up approach); the strategy should be individualized.[75]
Unlike aminosalicylates, biologics can cause serious side effects such as an increased risk of developing extra-intestinal cancers,[62] heart failure; and weakening of the immune system, resulting in a decreased ability of the immune system to clear infections and reactivation of latent infections such as tuberculosis. For this reason, people on these treatments are closely monitored and are often tested for hepatitis and tuberculosis annually.[76][77]
Nicotine
Unlike Crohn's disease, ulcerative colitis has a lesser chance of affecting smokers than non-smokers.[78][79] In select individuals with a history of previous tobacco use, resuming low dose smoking may improve signs and symptoms of active ulcerative colitis.[80] Studies using a transdermal nicotine patch have shown clinical and histological improvement.[81] In one double-blind, placebo-controlled study conducted in the United Kingdom, 48.6% of people with UC who used the nicotine patch, in conjunction with their standard treatment, showed complete resolution of symptoms. Another randomized, double-blind, placebo-controlled, single-center clinical trial conducted in the United States showed that 39% of people who used the patch showed significant improvement, versus 9% of those given a placebo.[82] However, nicotine therapy is generally not recommended due to side effects and inconsistent results.[83][84][85]
Iron supplementation
The gradual loss of blood from the gastrointestinal tract, as well as chronic inflammation, often leads to anemia, and professional guidelines suggest routinely monitoring for anemia with blood tests repeated every three months in active disease and annually in quiescent disease.[86] Adequate disease control usually improves anemia of chronic disease, but iron deficiency anemia should be treated with iron supplements. The form in which treatment is administered depends both on the severity of the anemia and on the guidelines that are followed. Some advise that parenteral iron be used first because people respond to it more quickly, it is associated with fewer gastrointestinal side effects, and it is not associated with compliance issues.[87] Others require oral iron to be used first, as people eventually respond and many will tolerate the side effects.[86][88]
Surgery
| Crohn's disease | Ulcerative colitis | |
|---|---|---|
| Mesalazine | Less useful[89] | More useful[89] |
| Antibiotics | Effective in long-term[90] | Generally not useful[91] |
| Surgery | Often returns following removal of affected part | Usually cured by removal of colon |
Unlike in Crohn's disease, the gastrointestinal aspects of ulcerative colitis can generally be cured by surgical removal of the large intestine, though extraintestinal symptoms may persist. This procedure is necessary in the event of: exsanguinating hemorrhage, frank perforation, or documented or strongly suspected carcinoma. Surgery is also indicated for people with severe colitis or toxic megacolon. People with symptoms that are disabling and do not respond to drugs may wish to consider whether surgery would improve the quality of life.[13]
Ulcerative colitis affects many parts of the body outside the intestinal tract. In rare cases, the extra-intestinal manifestations of the disease may require removal of the colon – although this does not necessarily resolve these symptoms.[18]
The removal of the entire large intestine, known as a proctocolectomy, results in a permanent ileostomy – where a stoma is created by pulling the terminal ileum through the abdomen. Intestinal contents are emptied into a removable ostomy bag which is secured around the stoma using adhesive.
Another surgical option for ulcerative colitis that is affecting most of the large bowel is called the ileal pouch-anal anastomosis (IPAA). This is a two- or three-step procedure. In a three-step procedure, the first surgery is a sub-total colectomy, in which the large bowel is removed, but the rectum remains in situ, and a temporary ileostomy is made. The second step is a proctecomy and formation of the ileal pouch (commonly known as a "j-pouch"). This involves removing the large majority of the remaining rectal stump and creating a new "rectum" by fashioning the end of the small intestine into a pouch and attaching it to the anus. After this procedure, a new type of ileostomy is created (known as a loop ileostomy) to allow the anastomoses to heal. The final surgery is a take-down procedure where the ileostomy is reversed and there is no longer the need for an ostomy bag. When done in two steps, a proctocolectomy – removing both the colon and rectum – is performed alongside the pouch formation and loop ileostomy. The final step is the same take-down surgery as in the three-step procedure. Time taken between each step can vary, but typically a six- to twelve-month interval is recommended between the first two steps, and a minimum of two to three months is required between the formation of the pouch and the ileostomy take-down.[13]
While the ileal pouch procedure removes the need for an ostomy bag, it does not restore normal bowel function. In the months following the final operation, patients typically experience 8–15 bowel movements a day. Over time this number decreases, with many patients reporting four-six bowel movements after one year post-op. While many patients have success with this procedure, there are a number of known complications. Pouchitis, inflammation of the ileal pouch resulting in symptoms similar to ulcerative colitis, is relatively common. Pouchitis can be acute, remitting, or chronic however treatment using antibiotics, steroids, or biologics can be highly effective. Other complications include fistulas, abbesses, and pouch failure. Depending on the severity of the condition, pouch revision surgery may need to be performed. In some cased the pouch may need to be de-functioned or removed and an ileostomy recreated.[92][93]
Bacterial recolonization
- In a number of randomized clinical trials, probiotics have demonstrated the potential to be helpful in the treatment of ulcerative colitis. Specific types of probiotics such as Escherichia coli Nissle have been shown to induce remission in some people for up to a year.[94] The probiotics may work by calming some of the ongoing inflammation that causes the disease, which in turn allows the body to mobilize dendritic cells, otherwise known as messenger immune cells. These cells then are able to produce other T-cells that further aid in restoring balance in the intestines by rebalancing systematic inflammation.[95]
- Fecal microbiota transplant involves the infusion of human probiotics through fecal enemas. Ulcerative colitis typically requires a more prolonged bacteriotherapy treatment than Clostridium difficile infection to be successful, possibly due to the time needed to heal the ulcerated epithelium. The response of ulcerative colitis is potentially very favorable with one study reporting 67.7% of sufferers experiencing complete remission.[96] Other studies found a benefit from using fecal microbiota transplantation.[97][98][99] It suggests that the cause of ulcerative colitis may be a previous infection by a still unknown pathogen. This initial infection resolves itself naturally, but somehow causes an imbalance in the colonic bacterial flora, leading to a cycle of inflammation which can be broken by "recolonizing" the colon with bacteria from a healthy bowel. There have been several reported cases of person who have remained in remission for up to 13 years.[100]
Alternative medicine
A variety of alternative medicine therapies have been used for ulcerative colitis, with inconsistent results. Curcumin (turmeric), in conjunction with taking the medications mesalamine or sulfasalazine, may be effective and safe for maintaining remission in people with well controlled ulcerative colitis.[101] The effect of curcumin alone on quiescent ulcerative colitis is unknown.[101]
Prognosis
Progression or remission
People with ulcerative colitis usually have an intermittent course, with periods of disease inactivity alternating with "flares" of disease. People with proctitis or left-sided colitis usually have a more benign course: only 15% progress proximally with their disease, and up to 20% can have sustained remission in the absence of any therapy. A subset of people experience a course of disease progress rapidly. In these cases, there is usually a failure to respond to medication and surgery often is performed within the first few years of disease onset.[102][103] People with more extensive disease are less likely to sustain remission, but the rate of remission is independent of the severity of the disease.[104] Several risk factors are associated with eventual need for colectomy, including: prior hospitalization for UC, extensive colitis, need for systemic steroids, young age at diagnosis, low serum albumin, elevated inflammatory markers (CRP & ESR), and severe inflammation seen during colonoscopy.[24] Surgical removal of the large intestine often cures the disease.[18]
