Appendix (anatomy)
| Appendix | |
|---|---|
 Drawing of colon with variability of appendix locations as seen from front | |
 Arteries of cecum and appendix (appendix labeled as vermiform process at lower right) | |
| Details | |
| Precursor | Midgut |
| System | Digestive system |
| Artery | Appendicular artery |
| Vein | Appendicular vein |
| Identifiers | |
| Latin | Appendix vermiformis |
| MeSH | D001065 |
| TA98 | A05.7.02.007 |
| TA2 | 2976 |
| FMA | 14542 |
| Anatomical terminology | |

The appendix (or vermiform appendix; also cecal [or caecal] appendix; vermix; or vermiform process) is a finger-like, blind-ended tube connected to the cecum, from which it develops in the embryo. The cecum is a pouch-like structure of the large intestine, located at the junction of the small and the large intestines. The term "vermiform" comes from Latin and means "worm-shaped." The appendix used to be considered a vestigial organ, but this view has changed over the past decades.[1] Research suggests that the appendix may serve an important purpose. In particular, it may serve as a reservoir for beneficial gut bacteria.
Structure

The human appendix averages 9 cm (3.5 in) in length but can range from 5 to 35 cm (2.0 to 13.8 in). The diameter of the appendix is 6 mm (0.24 in), and more than 6 mm (0.24 in) is considered a thickened or inflamed appendix. The longest appendix ever removed was 26 cm (10 in) long.[2] The appendix is usually located in the lower right quadrant of the abdomen, near the right hip bone. The base of the appendix is located 2 cm (0.79 in) beneath the ileocecal valve that separates the large intestine from the small intestine. Its position within the abdomen corresponds to a point on the surface known as McBurney's point.
The appendix is connected to the mesentery in the lower region of the ileum, by a short region of the mesocolon known as the mesoappendix.[3]
Variation
Some identical twins—known as mirror image twins—can have a mirror-imaged anatomy, a congenital condition with the appendix located in the lower left quadrant of the abdomen instead of the lower right.[4][5] Intestinal malrotation may also cause displacement of the appendix to the left side.
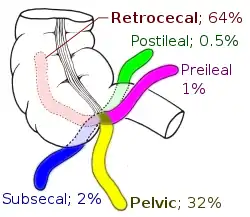
While the base of the appendix is typically located 2 cm (0.79 in) below the ileocecal valve, the tip of the appendix can be variably located—in the pelvis, outside the peritoneum or behind the cecum.[6] The prevalence of the different positions varies amongst populations with the retrocecal position being most common in Ghana and Sudan, with 67.3% and 58.3% occurrence respectively, in comparison to Iran and Bosnia where the pelvic position is most common, with 55.8% and 57.7% occurrence respectively.[7][8][9][10]
In very rare cases, the appendix may not be present at all (laparotomies for suspected appendicitis have given a frequency of 1 in 100,000).[11]
Sometimes there is a semi-circular fold of mucous membrane at the opening of the appendix. This valve of the vermiform appendix is also called Gerlach's valve.[3]
Functions
Maintaining gut flora
Although it has been long accepted that the immune tissue surrounding the appendix and elsewhere in the gut—called gut-associated lymphoid tissue—carries out a number of important functions, explanations were lacking for the distinctive shape of the appendix and its apparent lack of specific importance and function as judged by an absence of side effects following its removal.[12] Therefore, the notion that the appendix is only vestigial became widely held.
