Chiari malformation
Chiari malformation (CM) is a structural defect in the cerebellum, characterized by a downward displacement of one or both cerebellar tonsils through the foramen magnum (the opening at the base of the skull). CMs can cause headaches, difficulty swallowing, vomiting, dizziness, neck pain, unsteady gait, poor hand coordination, numbness and tingling of the hands and feet, and speech problems.[5] Less often, people may experience ringing or buzzing in the ears, weakness, slow heart rhythm, or fast heart rhythm, curvature of the spine (scoliosis) related to spinal cord impairment, abnormal breathing, such as central sleep apnea, characterized by periods of breathing cessation during sleep, and, in severe cases, paralysis.[5]
| Chiari malformation | |
|---|---|
| Other names | Hindbrain herniation |
 | |
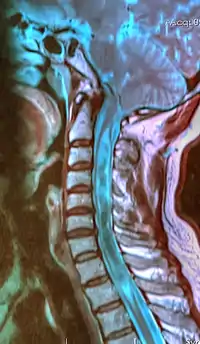
| A sagittal FLAIR MRI scan, from a patient with an Arnold–Chiari malformation, demonstrating tonsillar herniation of 7 mm. | |
| Pronunciation |
|
| Specialty | Neurosurgery |
| Complications | Hydrocephalus, spina bifida, syringomyelia, tethered cord syndrome.[1] |
| Types | I, II, III, IV[2] |
| Treatment | Decompressive surgery[3] |
| Prognosis | varies by type-see below |
| Frequency | 1 in 100 (type I)[lower-alpha 1] |
| Named after | |
This can sometimes lead to non-communicating hydrocephalus[6] as a result of obstruction of cerebrospinal fluid (CSF) outflow.[7] The cerebrospinal fluid outflow is caused by phase difference in outflow and influx of blood in the vasculature of the brain. The malformation is named after the Austrian pathologist Hans Chiari. A type II CM is also known as an Arnold–Chiari malformation in honor of Chiari and German pathologist Julius Arnold.
Signs and symptoms
Findings are due to brain stem and lower cranial nerve dysfunction. Onset of symptoms are less likely to be present during adulthood in most patients. Younger children generally have a substantially different presentation of clinical symptoms from older children. Younger children are more likely to have a more rapid neurological degeneration with profound brain stem dysfunction over several days.
- Neurogenic dysphagia: Difficulty swallowing. Seen by poor feeding in patient.
- Cyanosis: Bluish discoloration of skin while feeding.
- Weak crying
- Facial weakness
- Aspiration
- Headaches aggravated by Valsalva maneuvers, such as yawning, laughing, crying, coughing, sneezing or straining, bending over, or getting up suddenly[8]
- Tinnitus (ringing in the ears)
- Lhermitte's sign (electrical sensation that runs down the back and into the limbs)
- Vertigo (dizziness)
- Nausea
- Schmahmann syndrome
- Nystagmus (irregular eye movements; typically, so-called "downbeat nystagmus")
- Facial pain
- Muscle weakness
- Impaired gag reflex
- Dysphagia (difficulty swallowing)[9]
- Restless leg syndrome
- Sleep apnea
- Sleep disorders[10][11]
- Impaired coordination
- Severe cases may develop all the symptoms and signs of a bulbar palsy
- Paralysis due to pressure at the cervico-medullary junction may progress in a so-called "clockwise" fashion, affecting the right arm, then the right leg, then the left leg, and finally the left arm; or the opposite way around.[12]
- Papilledema on fundoscopic exam due to Increased intracranial pressure
- Pupillary dilation
- Dysautonomia: tachycardia (rapid heart), syncope (fainting), polydipsia (extreme thirst), chronic fatigue[13]
- Apnea: Sudden pause of breathing, usually during sleep.
- Opisthotonos: Spasm of the head which causes head to arch backwards. More common in infants than adults.