Colorectal cancer
The risk of colorectal cancer is significantly increased in people with ulcerative colitis after ten years if involvement is beyond the splenic flexure. People with backwash ileitis might have an increased risk for colorectal carcinoma.[105] Those people with only proctitis or rectosigmoiditis usually have no increased risk.[18] It is recommended that people have screening colonoscopies with random biopsies to look for dysplasia after eight years of disease activity, at one to two year intervals.[106]
Mortality
People with ulcerative colitis are at similar[107] or perhaps slightly increased overall risk of death compared with the background population.[108] However, the distribution of causes-of-death differs from the general population.[107] Specific risk factors may predict worse outcomes and a higher risk of mortality in people with ulcerative colitis, including: C. difficile infection[24] and cytomegalovirus infection (due to reactivation).[109]
Other long-term features
Changes that can be seen in chronic ulcerative colitis include granularity, loss of the vascular pattern of the mucosa, loss of haustra, effacement of the ileocecal valve, mucosal bridging, strictures and pseudopolyps.[110]
Epidemiology
Together with Crohn's disease, about 11.2 million people were affected as of 2015.[9] Each year, ulcerative colitis newly occurs in 1 to 20 per 100,000 people (incidence), and there are a total of 5-500 per 100,000 individuals with the disease (prevalence).[6][8] In 2015, a worldwide total of 47,400 people died due to inflammatory bowel disease (UC and Crohn's disease).[5] The peak onset is between 30 and 40 years of age,[111] with a second peak of onset occurring in the 6th decade of life.[112] Ulcerative colitis is equally common among men and women.[111][6] With appropriate treatment the risk of death appears the similar as that of the general population.[2] UC has become more common since the 1950s.[6][8]
The geographic distribution of UC and Crohn's disease is similar worldwide,[113] with the highest number of new cases a year of UC found in Canada, New Zealand and the United Kingdom.[114] The disease is more common in North America and Europe than other regions.[8] In general, higher rates are seen in northern locations compared to southern locations in Europe[115] and the United States.[116] UC is more common in western Europe compared with eastern Europe.[117] Worldwide, the prevalence of UC varies from 2 - 299 per 100,000 people.[4] Together, ulcerative colitis and Crohn's disease affect about a million people in the United States.[10]
As with Crohn's disease, the rates of UC are greater among Ashkenazi Jews and decreases progressively in other persons of Jewish descent, non-Jewish Caucasians, Africans, Hispanics, and Asians.[17] Appendectomy prior to age 20 for appendicitis[118] and current tobacco use[119] are protective against development of UC. However, former tobacco use is associated with a higher risk of developing the disease.[119]
United States
As of 2004, the number of new cases of UC in the United States was between 2.2 and 14.3 per 100,000 per year.[120] The number of people affected in the United States is between 37 and 246 per 100,000.[120]
Canada
In Canada, between 1998 and 2000, the number of new cases per year was 12.9 per 100,000 population or 4,500 new cases. The number of people affected was estimated to be 211 per 100,000 or 104,000.[121]
United Kingdom
In the United Kingdom 10 per 100,000 people newly develop the condition a year while the number of people affected is 243 per 100,000. Approximately 146,000 people in the United Kingdom have been diagnosed with UC.[122]
History
The first description of ulcerative colitis occurred around the 1850s.[8]
Research
Helminthic therapy using the whipworm Trichuris suis has been shown in a randomized control trial from Iowa to show benefit in people with ulcerative colitis.[123] The therapy tests the hygiene hypothesis which argues that the absence of helminths in the colons of people in the developed world may lead to inflammation. Both helminthic therapy and fecal microbiota transplant induce a characteristic Th2 white cell response in the diseased areas, which was unexpected given that ulcerative colitis was thought to involve Th2 overproduction.[124]
Alicaforsen is a first generation antisense oligodeoxynucleotide designed to bind specifically to the human ICAM-1 messenger RNA through Watson-Crick base pair interactions in order to subdue expression of ICAM-1.[125] ICAM-1 propagates an inflammatory response promoting the extravasation and activation of leukocytes (white blood cells) into inflamed tissue.[125] Increased expression of ICAM-1 has been observed within the inflamed intestinal mucosa of ulcerative colitis sufferers, where ICAM-1 over production correlated with disease activity.[126] This suggests that ICAM-1 is a potential therapeutic target in the treatment of ulcerative colitis.[127]
Gram positive bacteria present in the lumen could be associated with extending the time of relapse for ulcerative colitis.[128]
A series of drugs in development looks to disrupt the inflammation process by selectively targeting an ion channel in the inflammation signaling cascade known as KCa3.1.[129] In a preclinical study in rats and mice, inhibition of KCa3.1 disrupted the production of Th1 cytokines IL-2 and TNF-∝ and decreased colon inflammation as effectively as sulfasalazine.[129]
Neutrophil extracellular traps[130] and the resulting degradation of the extracellular matrix[131] have been reported in the colon mucosa in ulcerative colitis patients in clinical remission, indicating the involvement of the innate immune system in the etiology.[130]
Fexofenadine, an antihistamine drug used in treatment of allergies, has shown promise in a combination therapy in some studies.[132][133] Opportunely, low gastrointestinal absorption (or high absorbed drug gastrointestinal secretion) of fexofenadine results in higher concentration at the site of inflammation. Thus, the drug may locally decrease histamine secretion by involved gastrointestinal mast cells and alleviate the inflammation.[133]
There is evidence that etrolizumab is effective for ulcerative colitis, with phase 3 trials underway as of 2016.[7][134][135][136] Etrolizumab is a humanized monoclonal antibody that targets he β7 subunit of integrins α4β7 and αEβ7. Etrolizumab decreases lymphocytes trafficking, similar to vedolizumab (another integrin antagonist).
Leukocyte apheresis
A type of leukocyte apheresis, known as granulocyte and monocyte adsorptive apheresis, still requires large-scale trials to determine whether or not it is effective.[137] Results from small trials have been tentatively positive.[138]
Notable cases
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 "Ulcerative Colitis". NIDDK. September 2014. Archived from the original on 28 July 2016. Retrieved 3 August 2016.
- 1 2 3 4 Wanderås MH, Moum BA, Høivik ML, Hovde Ø (May 2016). "Predictive factors for a severe clinical course in ulcerative colitis: Results from population-based studies". World Journal of Gastrointestinal Pharmacology and Therapeutics. 7 (2): 235–41. doi:10.4292/wjgpt.v7.i2.235. PMC 4848246. PMID 27158539.
- ↑ Runge, Marschall S.; Greganti, M. Andrew (2008). Netter's Internal Medicine E-Book. Elsevier Health Sciences. p. 428. ISBN 9781437727722. Archived from the original on 27 August 2021. Retrieved 27 July 2020.
- 1 2 Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG (January 2012). "Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review". Gastroenterology. 142 (1): 46–54.e42, quiz e30. doi:10.1053/j.gastro.2011.10.001. PMID 22001864.
- 1 2 Wang H, Naghavi M, Allen C, Barber RM, Bhutta ZA, Carter A, et al. (GBD 2015 Mortality and Causes of Death Collaborators) (October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- 1 2 3 4 5 6 7 8 Ford AC, Moayyedi P, Hanauer SB (February 2013). "Ulcerative colitis". BMJ. 346: f432. doi:10.1136/bmj.f432. PMID 23386404. S2CID 14778938.
- 1 2 3 Akiho H, Yokoyama A, Abe S, Nakazono Y, Murakami M, Otsuka Y, Fukawa K, Esaki M, Niina Y, Ogino H (November 2015). "Promising biological therapies for ulcerative colitis: A review of the literature". World Journal of Gastrointestinal Pathophysiology. 6 (4): 219–27. doi:10.4291/wjgp.v6.i4.219. PMC 4644886. PMID 26600980.
