1,1,2,2-Tetrachloroethane
1,1,2,2-tetrachloroethane (TeCA), also known by the brand names Bonoform, Cellon and Westron, is an organic compound. It is colorless liquid and has a sweet odor. It is used as an industrial solvent and as a separation agent. TeCA is toxic and it can be inhaled, consumed or absorbed through the skin. After exposure, nausea, dizziness or even liver damage may occur.
 | |||
| |||
| Names | |||
|---|---|---|---|
| Preferred IUPAC name
1,1,2,2-Tetrachloroethane | |||
| Other names
s-Tetrachloroethane Acetylene tetrachloride R-130 TeCA UN 1702 | |||
| Identifiers | |||
3D model (JSmol) |
|||
| ChEBI | |||
| ChEMBL | |||
| ChemSpider | |||
| ECHA InfoCard | 100.001.089 | ||
| KEGG | |||
PubChem CID |
|||
| UNII | |||
CompTox Dashboard (EPA) |
|||
| |||
| |||
| Properties | |||
| C2H2Cl4 | |||
| Molar mass | 167.848 g/mol | ||
| Appearance | Colorless to pale yellow liquid[2] | ||
| Odor | pungent, chloroform-like[2] | ||
| Density | 1.59 g/cm3 | ||
| Melting point | −44 °C (−47 °F; 229 K) | ||
| Boiling point | 146.5 °C (295.7 °F; 419.6 K) | ||
| 1 g/350 mL | |||
| Vapor pressure | 5 mmHg (20°C)[2] | ||
| -89.8·10−6 cm3/mol | |||
| Hazards | |||
| Lethal dose or concentration (LD, LC): | |||
LC50 (median concentration) |
1000 ppm (rat, 4 hr)[3] | ||
LCLo (lowest published) |
1000 ppm (rat, 4 hr) 643 ppm (mouse, 2 hr) 2714 ppm (cat, 45 min)[3] | ||
| NIOSH (US health exposure limits): | |||
PEL (Permissible) |
TWA 5 ppm (35 mg/m3) [skin][2] | ||
REL (Recommended) |
Ca TWA 1 ppm (7 mg/m3) [skin][2] | ||
IDLH (Immediate danger) |
Ca [100 ppm][2] | ||
Except where otherwise noted, data are given for materials in their standard state (at 25 °C [77 °F], 100 kPa).
Infobox references | |||
History
1,1,2,2-Tetrachloroethane and 1,1,1,2-Tetrachloroethane were discovered by Auguste Laurent in 1836.[4][5]
1,1,2,2-tetrachloroethane was used in large amounts to produce other chemicals like trichloroethylene, tetrachloroethylene, and 1,2-dichloroethylene.[6] It also found its function as an industrial solvent and was used in paint removers and pesticides.
Because of its possible carcinogen effects on humans, the production of 1,1,2,2-tetrachloroethane has decreased significantly and is no longer widely used as an end-product.[7] It is however still generated as a byproduct and as an intermediate product during manufacturing, where low levels of the chemical have been detected in the air.[8]
Synthesis
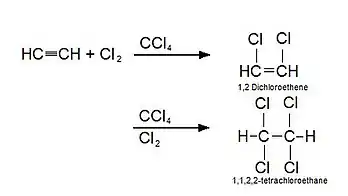
There are a few different ways to synthesise 1,1,2,2-tetrachloroethane. 1,1,2,2-tetrachloroethane can be produced by the catalytic addition of chlorine to acetylene (ethyne) which yields the highest purity.[9] It is also produced by direct chlorination or oxychlorination utilizing ethylene as feedstock and by catalytic chlorination of ethane or chlorination of 1,2- dichloroethane.[8] 1,1,2,2-Tetrachloroethane is always produced in closed systems to obtain the highest yield. Common side products that are created during the synthesis of 1,1,2,2-tetrachloroethane are 1,2-Dichloroethane and trichloroethylene (in the presence of heat).[10]
Toxicity
Alcohol increases the metabolism of 1,1,2,2-tetrachloroethane (TeCA)[11] and it will intensify the effects of TeCA.[12] Humans who consume alcohol might be at an increased risk for all toxic effects from TeCA. This is also a case for several other chlorinated aliphatic hydrocarbons. An investigation showed when you combine alcohol with TeCA it increases the relative weight of the experimented rats, indicating an enlarged activity of TeCA.[12]
Metabolism
The metabolism is believed to involve cytochrome (CYP) P450. Experiments showed that biotransformation reactions increased with chronic ethanol consumption and fasting.[13]
Mechanism of action
Looking at the chemical and physical properties the 1,1,2,2,-tetrachloroethane (TeCA) might be rapidly and extensively absorbed, which results in oral and inhalation exposures. In animal studies the oral take up was reported bij 70-100%[14][15] and 40-97% oral uptake in human inhalation.[16][17] TeCA is a small, volatile, lipophilic molecule; it appears that TeCA readily be absorbed from respiratory and gastrointestinal tracts. Absorption with passive diffusion is the most likely mechanism.