- Stridor
The blockage of cerebrospinal fluid (CSF) flow may also cause a syrinx to form, eventually leading to syringomyelia. Central cord symptoms such as hand weakness, dissociated sensory loss, and, in severe cases, paralysis may occur.[14]
Syringomyelia
Syringomyelia is most often chronic progressive degenerative disorder characterized by a fluid-filled cyst located in the spinal cord. However, there can be also cases where the syrinx in terms of size and extent of symptoms actually stays stable throughout a lifetime. Syringomyelia symptoms include pain, weakness, numbness, and stiffness in the back, shoulders, arms or legs. Other symptoms include headaches, the inability to feel changes in the temperature, sweating, sexual dysfunction, and loss of bowel and bladder control. It is usually seen in the cervical region but can extend into the medulla oblongata and pons or it can reach downward into the thoracic or lumbar segments. Syringomyelia is often associated with type I Chiari malformation and is commonly seen between the C-4 and C-6 levels. The exact development of syringomyelia is unknown but many theories suggest that the herniated tonsils in type I Chiari malformations cause a "plug" to form, which does not allow an outlet of CSF from the brain to the spinal canal. Syringomyelia is present in 25% of patients with type I Chiari malformations.[15]
Pathophysiology

The most widely accepted pathophysiological mechanism by which Chiari type I malformations occur is by a reduction or lack of development of the posterior fossa as a result of congenital or acquired disorders. Congenital causes include hydrocephalus, craniosynostosis (especially of the lambdoid suture), hyperostosis (such as craniometaphyseal dysplasia, osteopetrosis, erythroid hyperplasia), X-linked vitamin D-resistant rickets, and neurofibromatosis type I. Acquired disorders include space occupying lesions due to one of several potential causes ranging from brain tumors to hematomas.[16] Traumatic brain injury may cause delayed acquired Chiari malformation, but the pathophysiology of this is unknown.[17] Additionally, ectopia may be present but asymptomatic until a whiplash injury causes it to become symptomatic.[18]
Some neurological experts believe that Chiari malformation type I is developed as a result of Filum Disease, an abnormal traction of the spinal cord caused by an excessively tense Filum terminale. This theory was first introduced by Dr. Miguel B. Royo Salvador in 1993.[19]
Diagnosis
Diagnosis is made through a combination of patient history, neurological examination, and medical imaging.[20][21] Magnetic resonance imaging (MRI) is considered the preferred imaging modality for Chiari malformation.[22] The MRI visualizes neural tissue such as the cerebellar tonsils and spinal cord as well as bone and other soft tissues. CT and CT myelography are other options and were used prior to the advent of MRI, unfortunately the resolution of CT based modalities do not characterize syringomyelia and other neural abnormalities as well.[23]
By convention, the cerebellar tonsil position is measured relative to the basion-opisthion line, using sagittal T1 MRI images or sagittal CT images.[24] The selected cutoff distance for abnormal tonsil position is somewhat arbitrary, as not every person will be symptomatic at a certain amount of tonsil displacement, and the probability of symptoms and syrinx increases with greater displacement; however, greater than 5 mm is the most frequently cited cutoff number, though some consider 3–5 mm to be "borderline"; pathological signs and syrinx may occur beyond that distance.[24][25][26] One study showed little difference in cerebellar tonsil position between standard recumbent MRI and upright MRI for patients without a history of whiplash injury.[18] Neuroradiological investigation is used to first rule out any intracranial condition that could be responsible for tonsillar herniation. Neuroradiological diagnostics evaluate the severity of crowding of the neural structures within the posterior cranial fossa and their pressure against the foramen magnum. Chiari 1.5 is a term used when both brainstem and tonsillar herniation through the foramen magnum are present.[27]
The diagnosis of a Chiari II malformation can be made prenatally, through ultrasound.[28]
Classification
In the late 19th century, Austrian pathologist Hans Chiari described seemingly related anomalies of the hindbrain, the so-called Chiari malformations I, II and III. Later, other investigators added a fourth (Chiari IV) malformation. The scale of severity is rated I – IV, with IV being the most severe. Types III and IV are very rare.[29] Since Dr. Chiari's original descriptions Chiari 0, 1.5, 3.5, and 5 have been described in the medical literature.[30][27][31][32]
Types of Chiari malformation
| Type | Presentation | Clinical Features |
|---|---|---|
| 0 | Syringohydromyelia in the absence of cerebellar tonsillar herniation.[30][33][34] | Back pain, leg pain, hand numbness/weakness |
| I |