- 1 2 3 4 5 6 7 8 9 10 11 Danese S, Fiocchi C (November 2011). "Ulcerative colitis". The New England Journal of Medicine. 365 (18): 1713–25. doi:10.1056/NEJMra1102942. PMID 22047562.
- 1 2 Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators) (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- 1 2 Adams, James G. (2012). Emergency Medicine E-Book: Clinical Essentials (Expert Consult – Online). Elsevier Health Sciences. p. 304. ISBN 978-1455733941. Archived from the original on 16 March 2020. Retrieved 27 July 2020.
- 1 2 3 4 5 6 internetmedicin.se > Inflammatorisk tarmsjukdom, kronisk, IBD By Robert Löfberg. Retrieved Oct 2010 Translate.
- 1 2 3 4 Hanauer SB, Sandborn W (1 March 2001). "Management of Crohn's disease in adults" (PDF). American Journal of Gastroenterology. 96 (3): 635–43. doi:10.1111/j.1572-0241.2001.03671.x. PMID 11280528. Retrieved 7 November 2009.
- 1 2 3 4 5 Magro, Fernando; Gionchetti, Paolo; Eliakim, Rami; Ardizzone, Sandro; Armuzzi, Alessandro; Barreiro-de Acosta, Manuel; Burisch, Johan; Gecse, Krisztina B.; Hart, Ailsa L.; Hindryckx, Pieter; Langner, Cord (1 June 2017). "Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders". Journal of Crohn's and Colitis. 11 (6): 649–670. doi:10.1093/ecco-jcc/jjx008. ISSN 1873-9946. PMID 28158501. Archived from the original on 22 July 2020. Retrieved 27 July 2020.
- ↑ Hanauer SB (March 1996). "Inflammatory bowel disease". The New England Journal of Medicine. 334 (13): 841–8. doi:10.1056/NEJM199603283341307. PMID 8596552. Archived from the original on 28 April 2021. Retrieved 27 July 2020.
- ↑ Rosenberg, L; Lawlor, GO; Zenlea, T; Goldsmith, JD; Gifford, A; Falchuk, KR; Wolf, JL; Cheifetz, AS; Robson, SC; Moss, AC (2013). "Predictors of endoscopic inflammation in patients with ulcerative colitis in clinical remission". Inflammatory Bowel Diseases. 19 (4): 779–84. doi:10.1097/MIB.0b013e3182802b0e. PMC 3749843. PMID 23446338.
- ↑ Haskell, H; Andrews CW, Jr; Reddy, SI; Dendrinos, K; Farraye, FA; Stucchi, AF; Becker, JM; Odze, RD (November 2005). "Pathologic features and clinical significance of "backwash" ileitis in ulcerative colitis". The American Journal of Surgical Pathology. 29 (11): 1472–81. doi:10.1097/01.pas.0000176435.19197.88. PMID 16224214. S2CID 42108108.
- 1 2 Fauci et al. Harrison's Internal Medicine, 17th ed. New York: McGraw-Hill Medical, 2008. ISBN 978-0-07-159991-7
- 1 2 3 4 5 6 Kornbluth A, Sachar DB (July 2004). "Ulcerative colitis practice guidelines in adults (update): American College of Gastroenterology, Practice Parameters Committee". The American Journal of Gastroenterology. 99 (7): 1371–85. PMID 15233681.
- ↑ Greenstein AJ, Janowitz HD, Sachar DB (September 1976). "The extra-intestinal complications of Crohn's disease and ulcerative colitis: a study of 700 patients". Medicine (Baltimore). 55 (5): 401–12. doi:10.1097/00005792-197609000-00004. PMID 957999.
- ↑ Bernstein, Charles N; Blanchard, James F; Rawsthorne, Patricia; Yu, Nancy (April 2001). "The Prevalence of Extraintestinal Diseases in Inflammatory Bowel Disease: A Population-Based Study:". American Journal of Gastroenterology. 96 (4): 1116–1122. doi:10.1111/j.1572-0241.2001.03756.x. PMID 11316157.
- ↑ Harbord, Marcus; Annese, Vito; Vavricka, Stephan R.; Allez, Matthieu; Barreiro-de Acosta, Manuel; Boberg, Kirsten Muri; Burisch, Johan; De Vos, Martine; De Vries, Anne-Marie; Dick, Andrew D.; Juillerat, Pascal; Karlsen, Tom H.; Koutroubakis, Ioannis; Lakatos, Peter L.; Orchard, Tim; Papay, Pavol; Raine, Tim; Reinshagen, Max; Thaci, Diamant; Tilg, Herbert; Carbonnel, Franck (1 March 2016). "The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease". Journal of Crohn's and Colitis. 10 (3): 239–254. doi:10.1093/ecco-jcc/jjv213. PMID 26614685.
- ↑ Langan RC, Gotsch PB, Krafczyk MA, Skillinge DD (November 2007). "Ulcerative colitis: diagnosis and treatment" (PDF). American Family Physician. 76 (9): 1323–30. PMID 18019875. Archived (PDF) from the original on 20 May 2013.
- ↑ Olsson R, Danielsson A, Järnerot G, Lindström E, Lööf L, Rolny P, Rydén BO, Tysk C, Wallerstedt S (May 1991). "Prevalence of primary sclerosing cholangitis in patients with ulcerative colitis". Gastroenterology. 100 (5 Pt 1): 1319–23. doi:10.1016/0016-5085(91)90784-I. PMID 2013375.
- 1 2 3 4 5 6 7 8 Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD (March 2019). "ACG Clinical Guideline: Ulcerative Colitis in Adults". Am. J. Gastroenterol. 114 (3): 384–413. doi:10.14309/ajg.0000000000000152. PMID 30840605.

- ↑ Nachimuthu, Senthil. "Crohn's disease". eMedicineHealth. Archived from the original on 9 December 2019. Retrieved 8 December 2019.
- ↑ Ko IK, Kim BG, Awadallah A, Mikulan J, Lin P, Letterio JJ, Dennis JE (July 2010). "Targeting improves MSC treatment of inflammatory bowel disease". Molecular Therapy. 18 (7): 1365–72. doi:10.1038/mt.2010.54. PMC 2911249. PMID 20389289.
- 1 2 Orholm M, Binder V, Sørensen TI, Rasmussen LP, Kyvik KO (October 2000). "Concordance of inflammatory bowel disease among Danish twins. Results of a nationwide study". Scandinavian Journal of Gastroenterology. 35 (10): 1075–81. doi:10.1080/003655200451207. PMID 11099061.
- ↑ Tysk C, Lindberg E, Järnerot G, Flodérus-Myrhed B (July 1988). "Ulcerative colitis and Crohn's disease in an unselected population of monozygotic and dizygotic twins. A study of heritability and the influence of smoking". Gut. 29 (7): 990–6. doi:10.1136/gut.29.7.990. PMC 1433769. PMID 3396969.
- 1 2 3 Baumgart DC, Sandborn WJ (May 2007). "Inflammatory bowel disease: clinical aspects and established and evolving therapies". The Lancet. 369 (9573): 1641–57. doi:10.1016/S0140-6736(07)60751-X. PMID 17499606. Retrieved 4 November 2009.
