Nephritic syndrome
Nephritic syndrome is a syndrome comprising signs of nephritis, which is kidney disease involving inflammation. It often occurs in the glomerulus, where it is called glomerulonephritis. Glomerulonephritis is characterized by inflammation and thinning of the glomerular basement membrane and the occurrence of small pores in the podocytes of the glomerulus. These pores become large enough to permit both proteins and red blood cells to pass into the urine (yielding proteinuria and hematuria, respectively). By contrast, nephrotic syndrome is characterized by proteinuria and a constellation of other symptoms that specifically do not include hematuria.[6] Nephritic syndrome, like nephrotic syndrome, may involve low level of albumin in the blood due to the protein albumin moving from the blood to the urine.[7]
| Nephritic syndrome | |
|---|---|
| Other names | Acute nephritic syndrome[1] |
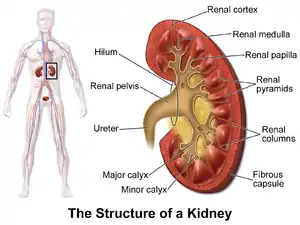 | |
| A graphic representation of the kidney. | |
| Specialty | Nephrology |
| Symptoms | Oliguria[2] |
| Causes | Infectious, autoimmune, or thrombotic[3] |
| Diagnostic method | Urinalysis, kidney biopsy[4] |
| Treatment | Antihypertensives[5] |
Signs and symptoms
Historically, nephritic syndrome has been characterized by blood in the urine (hematuria), high blood pressure (hypertension), decreased urine output <400 ml/day (oliguria), red blood cell casts, pyuria, and mild to moderate proteinuria.[8][9] If the condition is allowed to progress without treatment, it can eventually lead to azotemia and uremic symptoms.[9] This constellation of symptoms contrasts with the classical presentation of nephrotic syndrome (excessive proteinuria >3.5 g/day, low plasma albumin levels (hypoalbuminemia) <3 g/L, generalized edema, and hyperlipidemia).[8][10]
Signs and symptoms that are consistent with nephritic syndrome include:
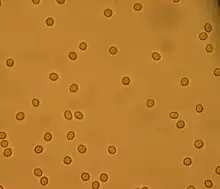
- Hematuria (red blood cells in the urine)[11]
- Proteinuria (protein in the urine) ranging from sub-nephrotic (<3.5 g/day) to >10 g/day,[7] although it is rarely above nephrotic range proteinuria levels.[12]
- Hypertension[13] resting blood pressure is persistently at or above 130/80 or 140/90 mmHg.[14]
- Blurred vision[4]
- Azotemia (increased plasma Urea and Creatinine)[2]
- Oliguria (low urine output <400 ml/day)[2]
- Red blood cell casts (seen with urinalysis and microscopy)[15]
- Pyuria (white blood cells or pus in the urine)[15]
Causes

Nephritic syndrome is caused by extensive inflammatory damage to the glomerulus capillaries, which is associated with a variety of medical conditions that we will discuss. Furthermore, the cause of this inflammation can be infectious, autoimmune, or thrombotic.[3] The causative conditions can be divided conveniently between age groups as follows, though it is important to note that many of the conditions listed in children/adolescents can also occur in adults with lower frequency, and vice versa:[4]
Children/adolescents
- IgA nephropathy (Note: Contrast time of onset with Post-streptococcal Glomerulonephritis) - Most commonly diagnosed in children who recently had an upper respiratory tract infection (URI). Symptoms typically present within 1–2 days of a non-specific URI with severe flank/abdominal pain, gross hematuria (characterized by dark brown or red colored urine), and edema of the hands, feet, and/or face.[16]
- Post-streptococcal glomerulonephritis (PSGN) - Similar to IgA nephropathy, post-streptococcal glomerulonephritis (PSGN) most often occurs in children who have recently had an upper respiratory infection (URI). In contrast with IgA nephropathy, however, PSGN typically presents 2–3 weeks after recovering from an URI that was caused specifically by a Streptococcus bacteria.[17] The symptoms at onset are very similar to IgA nephropathy and include abdominal pain, hematuria, edema, and oliguria.[18]
- Henoch–Schönlein purpura (HSP) - Often considered a systemic form of IgA nephropathy, Henoch–Schönlein purpura (HSP) is a systemic small-vessel vasculitis that is characterized by deposition of IgA antibody immune complexes in different key areas throughout the body. Most often, the condition presents in children with palpable purpura, abdominal pain, and arthritis. When the kidneys are affected, the IgA immune complexes deposit in the glomerulus very similarly to IgA nephropathy and will present in a similar way.[19]