Herniation of cerebellar tonsils.[2][35][36] Tonsillar ectopia below the foramen magnum, with greater than 5 mm below as the most commonly cited cutoff value for abnormal position (although this is considered somewhat controversial).[24][25][37][38] Syringomyelia of cervical or cervicothoracic spinal cord can be seen. Sometimes the medullary kink and brainstem elongation can be seen. Can be congenital, or acquired through trauma. When congenital, may be asymptomatic during childhood, but often manifests with headaches and cerebellar symptoms. Syndrome of occipitoatlantoaxial hypermobility is an acquired Chiari I malformation in patients with hereditary disorders of connective tissue.[39] Patients who exhibit extreme joint hypermobility and connective tissue weakness as a result of Ehlers–Danlos syndrome or Marfan syndrome are susceptible to instabilities of the craniocervical junction; thus they are at risk for acquiring a Chiari malformation. |
Headache, neck pain, unsteady gait usually during childhood[2] |
| 1.5 | In addition to tonsillar ectopia, patients with this entity also have caudal descent of the brainstem. A significant proportion of these patients require a second surgery as a result of persistent syringomyelia.[27][33] | Headache and neck pain, similar to Chiari I |
| II | This is the only type also known as an "Arnold–Chiari" malformation. As opposed to the less-pronounced tonsillar herniation seen with Chiari I, there is a larger cerebellar vermian displacement. Low-lying torcular herophili (confluence of sinuses), tectal beaking, and hydrocephalus with consequent clival hypoplasia are classic anatomic associations.[40] Usually accompanied by a lumbar or lumbosacral myelomeningocele, with tonsillar herniation below the foramen magnum.[2][41] Colpocephaly may be seen due to the associated neural tube defect. | Paralysis below the spinal bifida defect[2] |
| III | Associated with an occipital encephalocele containing a variety of abnormal neuroectodermal tissues as well as possible herniation of elements of cerebellum, brainstem, and occipital lobe. Syringomyelia, tethered cord, and hydrocephalus may also be seen.[2][42] | Abundant neurological deficits[2] |
| 3.5 | In 1894, Giuseppe Muscatello described what is believed to be the only case of an occipitocervical encephalocele with a communication to the stomach. This is an interesting historic finding; however, has not been seen nor described since then.[31] | Not compatible with life. |
| IV | Characterized by a lack of cerebellar development, in which the cerebellum and brain stem lie within the posterior fossa with no relation to the foramen magnum.[2][43] Equivalent to primary cerebellar agenesis.[44] | Not compatible with life[2] |
| V | Characterized by absence of cerebellar development and occipital lobe ectopia into the foramen magnum.[32] This rare entity has two described cases in the medical literature, both associated with myelomeningocele. This has sparked controversy, given the proposed mechanism of this syndrome. Experts in neurosurgery disagree if this is truly a separate entity or just a part of the spectrum of Chiari 2 malformations.[45] |
Other conditions sometimes causally associated with Chiari malformation include hydrocephalus,[46] syringomyelia, spinal curvature, tethered spinal cord syndrome, and connective tissue disorders[39] such as Ehlers–Danlos syndrome[47] and Marfan syndrome.
Chiari malformation is the most frequently used term for this set of conditions. The use of the term "Arnold–Chiari malformation" has fallen somewhat out of favor over time, although it is used to refer to the type II malformation. Current sources use "Chiari malformation" to describe its four specific types, reserving the term "Arnold–Chiari" for type II only.[48] Some sources still use "Arnold–Chiari" for all four types.[49]
Chiari malformation or Arnold–Chiari malformation should not be confused with Budd–Chiari syndrome,[50] a hepatic condition also named for Hans Chiari.
In Pseudo-Chiari Malformation, leaking of CSF may cause displacement of the cerebellar tonsils and similar symptoms sufficient to be mistaken for a Chiari I malformation.[51]
Treatment
While there is no current cure, the treatments for Chiari malformation are surgery and management of symptoms, based on the occurrence of clinical symptoms rather than the radiological findings. The presence of a syrinx is known to give specific signs and symptoms that vary from dysesthetic sensations to algo-thermal dissociation to spasticity and paresis. These are important indications that decompressive surgery is needed for patients with Chiari Malformation Type II. Type II patients have severe brain stem damage and rapidly diminishing neurological response.[52][53]
Decompressive surgery[3] involves removing the lamina of the first and sometimes the second or third cervical vertebrae and part of the occipital bone of the skull to relieve pressure. The flow of spinal fluid may be augmented by a shunt. Since this surgery usually involves the opening of the dura mater and the expansion of the space beneath, a dural graft is usually applied to cover the expanded posterior fossa.