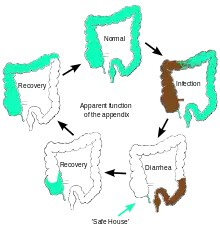
William Parker, Randy Bollinger, and colleagues at Duke University proposed in 2007 that the appendix serves as a haven for useful bacteria when illness flushes the bacteria from the rest of the intestines.[13][14] This proposition is based on an understanding that emerged by the early 2000s of how the immune system supports the growth of beneficial intestinal bacteria,[15][16] in combination with many well-known features of the appendix, including its architecture, its location just below the normal one-way flow of food and germs in the large intestine, and its association with copious amounts of immune tissue. Research performed at Winthrop–University Hospital showed that individuals without an appendix were four times as likely to have a recurrence of Clostridium difficile colitis.[17] The appendix, therefore, may act as a "safe house" for beneficial bacteria.[13] This reservoir of bacteria could then serve to repopulate the gut flora in the digestive system following a bout of dysentery or cholera or to boost it following a milder gastrointestinal illness.[14]
Immune and lymphatic systems
The appendix has been identified as an important component of mammalian mucosal immune function, particularly B cell-mediated immune responses and extrathymically derived T cells. This structure helps in the proper movement and removal of waste matter in the digestive system, contains lymphatic vessels that regulate pathogens, and lastly, might even produce early defences that prevent deadly diseases. Additionally, it is thought that this may provide more immune defences from invading pathogens and getting the lymphatic system's B and T cells to fight the viruses and bacteria that infect that portion of the bowel and training them so that immune responses are targeted and more able to reliably and less dangerously fight off pathogens.[18] In addition, there are different immune cells called innate lymphoid cells that function in the gut in order to help the appendix maintain digestive health.[19] Research also shows a positive correlation between the existence of appendix and the concentration of cecal lymphoid tissue, which supports that not only does the appendix evolve as a complex with the cecum but also has major immune benefits. [20]
Clinical significance

Common diseases of the appendix (in humans) are appendicitis and carcinoid tumors (appendiceal carcinoid).[21] Appendix cancer accounts for about 1 in 200 of all gastrointestinal malignancies. In rare cases, adenomas are also present.[22]
Appendicitis
Appendicitis is a condition characterized by inflammation of the appendix. Pain often begins in the center of the abdomen, corresponding to the appendix's development as part of the embryonic midgut. This pain is typically a dull, poorly localized, visceral pain.[23]
As the inflammation progresses, the pain begins to localize more clearly to the right lower quadrant, as the peritoneum becomes inflamed. This peritoneal inflammation, or peritonitis, results in rebound tenderness (pain upon removal of pressure rather than application of pressure). In particular, it presents at McBurney's point, 1/3 of the way along a line drawn from the anterior superior iliac spine to the umbilicus. Typically, point (skin) pain is not present until the parietal peritoneum is inflamed, as well. Fever and an immune system response are also characteristic of appendicitis.[23] Other signs and symptoms may include nausea and vomiting, low-grade fever that may get worse, constipation or diarrhea, abdominal bloating, or flatulence.[24]
Appendicitis usually requires the removal of the inflamed appendix, in an appendectomy either by laparotomy or laparoscopy. Untreated, the appendix may rupture, leading to peritonitis, followed by shock, and, if still untreated, death.[23]
Recently, practitioners reported good results in treating appendicitis without appendectomy. Managing appendicitis using only antibiotic treatment and cooling of the appendix was successful in first occurrence acute appendicitis without complication.[25]
Surgery
The surgical removal of the appendix is called an appendectomy. This removal is normally performed as an emergency procedure when the patient is suffering from acute appendicitis. In the absence of surgical facilities, intravenous antibiotics are used to delay or avoid the onset of sepsis. In some cases, the appendicitis resolves completely; more often, an inflammatory mass forms around the appendix. This is a relative contraindication to surgery.
The appendix is also used for the construction of an efferent urinary conduit, in an operation known as the Mitrofanoff procedure,[26] in people with a neurogenic bladder.