- Hemolytic uremic syndrome - Most cases occur immediately following infectious diarrhea caused by a specific type of E. coli (O157:H7). The bacteria produces a toxin that causes widespread inflammation and numerous blood clots in small blood vessels (thrombotic microangiopathy). When the inflammation reaches the kidney, or the by-products of systemic inflammation build up in the kidney, the patient will begin showing signs of nephritic syndrome or potentially acute kidney failure (elevated creatinine, BUN, etc.).[20]
Adults
- Goodpasture syndrome - This is a rare autoimmune disease where autoantibodies are produced that target the glomerular basement membrane in both the lungs and the kidneys. The damage to the basement membrane causes bleeding, and the disease often presents in patients as hematuria and haemoptysis (coughing up blood). If not treated promptly with plasmapharesis to remove the autoantibodies, it can lead to permanent damage in the lungs/kidneys.[21]
- Systemic Lupus Erythematosus (SLE) - Better known as simply "Lupus", this autoimmune disease can affect nearly every major system in the human body and the kidneys are no exception. Autoantibodies produced in SLE can form immune complexes that deposit along the glomerular basement membrane and cause glomerular inflammation which leads to a nephritic syndrome.[22]
- Rapidly progressive glomerulonephritis - This is a syndrome of the kidney that is characterized by rapid loss of kidney function (usually >50% decline in glomerular filtration rate (GFR) within 3 months)[23] with glomerular crescent formation frequently seen on kidney biopsy. Without treatment, it will quickly lead to kidney failure and potentially death within months. This syndrome has numerous underlying causes that can also cause nephritic syndrome, so this may be more of an association than a cause.[24]
- Infective endocarditis - Infection that affects the inner lining of the heart (endocardium) and can potentially cause a thrombus to form on one or more heart valves and, if left untreated, can cause septic emboli that can have many systemic effects, including deposition into the glomerulus, causing glomerulonephritis and nephritic syndrome.[25]
- Cryoglobulinemia - Antibodies that are sensitive to the cold can become activated in cold conditions and cause an increase in blood viscosity (hyperviscosity syndrome) as well as forming immune complexes that can deposit in the small blood vessels and can cause nephritic syndrome when this occurs in the kidneys.[26]
- Membranoproliferative glomerulonephritis (MPGN) - Another type of glomerulonephritis that is caused primarily by immune complex deposition in the glomerular mesangium and glomerular basement membrane thickening, which activates the complement cascade and damages the glomerulus. This damage leads to inflammation in the glomerulus and can present with a nephritic syndrome.[27]
- Other ANCA small-vessel vasculitides - The conditions included in this category are eosinophilic granulomatosis with polyangiitis, microscopic polyangiitis, and granulomatosis with polyangiitis.[9]
Pathophysiology
The pathophysiology of nephritic syndrome is dependent on the underlying disease process, which can vary depending on what condition the nephritic syndrome is secondary to. More specifically, different diseases (many of which are mentioned above in the Causes section) affect different segments of the glomerulus and cause disease-specific segments of the glomerulus to become inflamed. Most often, it is dependent on what part of the glomerulus is damaged by antibody-antigen complex (immune complex) deposition.[9] In all cases, however, the inflammatory processes in the glomerulus cause the capillaries to swell and the pores between podocytes become large enough that inappropriate contents in the blood plasma (i.e. red blood cells, protein, etc.) will begin to spill into the urine. This causes a decrease in glomerular filtration rate (GFR) and, if left untreated over time, will eventually produce uremic symptoms and retention of sodium and water in the body, leading to both edema and hypertension.[9]
Diagnosis
The diagnostic approach to nephritic syndrome includes evaluating the patient for any suspected underlying pathology that could cause a nephritic syndrome.