- ↑ Cho JH, Nicolae DL, Ramos R, Fields CT, Rabenau K, Corradino S, Brant SR, Espinosa R, LeBeau M, Hanauer SB, Bodzin J, Bonen DK (May 2000). "Linkage and linkage disequilibrium in chromosome band 1p36 in American Chaldeans with inflammatory bowel disease" (PDF). Human Molecular Genetics. 9 (9): 1425–32. doi:10.1093/hmg/9.9.1425. PMID 10814724.
- ↑ Sieg, I; Beckh, K; Kersten, U; Doss, MO (November 1991). "Manifestation of acute intermittent porphyria in patients with chronic inflammatory bowel disease". Zeitschrift fur Gastroenterologie. 29 (11): 602–5. PMID 1771936.
- ↑ Corrao G, Tragnone A, Caprilli R, Trallori G, Papi C, Andreoli A, Di Paolo M, Riegler G, Rigo GP, Ferraù O, Mansi C, Ingrosso M, Valpiani D (June 1998). "Risk of inflammatory bowel disease attributable to smoking, oral contraception and breastfeeding in Italy: a nationwide case-control study. Cooperative Investigators of the Italian Group for the Study of the Colon and the Rectum (GISC)" (PDF). International Journal of Epidemiology. 27 (3): 397–404. doi:10.1093/ije/27.3.397. PMID 9698126. Archived (PDF) from the original on 11 May 2020. Retrieved 27 July 2020.
- ↑ Wolverton SE, Harper JC (April 2013). "Important controversies associated with isotretinoin therapy for acne". American Journal of Clinical Dermatology. 14 (2): 71–6. doi:10.1007/s40257-013-0014-z. PMID 23559397. S2CID 918753.
- ↑ Järnerot G, Järnmark I, Nilsson K (November 1983). "Consumption of refined sugar by patients with Crohn's disease, ulcerative colitis, or irritable bowel syndrome". Scandinavian Journal of Gastroenterology. 18 (8): 999–1002. doi:10.3109/00365528309181832. PMID 6673083.
- ↑ Geerling BJ, Dagnelie PC, Badart-Smook A, Russel MG, Stockbrügger RW, Brummer RJ (April 2000). "Diet as a risk factor for the development of ulcerative colitis". The American Journal of Gastroenterology. 95 (4): 1008–13. PMID 10763951.
- ↑ Jowett SL, Seal CJ, Pearce MS, Phillips E, Gregory W, Barton JR, Welfare MR (October 2004). "Influence of dietary factors on the clinical course of ulcerative colitis: a prospective cohort study". Gut. 53 (10): 1479–84. doi:10.1136/gut.2003.024828. PMC 1774231. PMID 15361498.
- ↑ Andersen V, Olsen A, Carbonnel F, Tjønneland A, Vogel U (March 2012). "Diet and risk of inflammatory bowel disease". Digestive and Liver Disease. 44 (3): 185–94. doi:10.1016/j.dld.2011.10.001. PMID 22055893.
- ↑ Tilg H, Kaser A (October 2004). "Diet and relapsing ulcerative colitis: take off the meat?". Gut. 53 (10): 1399–401. doi:10.1136/gut.2003.035287. PMC 1774255. PMID 15361484.
- ↑ Moore J, Babidge W, Millard S, Roediger W (January 1998). "Colonic luminal hydrogen sulfide is not elevated in ulcerative colitis". Digestive Diseases and Sciences. 43 (1): 162–5. doi:10.1023/A:1018848709769. PMID 9508519. S2CID 20919357.
- ↑ Jørgensen J, Mortensen PB (August 2001). "Hydrogen sulfide and colonic epithelial metabolism: implications for ulcerative colitis". Digestive Diseases and Sciences. 46 (8): 1722–32. doi:10.1023/A:1010661706385. PMID 11508674. S2CID 30373968.
- ↑ Picton R, Eggo MC, Langman MJ, Singh S (February 2007). "Impaired detoxication of hydrogen sulfide in ulcerative colitis?". Digestive Diseases and Sciences. 52 (2): 373–8. doi:10.1007/s10620-006-9529-y. PMID 17216575. S2CID 22547709.
- 1 2 Roediger WE, Moore J, Babidge W (August 1997). "Colonic sulfide in pathogenesis and treatment of ulcerative colitis". Digestive Diseases and Sciences. 42 (8): 1571–9. doi:10.1023/A:1018851723920. PMID 9286219. S2CID 25496705.
- ↑ Pierce, ES (2018). "Could Mycobacterium avium subspecies paratuberculosis cause Crohn's disease, ulcerative colitis…and colorectal cancer?". Infectious Agents and Cancer. 13: 1. doi:10.1186/s13027-017-0172-3. PMC 5753485. PMID 29308085.
- ↑ Elson CO, Cong Y, Weaver CT, Schoeb TR, McClanahan TK, Fick RB, Kastelein RA (2007). "Monoclonal anti-interleukin 23 reverses active colitis in a T cell-mediated model in mice". Gastroenterology. 132 (7): 2359–70. doi:10.1053/j.gastro.2007.03.104. PMID 17570211.
- ↑ Levine J, Ellis CJ, Furne JK, Springfield J, Levitt MD (January 1998). "Fecal hydrogen sulfide production in ulcerative colitis". The American Journal of Gastroenterology. 93 (1): 83–7. PMID 9448181.
- ↑ Ulcerative colitis at eMedicine
- ↑ Walmsley RS, Ayres RC, Pounder RE, Allan RN (July 1998). "A simple clinical colitis activity index". Gut. 43 (1): 29–32. doi:10.1136/gut.43.1.29. PMC 1727189. PMID 9771402.
- ↑ Mardini HE, Grigorian AY (September 2014). "Probiotic mix VSL#3 is effective adjunctive therapy for mild to moderately active ulcerative colitis: a meta-analysis". Inflammatory Bowel Diseases. 20 (9): 1562–7. doi:10.1097/MIB.0000000000000084. PMID 24918321. S2CID 36218602.
- ↑ Del Pinto, R; Pietropaoli, D; Chandar, AK; Ferri, C; Cominelli, F (November 2015). "Association Between Inflammatory Bowel Disease and Vitamin D Deficiency: A Systematic Review and Meta-analysis". Inflammatory Bowel Diseases. 21 (11): 2708–17. doi:10.1097/MIB.0000000000000546. PMC 4615394. PMID 26348447.
- ↑ Shirley DA, Moonah S (July 2016). "Fulminant Amebic Colitis after Corticosteroid Therapy: A Systematic Review". PLOS Neglected Tropical Diseases. 10 (7): e0004879. doi:10.1371/journal.pntd.0004879. PMC 4965027. PMID 27467600.
- ↑ Kumar V, Soni P, Garg M, Abduraimova M, Harris J (12 June 2017). "Kaposi Sarcoma Mimicking Acute Flare of Ulcerative Colitis". Journal of Investigative Medicine High Impact Case Reports. 5 (2): 2324709617713510. doi:10.1177/2324709617713510. PMC 5470652. PMID 28638838.
- ↑ Tremaine, WJ (April 2012). "Is indeterminate colitis determinable?". Current Gastroenterology Reports. 14 (2): 162–5. doi:10.1007/s11894-012-0244-x. PMID 22314810. S2CID 40346031.
- 1 2 Rubin, DT; Ananthakrishnan, AN; Siegel, CA; Sauer, BG; Long, MD (March 2019). "ACG Clinical Guideline: Ulcerative Colitis in Adults". The American journal of gastroenterology. 114 (3): 384–413. doi:10.14309/ajg.0000000000000152. PMID 30840605.