The appendix is also used as a means to access the colon in children with paralysed bowels or major rectal sphincter problems. The appendix is brought out to the skin surface and the child/parent can then attach a catheter and easily wash out the colon (via normal defaecation) using an appropriate solution.[27]
History
Charles Darwin suggested that the appendix was mainly used by earlier hominids for digesting fibrous vegetation, then evolved to take on a new purpose over time. The very long cecum of some herbivorous animals, such as in the horse or the koala, appears to support this hypothesis. The koala's cecum enables it to host bacteria that specifically help to break down cellulose. Human ancestors may have also relied upon this system when they lived on a diet rich in foliage. As people began to eat more easily digested foods, they may have become less reliant on cellulose-rich plants for energy. As the cecum became less necessary for digestion, mutations that were previously deleterious (and would have hindered evolutionary progress) were no longer important, so the mutations survived. It is suggested that these alleles became more frequent and the cecum continued to shrink. After millions of years, the once-necessary cecum degraded to be the appendix of modern humans.[28]
Dr. Heather F. Smith of Midwestern University and colleagues explained:
Recently ... improved understanding of gut immunity has merged with current thinking in biological and medical science, pointing to an apparent function of the mammalian cecal appendix as a safe-house for symbiotic gut microbes, preserving the flora during times of gastrointestinal infection in societies without modern medicine. This function is potentially a selective force for the evolution and maintenance of the appendix. Three morphotypes of cecal-appendices can be described among mammals based primarily on the shape of the cecum: a distinct appendix branching from a rounded or sac-like cecum (as in many primate species), an appendix located at the apex of a long and voluminous cecum (as in the rabbit, greater glider and Cape dune mole rat), and an appendix in the absence of a pronounced cecum (as in the wombat). In addition, long narrow appendix-like structures are found in mammals that either lack an apparent cecum (as in monotremes) or lack a distinct junction between the cecum and appendix-like structure (as in the koala). A cecal appendix has evolved independently at least twice, and apparently represents yet another example of convergence in morphology between Australian marsupials and placentals in the rest of the world. Although the appendix has apparently been lost by numerous species, it has also been maintained for more than 80 million years in at least one clade.[29]
In a 2013 paper, the appendix was found to have evolved at least 32 times (and perhaps as many as 38 times) and to have been lost no more than six times.[30] A more recent study using similar methods on an updated database yielded similar, though less spectacular results, with at least 29 gains and at the most 12 losses (all of which were ambiguous), and this is still significantly asymmetrical.[31] This suggests that the cecal appendix has a selective advantage in many situations and argues strongly against its vestigial nature. This complex evolutionary history of the appendix, along with a great heterogeneity in its evolutionary rate in various taxa, suggests that it is a recurrent trait.[32]
Such a function may be useful in a culture lacking modern sanitation and healthcare practice, where diarrhea may be prevalent. Current epidemiological data on the cause of death in developed countries collected by the World Health Organization in 2001 show that acute diarrhea is now the fourth leading cause of disease-related death in developing countries (data summarized by The Bill and Melinda Gates Foundation). Two of the other leading causes of death are expected to have exerted limited or no selection pressure.[33]
Additional images
 Illustration depicting the location of the appendix in a child
Illustration depicting the location of the appendix in a child Normal location of the appendix relative to other organs of the digestive system (frontal view)
Normal location of the appendix relative to other organs of the digestive system (frontal view) Vermiform appendix
Vermiform appendix Ileo-cecal valve and vermiform appendix
Ileo-cecal valve and vermiform appendix Mucinous adenocarcinoma of the appendix tip
Mucinous adenocarcinoma of the appendix tip Cross section of the appendix with Enterobius with H&E stain
Cross section of the appendix with Enterobius with H&E stain Histology of vermiform appendix
Histology of vermiform appendix Micrograph of entry point of appendicular arteries (arrows at level of inner muscular layer), not to be confused with a perforation.
Micrograph of entry point of appendicular arteries (arrows at level of inner muscular layer), not to be confused with a perforation.
See also
References
- ↑ Kooij IA, Sahami S, Meijer SL, Buskens CJ, Te Velde AA (October 2016). "The immunology of the vermiform appendix: a review of the literature". Clinical and Experimental Immunology. 186 (1): 1–9. doi:10.1111/cei.12821. PMC 5011360. PMID 27271818.
- ↑ "Largest appendix removed". Guinness World Records. Archived from the original on 26 November 2020. Retrieved 22 May 2017.
- 1 2 Golalipour, M.J.; Arya, B.; Jahanshahi, M.; Azarhoosh, R. (2003). "Anatomical Variations Of Vermiform Appendix In South-East Caspian Sea (Gorgan-IRAN)" (PDF). J. Anat. Soc. India. Archived (PDF) from the original on 11 July 2020. Retrieved 1 October 2014.
- ↑ "Unusual Types of Twins". Multiples of America. Archived from the original on 2 May 2014. Retrieved 30 April 2014.