After TeCA is absorbed in the body, it is readily distributed throughout the body via passive diffusion. TeCA will most likely accumulate in lipid-rich tissues, liver.[14][15][18] Urinary elimination occurs as metabolites, including formic acid, glyoxalic acid, trichloroacetic acid and trichloroethanol.[14][15][18][19][20]
Already mentioned before passive diffusion is an important mechanism, because it is most likely the major mechanism of excretion.[14][15][18][19][20]
TeCA metabolism to reactive products plays a key role in the toxicity of TeCA. Microsomal and nuclear cytochrome P450 enzymes are implicated in the metabolism with TeCA, releasing biologically active compounds as; aldehydes, alkenes, acids and free radicals. Experiments of Hanley, Milman and Mitoma obtained evidence of this metabolism in rats.[14][15][21] Thus, metabolic capacity for tissues high, liver, formation of active metabolites is a likely mechanism for the toxicity. [PDF]
Mechanism for neurological effects is not yet determined and therefore can not be described, TeCA might play a role. The property of the readily passive diffusion to lipid-rich tissues allows it to interfere with neural membrane function, central nervous system depression, behavioral changes and anesthesia.[22] but there are no studies of TeCA's mechanism of neuronal effects.
Mode of action of the carcinogenic effect of TeCA is not completely determined. Several studies of TeCA have reported increases in the number of hepatocytes in mitosis, but the role these effects might have of TeCA on carcinogenicity is not evaluated. It suggests that TeCA may have promoting and initiating activity.[21][23][24]
Toxicokinetics
The most common health effect was found to be on the liver following 1,1,2,2-tetrachloroethane (TeCA) exposure. The studies for this have been divided into the four different Toxicokinetic phases: Adsorption, Distribution, Metabolism and Excretion (ADME). Three exposure routes have been studied to examine the effects depending on the entry route of TeCA into the body.
- Oral exposure: The experiment for the oral exposure was done by administering oral doses of radioactively labeled TeCA by gavage in corn oil to rats and mice. Followed by measuring the radioactivity in the expired air and urine.[14] a) Adsorption: With a measured radioactivity of 65%-73% the conclusion made was that the compound is almost completely absorbed orally. b) Distribution: Hepatic protein binding was observed by purifying the liver protein. Furthermore, adverse effects were seen in liver, kidney and testes leading to the conclusion that TeCA is distributed to these tissues.[25] c) Metabolism: see experiments on Metabolism routes d) Excretion: After 72h more than 90% of the dose was excreted in metabolized or unchanged form. The largest part was excreted in breath followed by urine and the least amount of TeCA was recovered in feces. 20%-30% were retained in skin and carcass.
- Inhalation exposure: The experiment on the health effects following inhalation exposure was performed on human volunteers[17] for adsorption and excretion studies and on animals[14] for distribution and metabolism. A bulb containing 38C1-labeled TeCA was inserted into their mouths and the volunteers inhaled deeply, held their breath for 20 seconds, and exhaled. The excretion of the radiolabeled TeCA was measured. a) Adsorption: The results of the study showed that 97% TeCA was adsorbed in a single breath. b) Distribution: After exposure to mice and rats via inhalation adverse effects were observed in liver and kidney indicating a systemic distribution of TeCA to these tissues. c) Metabolism: Following 6 hours of inhalation exposure the level of radioactively labeled TeCA was measured at a concentration of 7.73% non metabolized in expired air. 72 hours later 1.78% was measured. d) Excretion: One hour after exposure 3% of inhaled TeCA was measured in excreted breath and 0.015% in urine.
- Dermal exposure: To measure the health effects following dermal exposure were performed 1mL of TeCA was applied to the skin of mice and guinea pigs.[26] a) Adsorption: Within one half hour the dose was absorbed into the skin. b) Distribution: No experiments available. c) Metabolism: No experiments available d) Excretion: The half-life of TeCA in blood was shown to be approximately two hours.
Health effects
1,1,2,2-tetrachloroethane (TeCA) has a vast array of effects spread throughout the whole body. Effects have been investigated on different systems on both humans and animals, stated respectively.