A small number of neurological surgeons believe that detethering the spinal cord as an alternate approach relieves the compression of the brain against the skull opening (foramen magnum), obviating the need for decompression surgery and associated trauma. However, this approach is significantly less documented in the medical literature, with reports on only a handful of patients. The alternative spinal surgery is also not without risk.
Complications of decompression surgery can arise. They include bleeding, damage to structures in the brain and spinal canal, meningitis, CSF fistulas, occipito-cervical instability and pseudomeningocele. Rare post-operative complications include hydrocephalus and brain stem compression by retroflexion of odontoid. Also, an extended CVD created by a wide opening and big duroplasty can cause a cerebellar "slump". This complication needs to be corrected by cranioplasty.[52]
In certain cases, irreducible compression of the brainstem occurs from in front (anteriorly or ventral) resulting in a smaller posterior fossa and associated Chiari malformation. In these cases, an anterior decompression is required. The most commonly used approach is to operate through the mouth (transoral) to remove the bone compressing the brainstem, typically the odontoid. This results in decompressing the brainstem and therefore gives more room for the cerebellum, thus decompressing the Chiari malformation. Arnold Menzes, MD, is the neurosurgeon who pioneered this approach in the 1970s at the University of Iowa. Between 1984 and 2008 (the MR imaging era), 298 patients with irreducible ventral compression of the brainstem and Chiari type 1 malformation underwent a transoral approach for ventral cervicomedullary decompression at the University of Iowa. The results have been excellent resulting in improved brainstem function and resolution of the Chiari malformation in the majority of patients.
Epidemiology
Congenital Chiari I malformation, defined as tonsilar herniations of 3 to 5 mm or greater, was previously believed to be in the range of one per 1000 births, but is likely much higher.[39][54] Women are three times more likely than men to have a congenital Chiari malformation.[55] Type II malformations are more prevalent in people of Celtic descent.[54] A study using upright MRI found cerebellar tonsillar ectopia in 23% of adults with headache from motor-vehicle-accident head trauma. Upright MRI was more than twice as sensitive as standard MRI, likely because gravity affects cerebellar position.[18]
Cases of congenital Chiari malformation may be explained by evolutionary and genetic factors. Typically, an infant's brain weighs around 400g at birth and triples to 1100-1400g by age 11. At the same time the cranium triples in volume from 500 cm3 to 1500 cm3 to accommodate the growing brain.[56] During human evolution, the skull underwent numerous changes to accommodate the growing brain. The evolutionary changes included increased size and shape of the skull, decreased basal angle and basicranial length. These modifications resulted in significant reduction of the size of the posterior fossa in modern humans. In normal adults, the posterior fossa comprises 27% of the total intracranial space, while in adults with Chiari Type I, it is only 21%.[57] H. neanderthalensis had platycephalic (flattened) skulls. Some cases of Chiari are associated with platybasia (flattening of the skull base).[58]
History
The history of Chiari malformation is described below and categorized by the year:
- 1883: Cleland was the first to describe Chiari II or Arnold–Chiari malformation on his report of a child with spina bifida, hydrocephalus, and anatomical alterations of the cerebellum and brainstem.[59]
- 1891: Hans Chiari, a Viennese pathologist, described the case of a 17-year-old female with elongation of the tonsils into cone shaped projections which accompany the medulla and are crammed into the spinal canal.[59]