Physical examination
If the person in the office is being examined by a physician, some physical exam findings consistent with nephritic syndrome include the following:
- Edema - This could present as generalized edema (anasarca) or specific swelling of the hands, feet, and/or face.[9]
- Other signs of fluid overload - Diffuse rales (crackles) may be heard at bilateral lung bases or diffusely in all lung fields on auscultation with a stethoscope. Jugular venous distention (JVD) may also be appreciated when visualizing the veins of the neck on physical exam.[9]
- Elevated blood pressure - Measured at least two separate times with at least two minutes between measurements using a sphygmomanometer or equivalent method.[28]
- Abnormal heart sounds - If the underlying cause is cardiac in nature (such as infective endocarditis), then you may appreciate abnormal heart sounds during auscultation of the heart.[29]
Laboratory testing
If the physician is suspicious of a possible nephritic syndrome, then he/she may order some common lab tests including:
- Serum electrolytes - The kidney is one of the main regulators of electrolytes in the human body and measuring the different electrolyte levels using either a basic metabolic panel (BMP) or comprehensive metabolic panel (CMP) can be a useful indicator of the underlying pathology.[30]
- Serum creatinine - Also measured using a BMP or CMP, creatinine is one of the most important indicators of current kidney function and is used to calculate the glomerular filtration rate (GFR). An elevated creatinine level is considered abnormal and may indicate decreased kidney function.[31]
- Blood urea nitrogen (BUN) - Also measured using a BMP or CMP, blood urea nitrogen is an indicator of how much nitrogen is in the blood at the time of the phlebotomy. The kidney is responsible for excreting nitrogenous substances in the urine, so an elevated BUN usually indicates that the kidney is not functioning appropriately.[32]
- Urine Analysis (Urinalysis) - After the patient provides a urine specimen, it is sent to the lab for analysis using a variety of methods including urine dipstick testing and microscopic examination. Because the kidney is responsible for making urine, analyzing the urine directly can provide crucial data that can help the physician diagnose nephritic syndrome.[33] Some findings on urinalysis that are consistent with nephritic syndrome include red blood cells (hematuria), red blood cell casts, proteinuria, and possibly white blood cells (pyuria).[9]
If nephritic syndrome is identified and diagnosed, then it is important for the physician to determine the underlying cause. To do this, he/she may order any of a large variety of relevant lab tests, some of which are included here:
- Blood culture - This is the process where a sample of the patient's blood is sent to the microbiology lab to attempt to isolate and grow any bacteria that may be circulating in the blood, in order to identify the pathogen.[34] This is helpful if the physician suspects infection as the underlying cause of the nephritic syndrome.
- Antinuclear antibody (ANA) titer - ANA is commonly positive in patients who have an underlying autoimmune disease, so this test is useful if the physician suspects an underlying autoimmune disease (refer to the Causes section above for examples) as the cause of the presenting nephritic syndrome. If positive, then the physician may order additional tests to determine which autoimmune condition is the cause and how best to treat it.[35]
- Antiglomerular basement membrane (anti-GBM) antibody - If positive, this is highly indicative of Goodpasture's syndrome and can be used to guide treatment.[9]
- Antineutrophil cytoplasmic antibody (ANCA) - If positive, this indicates that there is likely an underlying vasculitis that may be causing the acute nephritic syndrome.[36]
- Serum complement (C3 and C4) - Complement factors bind to antibodies to form immune complexes and a decreased serum complement level could indicate that the complement is being consumed at a higher rate due to the formation of immune complexes leading to deposition in the glomerulus of the kidney.[9]
Invasive testing
A kidney biopsy will provide a fully definitive diagnosis of nephritic syndrome and may also reveal the underlying cause of the nephritic syndrome depending on the underlying pathological process. On biopsy, a patient with nephritic syndrome would show inflammation of numerous glomeruli.[37]