- ↑ Broomé U, Bergquist A (February 2006). "Primary sclerosing cholangitis, inflammatory bowel disease, and colon cancer". Seminars in Liver Disease. 26 (1): 31–41. doi:10.1055/s-2006-933561. PMID 16496231.
- ↑ Shepherd NA (August 2002). "Granulomas in the diagnosis of intestinal Crohn's disease: a myth exploded?". Histopathology. 41 (2): 166–8. doi:10.1046/j.1365-2559.2002.01441.x. PMID 12147095.
- ↑ Mahadeva U, Martin JP, Patel NK, Price AB (July 2002). "Granulomatous ulcerative colitis: a re-appraisal of the mucosal granuloma in the distinction of Crohn's disease from ulcerative colitis". Histopathology. 41 (1): 50–5. doi:10.1046/j.1365-2559.2002.01416.x. PMID 12121237.
- ↑ DeRoche, TC; Xiao, SY; Liu, X (August 2014). "Histological evaluation in ulcerative colitis". Gastroenterology report. 2 (3): 178–92. doi:10.1093/gastro/gou031. PMID 24942757.
- ↑ Chen JH, Andrews JM, Kariyawasam V, Moran N, Gounder P, Collins G, Walsh AJ, Connor S, Lee TW, Koh CE, Chang J, Paramsothy S, Tattersall S, Lemberg DA, Radford-Smith G, Lawrance IC, McLachlan A, Moore GT, Corte C, Katelaris P, Leong RW (July 2016). "Review article: acute severe ulcerative colitis – evidence-based consensus statements". Alimentary Pharmacology & Therapeutics. 44 (2): 127–44. doi:10.1111/apt.13670. PMID 27226344.
- ↑ "Should You Try a Low-Residue Diet?". WebMD. WebMD. 25 October 2016. Archived from the original on 16 March 2017. Retrieved 29 April 2017.
- ↑ Manual of Clinical Nutrition Management (PDF). Compass Group. 2013. Archived (PDF) from the original on 29 November 2015.
- ↑ Feuerstein, JD; Isaacs, KL; Schneider, Y; Siddique, SM; Falck-Ytter, Y; Singh, S; American Gastroenterological Association Institute Clinical Guidelines Committee. Electronic address, clinicalpractice@gastro.org. (13 January 2020). "AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis". Gastroenterology. 158 (5): 1450–1461. doi:10.1053/j.gastro.2020.01.006. PMC 7175923. PMID 31945371.
- 1 2 Axelrad JE, Lichtiger S, Yajnik V (May 2016). "Inflammatory bowel disease and cancer: The role of inflammation, immunosuppression, and cancer treatment". World Journal of Gastroenterology (Review). 22 (20): 4794–801. doi:10.3748/wjg.v22.i20.4794. PMC 4873872. PMID 27239106.
- ↑ Jiang, Y; Lin, O; Sinha, SR (June 2017). "Use of Tumor Necrosis Factor Alpha Inhibitors for Inflammatory Bowel Disease Patients with Concurrent Heart Failure". Digestive Diseases and Sciences. 62 (6): 1597–1606. doi:10.1007/s10620-017-4574-2. PMID 28417241. S2CID 9536863.
- ↑ "Uceris Approved for Active Ulcerative Colitis". empr.com. 16 January 2013. Archived from the original on 18 January 2013. Retrieved 16 January 2013.
- ↑ "FDA approves new treatment for moderately to severely active ulcerative colitis". U.S. Food and Drug Administration (FDA) (Press release). 30 May 2018. Archived from the original on 15 December 2019. Retrieved 31 May 2018.
- ↑ Chande N, Wang Y, MacDonald JK, McDonald JW (August 2014). "Methotrexate for induction of remission in ulcerative colitis". The Cochrane Database of Systematic Reviews. 8 (8): CD006618. doi:10.1002/14651858.CD006618.pub3. PMC 6486224. PMID 25162749.
- ↑ Krishnamoorthy, R; Abrams, K R; Guthrie, N; Samuel, S; Thomas, T (28 May 2012). "PWE-237 Ciclosporin in acute severe ulcerative colitis: a meta-analysis". Gut. 61 (Suppl 2): A394.2–A394. doi:10.1136/gutjnl-2012-302514d.237. S2CID 74798482.
- ↑ Ogata H, Kato J, Hirai F, Hida N, Matsui T, Matsumoto T, Koyanagi K, Hibi T (May 2012). "Double-blind, placebo-controlled trial of oral tacrolimus (FK506) in the management of hospitalized patients with steroid-refractory ulcerative colitis". Inflammatory Bowel Diseases. 18 (5): 803–8. doi:10.1002/ibd.21853. PMID 21887732. S2CID 1294555.
- ↑ Lichtiger, S; Present, DH; Kornbluth, A; Gelernt, I; Bauer, J; Galler, G; Michelassi, F; Hanauer, S (30 June 1994). "Cyclosporine in severe ulcerative colitis refractory to steroid therapy". The New England Journal of Medicine. 330 (26): 1841–5. doi:10.1056/NEJM199406303302601. PMID 8196726.
- ↑ Weisshof, R; Ollech, JE; El Jurdi, K; Yvellez, OV; Cohen, RD; Sakuraba, A; Dalal, S; Pekow, J; Rubin, DT (19 September 2019). "Ciclosporin Therapy After Infliximab Failure in Hospitalized Patients With Acute Severe Colitis is Effective and Safe". Journal of Crohn's & Colitis. 13 (9): 1105–1110. doi:10.1093/ecco-jcc/jjz032. PMID 30726894.
- ↑ Azad Khan AK, Piris J, Truelove SC (October 1977). "An experiment to determine the active therapeutic moiety of sulphasalazine". Lancet. 2 (8044): 892–5. doi:10.1016/s0140-6736(77)90831-5. PMID 72239.
- ↑ Wang Y, Parker CE, Bhanji T, Feagan BG, MacDonald JK (April 2016). "Oral 5-aminosalicylic acid for induction of remission in ulcerative colitis". The Cochrane Database of Systematic Reviews. 4: CD000543. doi:10.1002/14651858.CD000543.pub4. PMC 7045743. PMID 27101467.
- ↑ Wang Y, Parker CE, Feagan BG, MacDonald JK (May 2016). "Oral 5-aminosalicylic acid for maintenance of remission in ulcerative colitis". The Cochrane Database of Systematic Reviews (5): CD000544. doi:10.1002/14651858.CD000544.pub4. PMC 7045447. PMID 27158764.
- ↑ Marshall JK, Thabane M, Steinhart AH, Newman JR, Anand A, Irvine EJ (November 2012). "Rectal 5-aminosalicylic acid for maintenance of remission in ulcerative colitis". The Cochrane Database of Systematic Reviews. 11: CD004118. doi:10.1002/14651858.CD004118.pub2. PMID 23152224.
- ↑ Salahudeen, MS (June 2019). "A review of current evidence allied to step-up and top-down medication therapy in inflammatory bowel disease". Drugs of Today (Barcelona, Spain : 1998). 55 (6): 385–405. doi:10.1358/dot.2019.55.6.2969816. PMID 31250843.
- ↑ Stevens, JP; Ballengee, CR; Chandradevan, R; Thompson, AB; Schoen, BT; Kugathasan, S; Sauer, CG (October 2019). "Performance of Interferon-Gamma Release Assays for Tuberculosis Screening in Pediatric Inflammatory Bowel Disease". Journal of Pediatric Gastroenterology and Nutrition. 69 (4): e111–e116. doi:10.1097/MPG.0000000000002428. PMID 31261245.