- 1907: Schwalbe and Gredig, pupils of German pathologist Julius Arnold, described four cases of meningomyelocele and alterations in the brainstem and cerebellum, and gave the name "Arnold–Chiari" to these malformations.[59][60]
- 1932: Van Houweninge Graftdijk was the first to report the surgical treatment of Chiari malformations. All patients died from surgery or postoperative complications.[59]
- 1935: Russell and Donald suggested that decompression of the spinal cord at the foramen magnum might facilitate the CSF circulation.[59]
- 1940: Gustafson and Oldberg diagnosed Chiari malformation with syringomyelia.[59]
- 1974: Bloch et al. described the tonsils position to be classified between 7 mm and 8 mm below cerebellum.[59]
- 1985: Aboulezz used MRI for discovery of extension[59]
Society and culture
The condition was brought to the mainstream on the series CSI: Crime Scene Investigation in the tenth-season episode "Internal Combustion" on February 4, 2010.[61] Chiari malformation was briefly mentioned on the medical drama House M.D. in the fifth-season episode "House Divided", It was the focus of the sixth-season episode "The Choice". It is also the focus of Private Practice Season 4 episode 4, where a pregnant woman is diagnosed with it. It was the cause of death on the reality television series Dr. G: Medical Examiner in the sixth-season episode "Bruised and Battered". It was also mentioned in the medical drama A Gifted Man, in the first-season episode "In Case of Separation Anxiety".[62] It is also featured in the 3rd and 4th episode of the 7th season of the series Rizzoli & Isles where Dr. Maura Isles is diagnosed with the condition.[63][64][65]
Notable people
- Rosanne Cash[66] – U.S. singer-songwriter; daughter of Johnny Cash
- Julia Clukey[67] – U.S. luge competitor for Team USA in 2010 Vancouver Winter Olympics
- Joanna David[68] – British television and stage actress
- J. B. Holmes[69] – U.S. professional golfer
- Marissa Irwin[70] – U.S. fashion model with Chiari secondary to Ehlers–Danlos syndrome
- Bobby Jones[71] – U.S. World Golf Hall of Fame golfer and founder of the Augusta National Golf Club
- Allysa Seely – U.S. Gold Medalist at the 2016 Summer Paralympics in the paratriathlon[72]
- Leah Shapiro[73] – U.S. drummer for the band Black Rebel Motorcycle Club
- Michelle Stilwell – Canadian wheelchair racer and politician[74]
- Rachid Taha[75] – Algerian singer
- Sabre Norris – Australian skateboarder and surfer[76]
See also
Notes
- 1 in 1000 have symptomatic type I CM, but 1 in 100 meet the radiological criteria[4]
References
- clinic, mayo. "Chiari malformation". mayoclinic.org. Mayoclinic. Retrieved June 19, 2022.
- Vannemreddy P, Nourbakhsh A, Willis B, Guthikonda B (2010). "Congenital Chiari malformations". Neurology India. 58 (1): 6–14. doi:10.4103/0028-3886.60387. PMID 20228456.
- Guo F, Wang M, Long J, Wang H, Sun H, Yang B, Song L (2007). "Surgical management of Chiari malformation: analysis of 128 cases". Pediatric Neurosurgery. 43 (5): 375–81. doi:10.1159/000106386. PMID 17786002. S2CID 29634884.
- Sadler, Brooke; Kuensting, Timothy; Strahle, Jennifer; Park, Tae Sung; Smyth, Matthew; Limbrick, David D.; Dobbs, Matthew B.; Haller, Gabe; Gurnett, Christina A. (May 1, 2020). "Prevalence and Impact of Underlying Diagnosis and Comorbidities on Chiari 1 Malformation". Pediatric Neurology. 106: 32–37. doi:10.1016/j.pediatrneurol.2019.12.005. ISSN 0887-8994. PMC 7156318. PMID 32113729.
- "Chiari malformation: Symptoms". Mayo Clinic. November 13, 2008. Archived from the original on February 11, 2010.
- Hydrocephalus at eMedicine
- Rosenbaum, RB; DP Ciaverella (2004). Neurology in Clinical Practice. Butterworth Heinemann. pp. 2192–2193. ISBN 978-0-7506-7469-0.
- Riveira C, Pascual J (February 2007). "Is Chiari type I malformation a reason for chronic daily headache". Current Pain and Headache Reports. 11 (1): 53–5. doi:10.1007/s11916-007-0022-x. PMID 17214922. S2CID 41199446.
- "Department of Neurological Surgery – University of Washington". Depts.washington.edu. Archived from the original on November 21, 2010. Retrieved November 4, 2011.