Treatment
When a patient is confirmed to have nephritic syndrome, the main goal of treatment (regardless of the underlying cause) is to control elevated blood pressures and reduce active inflammation in the kidney itself.[4] Most often, the patient will need to be admitted to the hospital for close monitoring to ensure the efficacy of treatment and make adjustments as needed. Some treatment modalities commonly used to meet these goals include:
- Bed rest during the recovery process to ensure administration of optimal medical therapy with as low of a risk as possible for any exacerbating factors (falls, infection, etc.).[38]
- Fluid restriction to minimize the risk of edema (if not already present) or to reduce any active edema that may be present.[39]
- A special diet during the hospital stay that restricts sodium, potassium, and fluids in conjunction with the previously mentioned fluid restriction in an attempt to control symptoms of fluid overload.[40]
- Administration of diuretics if patient is showing signs of fluid overload. This will cause excess fluids to be excreted in the urine and may lessen the workload placed on the kidney, allowing it to recover from the inflammatory damage.[41]
- Administration of antihypertensives to alleviate hypertension and maintain a normal blood pressure during the recovery process.[42]
- Administration of anti-inflammatory medications (such as steroids or NSAIDs) to reduce active inflammation in the kidney.[43]
- If the patient is showing signs of kidney failure or end-organ damage, the treatment team may opt to utilize kidney dialysis temporarily (or permanently, in some severe cases) to decrease stress on the kidneys and allow for optimal recovery.[44]
Once the acute phase of the nephritic syndrome is controlled, it is crucial to determine the underlying pathology that caused the onset of the acute nephritic syndrome and to treat that condition. If the underlying cause is not determined and treated appropriately, it increases the risk of a recurrence of nephritic syndrome or chronic kidney disease (CKD) in the future.[4]
Prognosis
Because nephritic syndrome is a syndrome and not a disease, the prognosis depends on the underlying cause. Generally, the prognosis of nephritic syndrome in children is better than it is in adults.[5]
Epidemiology
According to the CDC, nephritis/nephrosis/nephritic syndrome was the 9th leading cause of death in the United States in 2017.[45] It was listed as the cause of death for 50,633 out of the total 2,813,503 deaths reported in 2017.[45]
Geography
The southeast region of the United States reported a significantly higher death rate due to kidney disease than any other region in 2017. Mississippi reported the highest death rate due to kidney disease (21.7), followed by Louisiana (20.6) and Arkansas (19.7).[46] Although Vermont reported the lowest death rate due to kidney disease (3.3), the western United States reported the lowest regional average death rate due to kidney disease in 2017.[46]
Gender
Out of the 1,374,392 female deaths reported in the US in 2017, kidney disease was listed as the cause of death for 24,889 women and was reported as the 9th overall cause of death for women in 2017.[45]
Out of the 1,439,111 male deaths reported in the US in 2017, kidney disease was not listed in the top 10 causes of death.[45]
Race and ethnicity
Out of the 2,378,385 deaths reported in individuals who identified as White, kidney disease was ranked 10th overall (39,105 deaths) in causes of death in the US in 2017.[45]
Out of the 340,644 deaths reported in individuals who identified as Black or African American, kidney disease was ranked 8th overall (9,609 deaths) in causes of death in the US in 2017.[45]
Out of the 74,094 deaths reported in individuals who identified as Asian or Pacific Islander, kidney disease was ranked 9th overall (1,563 deaths) in causes of death in the US in 2017.[45]
Out of the 197,249 deaths reported in individuals who identified as Hispanic or Latino, kidney disease was ranked 10th overall (3,928 deaths) in causes of death in the US 2017.[45]
References
- "acute nephritic syndrome" at Dorland's Medical Dictionary
- Madara, Bernadette; Pomarico-Denino, Vanessa (2008-07-08). Quick Look Nursing: Pathophysiology. Jones & Bartlett Learning. p. 484. ISBN 9780763749323.
- Schrier, Robert W. (2008-10-01). Manual of Nephrology. Lippincott Williams & Wilkins. pp. 144–145. ISBN 9780781796194.