- ↑ Gedda L, Sciacca A, Brenci G, Villatico S, Bonanni G, Gueli N, Talone C (1984). "Situs viscerum specularis in monozygotic twins". Acta Geneticae Medicae et Gemellologiae. 33 (1): 81–5. doi:10.1017/S0001566000007546. PMID 6540028.
- ↑ Paterson-Brown, S. (2007). "15. The acute abdomen and intestinal obstruction". In Parks, Rowan W.; Garden, O. James; Carter, David John; Bradbury, Andrew W.; Forsythe, John L. R. (eds.). Principles and practice of surgery (5th ed.). Edinburgh: Churchill Livingstone. ISBN 978-0-443-10157-1.
- ↑ Clegg-Lamptey JN, Armah H, Naaeder SB, Adu-Aryee NA (December 2006). "Position and susceptibility to inflammation of vermiform appendix in Accra, Ghana". East African Medical Journal. 83 (12): 670–3. doi:10.4314/eamj.v83i12.9498. PMID 17685212.
- ↑ Bakheit MA, Warille AA (June 1999). "Anomalies of the vermiform appendix and prevalence of acute appendicitis in Khartoum". East African Medical Journal. 76 (6): 338–40. PMID 10750522.
- ↑ Ghorbani A, Forouzesh M, Kazemifar AM (2014). "Variation in Anatomical Position of Vermiform Appendix among Iranian Population: An Old Issue Which Has Not Lost Its Importance". Anatomy Research International. 2014: 313575. doi:10.1155/2014/313575. PMC 4176911. PMID 25295193.
- ↑ Denjalić A, Delić J, Delić-Custendil S, Muminagić S (2009). "[Variations in position and place of formation of appendix vermiformis found in the course of open appendectomy]". Medicinski Arhiv (in Bosnian). 63 (2): 100–1. PMID 19537667.
- ↑ Zetina-Mejía CA, Alvarez-Cosío JE, Quillo-Olvera J (2009). "Congenital absence of the cecal appendix. Case report". Cirugia y Cirujanos. 77 (5): 407–10. PMID 19944032.
- ↑ Kumar, Vinay; Robbins, Stanley L.; Cotran, Ramzi S. (1989). Robbins' pathologic basis of disease (4th ed.). Philadelphia: Saunders. pp. 902–3. ISBN 978-0-7216-2302-3.
- 1 2 "Scientists may have found appendix's purpose". NBC News. Associated Press. 5 October 2007. Archived from the original on 4 February 2020. Retrieved 24 August 2019.
- 1 2 Randal Bollinger R, Barbas AS, Bush EL, Lin SS, Parker W (December 2007). "Biofilms in the large bowel suggest an apparent function of the human vermiform appendix". Journal of Theoretical Biology. 249 (4): 826–31. Bibcode:2007JThBi.249..826R. doi:10.1016/j.jtbi.2007.08.032. PMID 17936308.
- ↑ Sonnenburg JL, Angenent LT, Gordon JI (June 2004). "Getting a grip on things: how do communities of bacterial symbionts become established in our intestine?". Nature Immunology. 5 (6): 569–73. doi:10.1038/ni1079. PMID 15164016. S2CID 25672527.
- ↑ Everett M.L.; Palestrant D.; Miller S.E.; Bollinger R.R.; Parker W. (2004). "Immune exclusion and immune inclusion: a new model of host-bacterial interactions in the gut". Clinical and Applied Immunology Reviews. 4 (5): 321–32. doi:10.1016/j.cair.2004.03.001.
- ↑ Dunn, Rob (January 2, 2012). "Your Appendix Could Save Your Life". Scientific American. Archived from the original on 11 November 2020. Retrieved 22 December 2016.
- ↑ Zahid A (April 2004). "The vermiform appendix: not a useless organ". Journal of the College of Physicians and Surgeons--Pakistan. 14 (4): 256–8. PMID 15228837.
- ↑ Rankin LC, Girard-Madoux MJ, Seillet C, Mielke LA, Kerdiles Y, Fenis A, et al. (February 2016). "Complementarity and redundancy of IL-22-producing innate lymphoid cells". Nature Immunology. 17 (2): 179–86. doi:10.1038/ni.3332. PMC 4720992. PMID 26595889.