- "Mystery of Sleepless Boy Solved". ABC News.
- "Medical Mystery: The Boy Who Couldn't Sleep". ABC News.
- "Chiari malformation". Mayo Clinic. Retrieved May 10, 2020.
- "Dysautonomia News – Winter/Spring 2006". Dinet.org. Archived from the original on November 29, 2011. Retrieved November 4, 2011.
- Chiari Malformation at eMedicine
- Adnan BURINA; Dževdet SMAJLOVIĆ; Osman SINANOVIĆ; Mirjana VIDOVIĆ; Omer Ć. IBRAHIMAGIĆ (2009). "ARNOLD–CHIARI MALFORMATION AND SYRINGOMYELIA". Acta Med Sal. 38: 44–46. doi:10.5457/ams.v38i1.31. Archived from the original on September 18, 2012.
- Loukas M, Shayota BJ, Oelhafen K, Miller JH, Chern JJ, Tubbs RS, Oakes WJ (September 2011). "Associated disorders of Chiari Type I malformations: a review". Neurosurgical Focus. 31 (3): E3. doi:10.3171/2011.6.FOCUS11112. PMID 21882908. S2CID 45262171.
- Moscote-Salazar LR, Zabaleta-Churio N, Alcala-Cerra G, M Rubiano A, Calderon-Miranda WG, Alvis-Miranda HR, Agrawal A (January 2016). "Symptomatic Chiari Malformation with Syringomyelia after Severe Traumatic Brain Injury: Case Report". Bulletin of Emergency and Trauma. 4 (1): 58–61. PMC 4779473. PMID 27162930.
- Freeman MD, Rosa S, Harshfield D, Smith F, Bennett R, Centeno CJ, Kornel E, Nystrom A, Heffez D, Kohles SS (2010). "A case-control study of cerebellar tonsillar ectopia (Chiari) and head/neck trauma (whiplash)". Brain Injury. 24 (7–8): 988–94. doi:10.3109/02699052.2010.490512. PMID 20545453. S2CID 9553904.
- "Malformación de Arnold Chiari | Institut Chiari de Barcelona".
- Ciaramitaro, Palma; Massimi, Luca; Bertuccio, Alessandro; Solari, Alessandra; Farinotti, Mariangela; Peretta, Paola; Saletti, Veronica; Chiapparini, Luisa; Barbanera, Andrea; Garbossa, Diego; Valentini, Laura (June 15, 2021). "Diagnosis and treatment of Chiari malformation and syringomyelia in adults: international consensus document". Neurological Sciences. 43 (2): 1327–1342. doi:10.1007/s10072-021-05347-3. ISSN 1590-3478. PMID 34129128. S2CID 235438643.
- "Chiari malformations". Institute for Neurology and Neurosurgery. Northwell Health. Retrieved March 28, 2023.
- McClugage, Samuel G.; Oakes, W. Jerry (September 2019). "The Chiari I malformation: JNSPG 75th Anniversary Invited Review Article". Journal of Neurosurgery: Pediatrics. 24 (3): 217–226. doi:10.3171/2019.5.PEDS18382. ISSN 1933-0707. PMID 31473667.
- "Chiari Malformations". The Lecturio Medical Concept Library. Retrieved July 5, 2021.
- Barkovich AJ, Wippold FJ, Sherman JL, Citrin CM (1986). "Significance of cerebellar tonsillar position on MR". AJNR. American Journal of Neuroradiology. 7 (5): 795–9. PMC 8331977. PMID 3096099.
- Aboulezz AO, Sartor K, Geyer CA, Gado MH (1985). "Position of cerebellar tonsils in the normal population and in patients with Chiari malformation: a quantitative approach with MR imaging". Journal of Computer Assisted Tomography. 9 (6): 1033–6. doi:10.1097/00004728-198511000-00005. PMID 4056132. S2CID 37901812.
- Chern JJ, Gordon AJ, Mortazavi MM, Tubbs RS, Oakes WJ (July 2011). "Pediatric Chiari malformation Type 0: a 12-year institutional experience". Journal of Neurosurgery. Pediatrics. 8 (1): 1–5. doi:10.3171/2011.4.peds10528. PMID 21721881. S2CID 2220301.