- "Acute nephritic syndrome: MedlinePlus Medical Encyclopedia". www.nlm.nih.gov. Retrieved 2015-10-27.
- "Acute Nephritis; Nephrosis; Nephritic syndrome information. Patient | Patient". Patient. Retrieved 2015-10-27.
- Ferri, Fred F. (2017-05-25). Ferri's clinical advisor 2018 : 5 books in 1. Preceded by: Ferri, Fred F. Philadelphia, PA. p. 889. ISBN 978-0-323-52957-0. OCLC 989151714.
{{cite book}}: CS1 maint: location missing publisher (link) - Schrier, Robert W. (2010). Renal and Electrolyte Disorders. Lippincott Williams & Wilkins. pp. 559–560. ISBN 978-1-60831-072-2.
- Kibble, Jonathan David (2009). Medical physiology : the big picture. Halsey, Colby Ray. New York: McGraw-Hill. p. 221. ISBN 978-0-07-164302-3. OCLC 469141953.
- Harrison's principles of internal medicine. Longo, Dan L. (Dan Louis), 1949-, Fauci, Anthony S., 1940-, Kasper, Dennis L., Hauser, Stephen L., Jameson, J. Larry., Loscalzo, Joseph. (18th ed.). New York: McGraw-Hill. 2012. pp. 2334–2345. ISBN 978-0-07-174890-2. OCLC 747712285.
{{cite book}}: CS1 maint: others (link) - Floege, Jürgen; Johnson, Richard J.; Feehally, John (2010). Comprehensive Clinical Nephrology (Fourth ed.). Mosby. p. 198. doi:10.1016/B978-0-323-05876-6.00015-0. ISBN 9780323058766.
- Schrier, Robert W. (2010-01-01). Renal and Electrolyte Disorders. Lippincott Williams & Wilkins. p. 560. ISBN 9781608310722.
- Floege, Jurgen; Johnson, Richard J.; Feehally, John (2010-11-08). Comprehensive Clinical Nephrology E-Book. Elsevier Health Sciences. pp. 202–203. ISBN 978-0-323-08133-7.
- Krueger, Gerhard R. F.; Buja, L. Maximilian (2013-03-12). Atlas of Anatomic Pathology with Imaging: A Correlative Diagnostic Companion. Springer Science & Business Media. p. 287. ISBN 9781447128465.
- Whelton, Paul K.; Carey, Robert M.; Aronow, Wilbert S.; Casey, Donald E.; Collins, Karen J.; Dennison Himmelfarb, Cheryl; DePalma, Sondra M.; Gidding, Samuel; Jamerson, Kenneth A.; Jones, Daniel W.; MacLaughlin, Eric J. (June 2018). "2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines". Hypertension. 71 (6): e13–e115. doi:10.1161/HYP.0000000000000065. ISSN 1524-4563. PMID 29133356.
- "Subtopic 3: Microscopic Examination of Urine Sediment". Texas Collaborative. November 19, 2004. Archived from the original on 2004-11-19. Retrieved January 22, 2020.
- Davin, J. C.; Ten Berge, I. J.; Weening, J. J. (March 2001). "What is the difference between IgA nephropathy and Henoch–Schönlein purpura nephritis?". Kidney International. 59 (3): 823–834. doi:10.1046/j.1523-1755.2001.059003823.x. ISSN 0085-2538. PMID 11231337.
- "Acute Poststreptococcal Glomerulonephritis: Background, Pathophysiology, Epidemiology". 2018-12-05.
{{cite journal}}: Cite journal requires|journal=(help) - Comprehensive pediatric nephrology. Geary, Denis F., Schaefer, Franz. Philadelphia, PA: Mosby/Elsevier. 2008. pp. 309–317. ISBN 978-0-323-07096-6. OCLC 324995599.
{{cite book}}: CS1 maint: others (link) - Kraft, D. M.; Mckee, D.; Scott, C. (August 1998). "Henoch–Schönlein purpura: a review". American Family Physician. 58 (2): 405–408, 411. ISSN 0002-838X. PMID 9713395.