Gastrointestinal Effects
4 studies[27][28][29][30] on humans after TeCA exposure determined gastrointestinal distress in the participants. Two humans exposed to 2.9 ppm TeCA for 30 minutes showed symptoms of vomiting and nausea.[16] These symptoms also caused weight loss.[31]
A study by Horiuchi et al.[32] showed that a monkey frequently exposed to 1.9 ppm TeCA got anorexic and developed regular diarrhea.
Hematological Effects
Workers in an artificial silk factory that had regularly inhaled TeCA, showed elevated white blood cell levels and slight anemia.[33]
In 1962, a study showed that 2⁄3 of the investigated rats exposed to 9000 ppm TeCA for 29 days had decreased red blood cells and hemoglobin levels.[32]
Hepatic Effects
Autopsies on humans who died due to TeCA exposure showed that some humans developed hepatic failure from the TeCA, they showed jaundice and an enlarged liver. The liver is the most affected system with TeCA poisoning, causing for example apoptosis of the liver tissue.[27][28][29][32][33]
After 60 ppm exposure rats show fatty liver degeneration.[34] Another study determined the limit for acute hepatic failure to be at 102ppm for four hours, indicated by increases in hepatic ascorbic acid and serum glutamate dehydrogenase and decreases in serum triglycerides.[12]
Ocular Effects
The vapors of TeCA can cause eye irritation, stinging, squinting and lacrimation in both humans[16] and animals.[35] This is due to direct contact of the skin and vapor rather than inhalation or digestion.
Neurological effects
Inhalation of TeCA vapor can cause dizziness, headache and tremors.[16]
Acute symptoms in rats showed in the form of 50% motor loss when exposed to 360ppm for one hour.[36]
Carcinogenic Effects
The National Cancer Institute performed experiments on the tumorigenicity of TeCA in rats and mice via the oral exposure route. Liver tumors were found in both species. Other studies on the tumorigenic mode of action revealed that it acts both as initiator and promoter.[25]
Lethal dose
Due to several case study reports on individuals who died after ingesting TeCA, the approximate lethal dose was possible to be established. Since the amount consumed varied this was difficult to exactly determine. One report was shown to be 4100 mg/kg,[37] the second 357 mg/kg[38] and the third 1100–9600 mg/kg.[39] Death following the ingestion occurred within 3–20 hours.
See also
References
- Merck Index, 11th Edition, 9125.
- NIOSH Pocket Guide to Chemical Hazards. "#0598". National Institute for Occupational Safety and Health (NIOSH).
- "1,1,2,2-Tetrachloroethane". Immediately Dangerous to Life or Health Concentrations (IDLH). National Institute for Occupational Safety and Health (NIOSH).
- Essai sur l'Action du Chlore sur la Liqueur des Hollandais et sur quelques Ethers in Annal. de Chimie, LXIII. (1836) page 377
- The so-called Perchloride of Formyl, Gmelin, L. (1855). Hand-book of Chemistry: Organic chemistry. Cavendish Society. pages 200–201
- "1,1,2,2-Tetrachloroethane" (PDF).
- "Toxicological Profile for 1,1,2,2-Tetrachloroethane" (PDF).
- "1,1,2,2-Tetrachloroethane".
- Antonini et al. Preparation of 1,2-dichloroethane and 1,1,2,2-tetrachloroethane by oxychlorination. United States Patent. 1975 May 13.
- OECD SIDS. 1,1,2,2-tetrachloroethane Initial Assessment Report. 2002 October 22–25.
- Sato A, Nakajima T, Koyama Y. 1980. Effects of chronic ethanol consumption on hepatic metabolism of aromatic and chlorinated hydrocarbons in rats. Br J Ind Med 37:382-386
- Schmidt P, Binnevies S, Gohlke R, et al. 1972. [Subacute action of low concentration of chlorinated ethanes on rats with and without additional ethanol treatment. I. Biochemical and toxicometrical aspects, especially results in subacute and chronic toxicity studies with 1,1,2,2-tetrachloroethane.] Int Arch Arbeitsmed 30:283-298. (German)
- Johansson I, Ekstroem G, Scholte B, Puzycki D, Jörnvall H, Ingelman-Sundberg M. Ethanol-, fasting-, and aceton-inducible cytochromes P-450 in rat liver: regulation and characteristics of enzymes belonging to the IIB and IIE gene subfamilies. Biochemistry. 1988 Mar 1;27(6):1925-34
- Hanley TR, Quast JF, Schumann AM. 1988. The metabolism and hepatic macromolecular interactions of 1,1,2,2-tetrachloroethane (TCE) in mice and rats. Dow Chemical Company. Submitted to the U.S. Environmental Protection Agency under TSCA Section 8D. OTS0514187.