- ↑ Lee, CK; Wong, SHV; Lui, G; Tang, W; Tam, LS; Ip, M; Hung, E; Chen, M; Wu, JC; Ng, SC (30 July 2018). "A Prospective Study to Monitor for Tuberculosis During Anti-tumour Necrosis Factor Therapy in Patients With Inflammatory Bowel Disease and Immune-mediated Inflammatory Diseases". Journal of Crohn's & Colitis. 12 (8): 954–962. doi:10.1093/ecco-jcc/jjy057. PMID 29757355. S2CID 21673794.
- ↑ Calkins BM (December 1989). "A meta-analysis of the role of smoking in inflammatory bowel disease". Digestive Diseases and Sciences. 34 (12): 1841–54. doi:10.1007/BF01536701. PMID 2598752. S2CID 5775169.
- ↑ Lakatos PL, Szamosi T, Lakatos L (December 2007). "Smoking in inflammatory bowel diseases: good, bad or ugly?". World Journal of Gastroenterology. 13 (46): 6134–9. doi:10.3748/wjg.13.6134. PMC 4171221. PMID 18069751.
- ↑ Calabrese, E; Yanai, H; Shuster, D; Rubin, DT; Hanauer, SB (August 2012). "Low-dose smoking resumption in ex-smokers with refractory ulcerative colitis". Journal of Crohn's & Colitis. 6 (7): 756–62. doi:10.1016/j.crohns.2011.12.010. PMID 22398093.
- ↑ Guslandi M (October 1999). "Nicotine treatment for ulcerative colitis". British Journal of Clinical Pharmacology. 48 (4): 481–4. doi:10.1046/j.1365-2125.1999.00039.x. PMC 2014383. PMID 10583016.
- ↑ Sandborn WJ, Tremaine WJ, Offord KP, Lawson GM, Petersen BT, Batts KP, Croghan IT, Dale LC, Schroeder DR, Hurt RD (March 1997). "Transdermal nicotine for mildly to moderately active ulcerative colitis. A randomized, double-blind, placebo-controlled trial". Annals of Internal Medicine. 126 (5): 364–71. doi:10.7326/0003-4819-126-5-199703010-00004. PMID 9054280. S2CID 25745900.
- ↑ Bonapace, CR; Mays, DA (1997). "The effect of mesalamine and nicotine in the treatment of inflammatory bowel disease". The Annals of Pharmacotherapy. 31 (7–8): 907–13. doi:10.1177/106002809703100719. PMID 9220055. S2CID 24122049.
- ↑ Kennedy, LD (September 1996). "Nicotine therapy for ulcerative colitis". The Annals of Pharmacotherapy. 30 (9): 1022–3. PMID 8876866.
- ↑ Rubin, DT; Hanauer, SB (August 2000). "Smoking and inflammatory bowel disease". European Journal of Gastroenterology & Hepatology. 12 (8): 855–62. doi:10.1097/00042737-200012080-00004. PMID 10958212.
- 1 2 Goddard AF, James MW, McIntyre AS, Scott BB (October 2011). "Guidelines for the management of iron deficiency anaemia". Gut. 60 (10): 1309–16. doi:10.1136/gut.2010.228874. PMID 21561874.
- ↑ Inflamm Bowel Dis 2007;13:1545–1553
- ↑ Mowat C, Cole A, Windsor A, Ahmad T, Arnott I, Driscoll R, Mitton S, Orchard T, Rutter M, Younge L, Lees C, Ho GT, Satsangi J, Bloom S (May 2011). "Guidelines for the management of inflammatory bowel disease in adults". Gut. 60 (5): 571–607. doi:10.1136/gut.2010.224154. PMID 21464096. S2CID 8269837.
- 1 2 Agabegi, Elizabeth D; Agabegi, Steven S. (2008). "Inflammatory bowel disease (IBD)". Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. pp. 152–156. ISBN 0-7817-7153-6.
{{cite book}}: Unknown parameter|name-list-format=ignored (help) - ↑ Feller M, Huwiler K, Schoepfer A, Shang A, Furrer H, Egger M (February 2010). "Long-term antibiotic treatment for Crohn's disease: systematic review and meta-analysis of placebo-controlled trials". Clinical Infectious Diseases. 50 (4): 473–80. doi:10.1086/649923. PMID 20067425.
- ↑ Prantera C, Scribano ML (July 2009). "Antibiotics and probiotics in inflammatory bowel disease: why, when, and how". Current Opinion in Gastroenterology. 25 (4): 329–33. doi:10.1097/MOG.0b013e32832b20bf. PMID 19444096.
- ↑ "Colectomy Not a Final Cure for Ulcerative Colitis, Data Show". www.mdedge.com. Archived from the original on 27 August 2021. Retrieved 15 December 2019.
- ↑ Pappou, Emmanouil P.; Kiran, Ravi P. (June 2016). "The Failed J Pouch". Clinics in Colon and Rectal Surgery. 29 (2): 123–129. doi:10.1055/s-0036-1580724. ISSN 1531-0043. PMC 4882179. PMID 27247537.
- ↑ Fedorak RN (November 2010). "Probiotics in the management of ulcerative colitis". Gastroenterology & Hepatology. 6 (11): 688–90. PMC 3033537. PMID 21437015.
- ↑ Northwestern University (2011). "New Probiotics Combats Inflammatory Bowel Disease". Science Daily. Archived from the original on 15 December 2013.
- ↑ Borody TJ, Brandt LJ, Paramsothy S (January 2014). "Therapeutic faecal microbiota transplantation: current status and future developments". Current Opinion in Gastroenterology. 30 (1): 97–105. doi:10.1097/MOG.0000000000000027. PMC 3868025. PMID 24257037.
- ↑ Narula N, Kassam Z, Yuan Y, Colombel JF, Ponsioen C, Reinisch W, et al. (October 2017). "Systematic Review and Meta-analysis: Fecal Microbiota Transplantation for Treatment of Active Ulcerative Colitis". Inflamm. Bowel Dis. 23 (10): 1702–1709. doi:10.1097/MIB.0000000000001228. PMID 28906291.
- ↑ Shi Y, Dong Y, Huang W, Zhu D, Mao H, Su P (2016). "Fecal Microbiota Transplantation for Ulcerative Colitis: A Systematic Review and Meta-Analysis". PLOS ONE. 11 (6): e0157259. Bibcode:2016PLoSO..1157259S. doi:10.1371/journal.pone.0157259. PMC 4905678. PMID 27295210.
- ↑ Costello SP, Hughes PA, Waters O, Bryant RV, Vincent AD, Blatchford P, et al. (January 2019). "Effect of Fecal Microbiota Transplantation on 8-Week Remission in Patients With Ulcerative Colitis: A Randomized Clinical Trial". JAMA. 321 (2): 156–164. doi:10.1001/jama.2018.20046. PMC 6439766. PMID 30644982.
- ↑ Borody TJ, Warren EF, Leis S, Surace R, Ashman O (July 2003). "Treatment of ulcerative colitis using fecal bacteriotherapy" (PDF). Journal of Clinical Gastroenterology. 37 (1): 42–7. doi:10.1097/00004836-200307000-00012. PMID 12811208. S2CID 1048312. Archived from the original (PDF) on 9 April 2013.
- 1 2 Kumar S, Ahuja V, Sankar MJ, Kumar A, Moss AC (October 2012). "Curcumin for maintenance of remission in ulcerative colitis". The Cochrane Database of Systematic Reviews. 10: CD008424. doi:10.1002/14651858.CD008424.pub2. PMC 4001731. PMID 23076948.