- Cody, Ellen M.; Dixon, Bradley P. (February 2019). "Hemolytic Uremic Syndrome". Pediatric Clinics of North America. 66 (1): 235–246. doi:10.1016/j.pcl.2018.09.011. ISSN 1557-8240. PMID 30454746. S2CID 53875876.
- Salama, A. D.; Levy, J. B.; Lightstone, L.; Pusey, C. D. (2001-09-15). "Goodpasture's disease". Lancet. 358 (9285): 917–920. doi:10.1016/S0140-6736(01)06077-9. ISSN 0140-6736. PMID 11567730. S2CID 40175400.
- Ward, M. M. (2000-11-13). "Changes in the incidence of end-stage renal disease due to lupus nephritis, 1982-1995". Archives of Internal Medicine. 160 (20): 3136–3140. doi:10.1001/archinte.160.20.3136. ISSN 0003-9926. PMID 11074743.
- Lohr, James W. (January 10, 2018). "Rapidly Progressive Glomerulonephritis". Medscape. Retrieved January 21, 2020.
- Bhowmik, Dipankar (January 2011). "Clinical Approach to Rapidly Progressive Renal Failure" (PDF). Journal of the Association of Physicians of India. 59: 38–44. PMID 21751663.
- Robbins basic pathology. Kumar, Vinay, 1944-, Robbins, Stanley L. (Stanley Leonard), 1915-2003. (8th ed.). Philadelphia, PA: Saunders/Elsevier. 2007. pp. 406–408. ISBN 978-1-4160-2973-1. OCLC 69672074.
{{cite book}}: CS1 maint: others (link) - Retamozo, Soledad; Brito-Zerón, Pilar; Bosch, Xavier; Stone, John H.; Ramos-Casals, Manuel (November 2013). "Cryoglobulinemic disease". Oncology (Williston Park, N.Y.). 27 (11): 1098–1105, 1110–1116. ISSN 0890-9091. PMID 24575538.
- Habib, R.; Gubler, M. C.; Loirat, C.; Mäiz, H. B.; Levy, M. (April 1975). "Dense deposit disease: a variant of membranoproliferative glomerulonephritis". Kidney International. 7 (4): 204–215. doi:10.1038/ki.1975.32. ISSN 0085-2538. PMID 1095806.
- "Tips for having your blood pressure taken". National Heart, Lung, and Blood Institute. July 2, 2014. Archived from the original on July 2, 2014.
- "Techniques: Heart Sounds & Murmurs". University of Washington Department of Medicine. Retrieved January 22, 2020.
- "Electrolytes". MedlinePlus. November 20, 2017. Retrieved January 22, 2020.
- "Creatinine Blood Test". MedlinePlus. July 15, 2017. Retrieved January 22, 2020.
- "BUN - blood test". MedlinePlus. April 29, 2019. Retrieved January 22, 2020.
- "Urinalysis". MedlinePlus. February 7, 2019. Retrieved January 22, 2020.
- Lee, Andrew; Mirrett, Stanley; Reller, L. Barth; Weinstein, Melvin P. (November 2007). "Detection of bloodstream infections in adults: how many blood cultures are needed?". Journal of Clinical Microbiology. 45 (11): 3546–3548. doi:10.1128/JCM.01555-07. ISSN 0095-1137. PMC 2168497. PMID 17881544.
- Kavanaugh, A.; Tomar, R.; Reveille, J.; Solomon, D. H.; Homburger, H. A. (January 2000). "Guidelines for clinical use of the antinuclear antibody test and tests for specific autoantibodies to nuclear antigens". Archives of Pathology & Laboratory Medicine. 124 (1): 71–81. doi:10.5858/2000-124-0071-GFCUOT. ISSN 0003-9985. PMID 10629135.
- Bradwell, A. R. (1999). Advanced atlas of autoantibody patterns. Mead, G. P., Stokes, R. P., Binding Site Limited. Birmingham: The Binding Site. ISBN 0-7044-8510-9. OCLC 41258931.
- "Acute nephritic syndrome". MedlinePlus. July 16, 2019. Retrieved January 22, 2020.