- ↑ Smith H, Parker W, Kotze S, Laurin M (September 2016). "Morphological evolution of the mammalian cecum and cecal appendix" (PDF). Comptes Rendus Palevol. 16 (1): 39–57. doi:10.1016/j.crpv.2016.06.001.
- ↑ "Miscellaneous conditions of the appendix". Seminars in Diagnostic Pathology. National Institutes of Health. 21 (2): 151–63. 2004. doi:10.1053/j.semdp.2004.11.006. PMID 15807474. Retrieved 30 December 2020.
- ↑ "Statistics about Appendix disorder". rightdiagnosis.com. Archived from the original on 2019-10-16. Retrieved 2020-12-30.
- 1 2 3 Miller R., Kenneth; Levine, Joseph (2002). Biology. Prentice Hall. pp. 92–98. ISBN 978-0-13-050730-3.
- ↑ "Appendicitis - Symptoms and causes - Mayo Clinic". mayoclinic.org. Mayo Clinic. Archived from the original on 25 November 2020. Retrieved 29 December 2020.
- ↑ Wilms; de Hoog; de Visser (November 2011). "Appendectomy versus antibiotic treatment for acute appendicitis". Cochrane Database of Systematic Reviews (11): CD008359. doi:10.1002/14651858.CD008359.pub2. PMID 22071846.
- ↑ Mingin GC, Baskin LS (2003). "Surgical management of the neurogenic bladder and bowel". International Braz J Urol. 29 (1): 53–61. doi:10.1590/S1677-55382003000100012. PMID 15745470.
- ↑ "Wellington Children's Hospital : Caring for an ACE or Chait Tube : Healthpoint". Retrieved 22 December 2016.
- ↑ Darwin, Charles (1871) "Jim's Jesus". The Descent of Man, and Selection in Relation to Sex. John Murray: London.
- ↑ Smith HF, Fisher RE, Everett ML, Thomas AD, Bollinger RR, Parker W (October 2009). "Comparative anatomy and phylogenetic distribution of the mammalian cecal appendix". Journal of Evolutionary Biology. 22 (10): 1984–99. doi:10.1111/j.1420-9101.2009.01809.x. PMID 19678866. S2CID 6112969.
- ↑ Smith H. F.; Parker W.; Kotzé, S. H.; Laurin, M. (2013). "Multiple independent appearances of the cecal appendix in mammalian evolution and an investigation of related ecological and anatomical factors". Comptes Rendus Palevol. 12 (6): 339–354. doi:10.1016/j.crpv.2012.12.001.
- ↑ Smith H. F.; Parker W.; Kotzé, S. H.; Laurin, M. (2017). "Morphological evolution of the mammalian cecum and cecal appendix". Comptes Rendus Palevol. 11 (1): 39–57. doi:10.1016/j.crpv.2016.06.001.
- ↑ Laurin M, Everett ML, Parker W (April 2011). "The cecal appendix: one more immune component with a function disturbed by post-industrial culture". Anatomical Record. 294 (4): 567–79. doi:10.1002/ar.21357. PMID 21370495. S2CID 3237168.
- ↑ Evolution of the Appendix: A Biological 'Remnant' No More; By Duke Medicine News and Communications; Published: 20 August 2009 Updated: 21 August 2009
Further reading
| Wikimedia Commons has media related to Appendix (anatomy). |
- Appendix May Actually Have a Purpose—2007 WebMD article
- Anatomy photo:37:12-0102 at the SUNY Downstate Medical Center—"Abdominal Cavity: The Cecum and the Vermiform Appendix"
- "The vestigiality of the human vermiform appendix: A Modern Reappraisal"—evolutionary biology argument that the appendix is vestigial
- Smith HF, Fisher RE, Everett ML, Thomas AD, Bollinger RR, Parker W (October 2009). "Comparative anatomy and phylogenetic distribution of the mammalian cecal appendix". Journal of Evolutionary Biology. 22 (10): 1984–99. doi:10.1111/j.1420-9101.2009.01809.x. PMID 19678866. S2CID 6112969.
- Cho, Jinny. "Scientists refute Darwin's theory on appendix". The Chronicle (Duke University), August 27, 2009. (News article on the above journal article.)
Authority control | |
|---|---|
| National libraries | |
| Scientific databases | |