- Milman HA, Mitoma C, Tyson C, et al. 1984. Comparative pharmacokinetics/metabolism, carcinogenicity and mutagenicity of chlorinated ethanes and ethylenes (meeting abstract). Arbete och Halsa 29:19.
- Lehmann KB, Schmidt-Kehl L. 1936. [Study of the 13 most important chlorohydrocarbons from the standpoint of industrial hygienics.] Arch Hyg 116:132-200. (German)
- Morgan A, Black A, Belcher DR. 1970. The excretion in breath of some aliphatic halogenated hydrocarbons following administration by inhalation. Ann Occup Hyg 13:219.
- Yllner S. 1971. Metabolism of 1,1,2,2-tetrachloroethane-14C in the mouse. Acta Pharmacol Toxicol 29:499-512.
- Gargas ML, Andersen ME. 1989. Determining kinetic constants of chlorinated ethane metabolism in the rat from rates of exhalation. Toxicol Appl Pharmacol 99:344-353.
- Ikeda M, Ohtsuji H. 1972. Comparative study of the excretion of Fujiwara reaction-positive substances in urine of humans and rodents given trichloro-or tetrachloro-derivatives of ethane and ethylene. Br J Ind Med 29:99-184.
- Milman HA, Story DL, Riccio ES, et al. 1988. Rat liver foci and in vitro assays to detect initiating and promoting effects of chlorinated ethanes and ethylenes. Ann NY Acad Sci 534:521-530.
- Klaassen, CD. 1996. Casarett & Doull's toxicology: The basic science of poisons. 5th ed. New York, NY: McGraw-Hill, 750-751.
- Colacci A, Vaccari M, Perocco P, et al. 1996. Enhancement of BALB/c 3T3 cells transformation by 1,2- dibromoethane promoting effect. Carcinogenesis 17(2):225-231.
- Story DL, Meierhenry EF, Tyson CA, et al. 1986. Difference in rat liver enzyme-altered foci produced by chlorinated aliphatics and phenobarbital. Toxicol Ind Health 2:351-362.
- National Cancer Institute (US). Division of Cancer Cause and Prevention. Bioassay of 1, 1, 2, 2-tetrachloroethane for Possible Carcinogenicity. Department of Health, Education, and Welfare, Public Health Service, National Institutes of Health, National Cancer Institute, Division of Cancer Cause and Prevention; 1978.
- Jakobson I, Wahlberg JE, Holmberg B, Johansson G. Uptake via the blood and elimination of 10 organic solvents following epicutaneous exposure of anesthetized guinea pigs. Toxicology and applied pharmacology. 1982 Apr 1;63(2):181-7.
- Coyer HA. 1944. Tetrachloroethane poisoning. Ind Med 13:230-233.
- Willcox WH, Spilsbury BH, Legge TM. 1915. An outbreak of toxic jaundice of a new type amongst aeroplane workers-Its clinical and toxicological aspect. Trans Med Soc London 38:129-156.
- Jeney E, Bartha F, Kondor L, et al. 1957. [Prevention of industrial tetrachloroethane intoxication--Part III.] Egeszsegtudomany 1:155-164. (Hungarian)
- Lobo-Mendonca R. 1963. Tetrachloroethane - A survey. Br J Ind Med 20:51-56.
- Parmenter DC. 1921. Tetrachloroethane poisoning and its prevention. J Ind Hyg 2:456-465.
- Horiuchi K, Horiguchi S, Hashimoto K, et al. 1962. Studies on the industrial tetrachloroethane poisoning. Osaka City Medical J 8:29-38.
- Koelsch F. 1915. Industrial poisonings by celluloid varnishes in the airplane industry. Muench Medizin Wochensch 62:1567-1569.
- Gohlke R, Schmidt P. 1972. [Subacute action of low concentrations of chlorinated ethanes with and without additional ethanol treatment in the rat.] Int Arch Arbeitsmed 30:299-312. (German)
- NIOSH. 1978. Toxicity data for establishing "immediately dangerous to life or health" (IDLH) values. Cincinnati, OH: National Institute for Occupational Safety and Health. PB87163531
- Horvath M, Frantik E. 1973. To the relative sensitivity of nervous functions and behavior to nonspecific effects of foreign substances. Activ Nerv Super 15:25-27.
- Hepple RA. An unusual case of poisoning. BMJ Military Health. 1927 Dec 1;49(6):442-5
- Lilliman B. Suggested mechanism of poisoning by liquid tetrachloroethane. Analyst. 1949 Jan 1;74(882):510-1.
- Mant AK. Acute Tetrachlorethane Poisoning. British Medical Journal. 1953 Mar 21;1(4811):655.