- ↑ Kevans, David; Murthy, Sanjay; Mould, Diane R.; Silverberg, Mark S. (25 May 2018). "Accelerated Clearance of Infliximab is Associated With Treatment Failure in Patients With Corticosteroid-Refractory Acute Ulcerative Colitis". Journal of Crohn's and Colitis. 12 (6): 662–669. doi:10.1093/ecco-jcc/jjy028. ISSN 1873-9946. PMID 29659758. Archived from the original on 28 April 2021. Retrieved 27 July 2020.
- ↑ Horio, Yuki; Uchino, Motoi; Bando, Toshihiro; Chohno, Teruhiro; Sasaki, Hirofumi; Hirata, Akihiro; Takesue, Yoshio; Ikeuchi, Hiroki (19 May 2017). "Rectal-sparing type of ulcerative colitis predicts lack of response to pharmacotherapies". BMC Surgery. 17 (1): 59. doi:10.1186/s12893-017-0255-5. ISSN 1471-2482. PMC 5437574. PMID 28526076.
- ↑ Mark T. Osterman, Gary R. Liechtenstein. Ulcerative Colitis, Chapter 116, pp.2023–2061. In: Sleisenger and Fordtran's Gastrointestinal and Liver Disease, 10th edition, 2016. eds Mark Feldman, Lawrence S. Friedman, Lawrence J. Brandt.
- ↑ Patil, DT; Odze, RD (August 2017). "Backwash Is Hogwash: The Clinical Significance of Ileitis in Ulcerative Colitis". The American Journal of Gastroenterology. 112 (8): 1211–1214. doi:10.1038/ajg.2017.182. PMID 28631729. S2CID 10801391.
- ↑ Leighton JA, Shen B, Baron TH, Adler DG, Davila R, Egan JV, Faigel DO, Gan SI, Hirota WK, Lichtenstein D, Qureshi WA, Rajan E, Zuckerman MJ, VanGuilder T, Fanelli RD (April 2006). "ASGE guideline: endoscopy in the diagnosis and treatment of inflammatory bowel disease". Gastrointestinal Endoscopy. 63 (4): 558–65. doi:10.1016/j.gie.2006.02.005. PMID 16564852.
- 1 2 Jess T, Gamborg M, Munkholm P, Sørensen TI (March 2007). "Overall and cause-specific mortality in ulcerative colitis: meta-analysis of population-based inception cohort studies". The American Journal of Gastroenterology. 102 (3): 609–17. PMID 17156150.
- ↑ da Silva, BC; Lyra, AC; Rocha, R; Santana, GO (28 July 2014). "Epidemiology, demographic characteristics and prognostic predictors of ulcerative colitis". World Journal of Gastroenterology. 20 (28): 9458–67. doi:10.3748/wjg.v20.i28.9458. PMC 4110577. PMID 25071340.
- ↑ Nguyen, M; Bradford, K; Zhang, X; Shih, DQ (1 January 2011). "Cytomegalovirus Reactivation in Ulcerative Colitis Patients". Ulcers. 2011: 1–7. doi:10.1155/2011/282507. PMC 3124815. PMID 21731826.
- ↑ Page 481 Archived 9 May 2013 at the Wayback Machine in: Colonic diseases. By Timothy R. Koch. 2003. ISBN 978-0-89603-961-2
- 1 2 Ungaro, R; Mehandru, S; Allen, PB; Peyrin-Biroulet, L; Colombel, JF (29 April 2017). "Ulcerative colitis". Lancet. 389 (10080): 1756–1770. doi:10.1016/S0140-6736(16)32126-2. PMC 6487890. PMID 27914657.
- ↑ Karlinger K, Györke T, Makö E, Mester A, Tarján Z (September 2000). "The epidemiology and the pathogenesis of inflammatory bowel disease". European Journal of Radiology. 35 (3): 154–67. doi:10.1016/s0720-048x(00)00238-2. PMID 11000558.
- ↑ Podolsky DK (August 2002). "Inflammatory bowel disease". The New England Journal of Medicine. 347 (6): 417–29. doi:10.1056/NEJMra020831. PMID 12167685. Archived from the original on 28 April 2021. Retrieved 27 July 2020.
- ↑ Schmidt JA, Marshall J, Hayman MJ (December 1985). "Identification and characterization of the chicken transferrin receptor". The Biochemical Journal. 232 (3): 735–41. doi:10.1042/bj2320735. PMC 1152945. PMID 3004417.
- ↑ Shivananda S, Lennard-Jones J, Logan R, Fear N, Price A, Carpenter L, van Blankenstein M (November 1996). "Incidence of inflammatory bowel disease across Europe: is there a difference between north and south? Results of the European Collaborative Study on Inflammatory Bowel Disease (EC-IBD)" (PDF). Gut. 39 (5): 690–7. doi:10.1136/gut.39.5.690. PMC 1383393. PMID 9014768. Archived (PDF) from the original on 4 June 2012.
- ↑ Sonnenberg A, McCarty DJ, Jacobsen SJ (January 1991). "Geographic variation of inflammatory bowel disease within the United States". Gastroenterology. 100 (1): 143–9. doi:10.1016/0016-5085(91)90594-B. PMID 1983816.
- ↑ Burisch, J; Pedersen, N; Čuković-Čavka, S; Brinar, M; Kaimakliotis, I; Duricova, D; Shonová, O; Vind, I; Avnstrøm, S; Thorsgaard, N; Andersen, V; Krabbe, S; Dahlerup, JF; Salupere, R; Nielsen, KR; Olsen, J; Manninen, P; Collin, P; Tsianos, EV; Katsanos, KH; Ladefoged, K; Lakatos, L; Björnsson, E; Ragnarsson, G; Bailey, Y; Odes, S; Schwartz, D; Martinato, M; Lupinacci, G; Milla, M; De Padova, A; D'Incà, R; Beltrami, M; Kupcinskas, L; Kiudelis, G; Turcan, S; Tighineanu, O; Mihu, I; Magro, F; Barros, LF; Goldis, A; Lazar, D; Belousova, E; Nikulina, I; Hernandez, V; Martinez-Ares, D; Almer, S; Zhulina, Y; Halfvarson, J; Arebi, N; Sebastian, S; Lakatos, PL; Langholz, E; Munkholm, P; EpiCom-group. (April 2014). "East-West gradient in the incidence of inflammatory bowel disease in Europe: the ECCO-EpiCom inception cohort". Gut. 63 (4): 588–97. doi:10.1136/gutjnl-2013-304636. PMID 23604131. S2CID 25069828. Archived from the original on 27 August 2021. Retrieved 27 July 2020.
- ↑ Andersson RE, Olaison G, Tysk C, Ekbom A (March 2001). "Appendectomy and protection against ulcerative colitis". The New England Journal of Medicine. 344 (11): 808–14. doi:10.1056/NEJM200103153441104. PMID 11248156.
- 1 2 Boyko EJ, Koepsell TD, Perera DR, Inui TS (March 1987). "Risk of ulcerative colitis among former and current cigarette smokers". The New England Journal of Medicine. 316 (12): 707–10. doi:10.1056/NEJM198703193161202. PMID 3821808.
- 1 2 "Epidemiology of the IBD". Centers for Disease Control and Prevention (CDC). Archived from the original on 23 February 2017. Retrieved 23 February 2017.