- Allen, C.; Glasziou, P.; Del Mar, C. (1999-10-09). "Bed rest: a potentially harmful treatment needing more careful evaluation". Lancet. 354 (9186): 1229–1233. doi:10.1016/s0140-6736(98)10063-6. ISSN 0140-6736. PMID 10520630. S2CID 12196831.
- "Fluid Restricted Diet". Intermountain Healthcare. 2016. Retrieved January 23, 2020.
- Mahtani, Kamal R.; Heneghan, Carl; Onakpoya, Igho; Tierney, Stephanie; Aronson, Jeffrey K.; Roberts, Nia; Hobbs, F. D. Richard; Nunan, David (December 1, 2018). "Reduced Salt Intake for Heart Failure: A Systematic Review". JAMA Internal Medicine. 178 (12): 1693–1700. doi:10.1001/jamainternmed.2018.4673. ISSN 2168-6114. PMC 6422065. PMID 30398532. S2CID 53241717.
- Ali, Syed Salman; Sharma, Pramod Kumar; Garg, Vipin Kumar; Singh, Avnesh Kumar; Mondal, Sambhu Charan (April 2012). "The target-specific transporter and current status of diuretics as antihypertensive". Fundamental & Clinical Pharmacology. 26 (2): 175–179. doi:10.1111/j.1472-8206.2011.01012.x. ISSN 1472-8206. PMID 22145583. S2CID 43171023.
- Wright, Jackson T.; Bakris, George; Greene, Tom; Agodoa, Larry Y.; Appel, Lawrence J.; Charleston, Jeanne; Cheek, DeAnna; Douglas-Baltimore, Janice G.; Gassman, Jennifer; Glassock, Richard; Hebert, Lee (2002-11-20). "Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: results from the AASK trial". JAMA. 288 (19): 2421–2431. doi:10.1001/jama.288.19.2421. ISSN 0098-7484. PMID 12435255.
- Rhen, Turk; Cidlowski, John A. (2005-10-20). "Antiinflammatory action of glucocorticoids--new mechanisms for old drugs". The New England Journal of Medicine. 353 (16): 1711–1723. doi:10.1056/NEJMra050541. ISSN 1533-4406. PMID 16236742. S2CID 5744727.
- Tattersall, James; Dekker, Friedo; Heimbürger, Olof; Jager, Kitty J.; Lameire, Norbert; Lindley, Elizabeth; Van Biesen, Wim; Vanholder, Raymond; Zoccali, Carmine; ERBP Advisory Board (July 2011). "When to start dialysis: updated guidance following publication of the Initiating Dialysis Early and Late (IDEAL) study". Nephrology, Dialysis, Transplantation. 26 (7): 2082–2086. doi:10.1093/ndt/gfr168. ISSN 1460-2385. PMID 21551086.
- "Leading causes of death and numbers of deaths, by sex, race, and Hispanic origin: United States, 1980 and 2017" (PDF). CDC. 2018. Retrieved January 21, 2020.
- "Kidney Disease Mortality by State". CDC. 2017. Retrieved January 21, 2020.
- Covic, Adrian; Schiller, Adalbert; Volovat, Carmen; Gluhovschi, Gheorghe; Gusbeth-Tatomir, Paul; Petrica, Ligia; Caruntu, Irina-Draga; Bozdog, Gheorghe; Velciov, Silvia; Trandafirescu, Virginia; Bob, Flaviu; Gluhovschi, Cristina (1 February 2006). "Epidemiology of renal disease in Romania: a 10 year review of two regional renal biopsy databases". Nephrology Dialysis Transplantation. 21 (2): 419–424. doi:10.1093/ndt/gfi207. ISSN 0931-0509. PMID 16249204. Retrieved 1 May 2020.
Further reading
- Crutchlow, Eileen M.; Dudac, Pamela J.; MacAvoy, Suzanne; Madara, Bernadette R. (2002-01-01). Pathophysiology. Jones & Bartlett Learning. ISBN 9781556425653.
- Schrier, Robert W. (2014-05-13). Manual of Nephrology. Lippincott Williams & Wilkins. ISBN 9781469887364.