- ↑ Makhlouf GM, Zfass AM, Said SI, Schebalin M (April 1978). "Effects of synthetic vasoactive intestinal peptide (VIP), secretin and their partial sequences on gastric secretion". Proceedings of the Society for Experimental Biology and Medicine. 157 (4): 565–8. doi:10.3181/00379727-157-40097. PMID 349569. S2CID 40543366.
- ↑ "NICE clinical guideline and quality standard: Ulcerative colitis scope". National Institute for Health and Care Excellence, Ulcerative colitis: management Clinical guideline [CG166] (PDF). 5 September 2011. Archived from the original on 24 February 2017. Retrieved 24 February 2017.
- ↑ Summers RW, Elliott DE, Urban JF, Thompson RA, Weinstock JV (April 2005). "Trichuris suis therapy for active ulcerative colitis: a randomized controlled trial" (PDF). Gastroenterology. 128 (4): 825–32. doi:10.1053/j.gastro.2005.01.005. PMID 15825065. Archived from the original (PDF) on 14 January 2015. Retrieved 22 December 2012.
- ↑ Summers RW, Elliott DE, Urban JF, Thompson RA, Weinstock JV (April 2005). "Trichuris suis therapy for active ulcerative colitis: a randomized controlled trial". Gastroenterology. 128 (4): 825–32. doi:10.1053/j.gastro.2005.01.005. PMID 15825065.
- 1 2 Bennett CF, Condon TC, Grimm S, Chan H, Chiang MY (1994). "Inhibition of endothelial cell-leukocyte adhesion molecule expression with antisense oligonucleotides". The Journal of Immunology. 152 (1): 3530–40.
- ↑ Jones SC, Banks RE, Haidar A, Gearing AJ, Hemingway IK, Ibbotson SH, Dixon MF, Axon AT (May 1995). "Adhesion molecules in inflammatory bowel disease". Gut. 36 (5): 724–30. doi:10.1136/gut.36.5.724. PMC 1382677. PMID 7541009.
- ↑ van Deventer SJ, Wedel MK, Baker BF, Xia S, Chuang E, Miner PB (May 2006). "A phase II dose ranging, double-blind, placebo-controlled study of alicaforsen enema in subjects with acute exacerbation of mild to moderate left-sided ulcerative colitis". Alimentary Pharmacology & Therapeutics. 23 (10): 1415–25. doi:10.1111/j.1365-2036.2006.02910.x. PMID 16669956.
- ↑ Ghouri YA, Richards DM, Rahimi EF, Krill JT, Jelinek KA, DuPont AW (9 December 2014). "Systematic review of randomized controlled trials of probiotics, prebiotics, and synbiotics in inflammatory bowel disease". Clinical and Experimental Gastroenterology. 7: 473–87. doi:10.2147/CEG.S27530. PMC 4266241. PMID 25525379.
- 1 2 Strøbæk D, Brown DT, Jenkins DP, Chen YJ, Coleman N, Ando Y, Chiu P, Jørgensen S, Demnitz J, Wulff H, Christophersen P (January 2013). "NS6180, a new K(Ca) 3.1 channel inhibitor prevents T-cell activation and inflammation in a rat model of inflammatory bowel disease". British Journal of Pharmacology. 168 (2): 432–44. doi:10.1111/j.1476-5381.2012.02143.x. PMC 3572569. PMID 22891655.
- 1 2 Bennike, Tue Bjerg; Carlsen, Thomas Gelsing; Ellingsen, Torkell; Bonderup, Ole Kristian; Glerup, Henning; Bøgsted, Martin; Christiansen, Gunna; Birkelund, Svend; Stensballe, Allan; Andersen, Vibeke (September 2015). "Neutrophil Extracellular Traps in Ulcerative Colitis: A Proteome Analysis of Intestinal Biopsies". Inflammatory Bowel Diseases. 21 (9): 2052–2067. doi:10.1097/MIB.0000000000000460. ISSN 1078-0998. PMC 4603666. PMID 25993694.
- ↑ Kirov, Stefan; Sasson, Ariella; Zhang, Clarence; Chasalow, Scott; Dongre, Ashok; Steen, Hanno; Stensballe, Allan; Andersen, Vibeke; Birkelund, Svend; Bennike, Tue Bjerg (2019). "Degradation of the extracellular matrix is part of the pathology of ulcerative colitis". Molecular Omics. 15 (1): 67–76. doi:10.1039/C8MO00239H. ISSN 2515-4184. PMID 30702115.
- ↑ Raithel M, Winterkamp S, Weidenhiller M, Müller S, Hahn EG (July 2007). "Combination therapy using fexofenadine, disodium cromoglycate, and a hypoallergenic amino acid-based formula induced remission in a patient with steroid-dependent, chronically active ulcerative colitis". International Journal of Colorectal Disease. 22 (7): 833–9. doi:10.1007/s00384-006-0120-y. PMID 16944185. S2CID 2605447.
- 1 2 Dhaneshwar S, Gautam H (August 2012). "Exploring novel colon-targeting antihistaminic prodrug for colitis". Journal of Physiology and Pharmacology. 63 (4): 327–37. PMID 23070081.
- ↑ Vermeire, S; O'Byrne, S; Keir, M; Williams, M; Lu, TT; Mansfield, JC; Lamb, CA; Feagan, BG; Panes, J; Salas, A; Baumgart, DC; Schreiber, S; Dotan, I; Sandborn, WJ; Tew, GW; Luca, D; Tang, MT; Diehl, L; Eastham-Anderson, J; De Hertogh, G; Perrier, C; Egen, JG; Kirby, JA; van Assche, G; Rutgeerts, P (26 July 2014). "Etrolizumab as induction therapy for ulcerative colitis: a randomised, controlled, phase 2 trial". Lancet. 384 (9940): 309–18. doi:10.1016/S0140-6736(14)60661-9. PMID 24814090. S2CID 7369482.
- ↑ Rosenfeld, G; Parker, CE; MacDonald, JK; Bressler, B (2 December 2015). "Etrolizumab for induction of remission in ulcerative colitis". The Cochrane Database of Systematic Reviews (12): CD011661. doi:10.1002/14651858.CD011661.pub2. PMID 26630451.
- ↑ Makker, J; Hommes, DW (2016). "Etrolizumab for ulcerative colitis: the new kid on the block?". Expert Opinion on Biological Therapy. 16 (4): 567–72. doi:10.1517/14712598.2016.1158807. PMID 26914639. S2CID 24706213.
- ↑ Abreu MT, Plevy S, Sands BE, Weinstein R (2007). "Selective leukocyte apheresis for the treatment of inflammatory bowel disease". Journal of Clinical Gastroenterology. 41 (10): 874–88. doi:10.1097/MCG.0b013e3180479435. PMID 18090155. S2CID 36724094.
- ↑ Vernia P, D'Ovidio V, Meo D (October 2010). "Leukocytapheresis in the treatment of inflammatory bowel disease: Current position and perspectives". Transfusion and Apheresis Science. 43 (2): 227–9. doi:10.1016/j.transci.2010.07.023. PMID 20817610.
Further reading
- Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD (March 2019). "ACG Clinical Guideline: Ulcerative Colitis in Adults". Am. J. Gastroenterol. 114 (3): 384–413. doi:10.14309/ajg.0000000000000152. PMID 30840605. S2CID 73473272.
External links
| Classification | |
|---|---|
| External resources |
- MedlinePlus ulcerative colitis page Archived 5 July 2016 at the Wayback Machine
- Torpy JM, Lynm C, Golub RM (January 2012). "JAMA patient page. Ulcerative colitis". JAMA. 307 (1): 104. doi:10.1001/jama.2011.1889. PMID 22215172.