- Tubbs RS, Iskandar BJ, Bartolucci AA, Oakes WJ (November 2004). "A critical analysis of the Chiari 1.5 malformation". Journal of Neurosurgery. 101 (2 Suppl): 179–83. doi:10.3171/ped.2004.101.2.0179. PMID 15835105.
- Cui LG, Jiang L, Zhang HB, Liu B, Wang JR, Jia JW, Chen W (April 2011). "Monitoring of cerebrospinal fluid flow by intraoperative ultrasound in patients with Chiari I malformation". Clinical Neurology and Neurosurgery. 113 (3): 173–6. doi:10.1016/j.clineuro.2010.10.011. PMID 21075511. S2CID 22878869.
- "Arnold Chiari Malformation". Archived from the original on July 7, 2010. Retrieved July 17, 2008.
- Iskandar BJ, Hedlund GL, Grabb PA, Oakes WJ (August 1998). "The resolution of syringohydromyelia without hindbrain herniation after posterior fossa decompression". Journal of Neurosurgery. 89 (2): 212–6. doi:10.3171/jns.1998.89.2.0212. PMID 9688115.
- Fisahn C, Shoja MM, Turgut M, Oskouian RJ, Oakes WJ, Tubbs RS (December 2016). "The Chiari 3.5 malformation: a review of the only reported case". Child's Nervous System. 32 (12): 2317–2319. doi:10.1007/s00381-016-3255-3. PMID 27679454. S2CID 11329088.
- Tubbs RS, Muhleman M, Loukas M, Oakes WJ (February 2012). "A new form of herniation: the Chiari V malformation". Child's Nervous System. 28 (2): 305–7. doi:10.1007/s00381-011-1616-5. PMID 22038152. S2CID 3255189.
- Leland Albright, A.; Pollack, Ian F.; David Adelson, P. (September 15, 2014). Principles and practice of pediatric neurosurgery. Albright, A. Leland,, Pollack, Ian F.,, Adelson, P. David (Third ed.). New York. ISBN 9781604068016. OCLC 892430302.
{{cite book}}: CS1 maint: location missing publisher (link) - Tubbs RS, Elton S, Grabb P, Dockery SE, Bartolucci AA, Oakes WJ (May 2001). "Analysis of the posterior fossa in children with the Chiari 0 malformation". Neurosurgery. 48 (5): 1050–4, discussion 1054–5. doi:10.1097/00006123-200105000-00016. PMID 11334271. S2CID 12244111.
- Kojima A, Mayanagi K, Okui S (February 2009). "Progression of pre-existing Chiari type I malformation secondary to cerebellar hemorrhage: case report". Neurologia Medico-Chirurgica. 49 (2): 90–2. doi:10.2176/nmc.49.90. PMID 19246872.
- O'Shaughnessy BA, Bendok BR, Parkinson RJ, Shaibani A, Walker MT, Shakir E, Batjer HH (January 2006). "Acquired Chiari malformation Type I associated with a supratentorial arteriovenous malformation. Case report and review of the literature". Journal of Neurosurgery. 104 (1 Suppl): 28–32. doi:10.3171/ped.2006.104.1.28. PMID 16509477.
- Smith BW, Strahle J, Bapuraj JR, Muraszko KM, Garton HJ, Maher CO (September 2013). "Distribution of cerebellar tonsil position: implications for understanding Chiari malformation". Journal of Neurosurgery. 119 (3): 812–9. doi:10.3171/2013.5.jns121825. PMID 23767890.
- Raffel C (September 2013). "Cerebellar tonsil position and Chiari malformation". Journal of Neurosurgery. 119 (3): 810–1. doi:10.3171/2013.3.jns1339. PMID 23767894.
- Milhorat TH, Bolognese PA, Nishikawa M, McDonnell NB, Francomano CA (December 2007). "Syndrome of occipitoatlantoaxial hypermobility, cranial settling, and chiari malformation type I in patients with hereditary disorders of connective tissue". Journal of Neurosurgery. Spine. 7 (6): 601–9. doi:10.3171/SPI-07/12/601. PMID 18074684.
- "Cleveland Clinic Children's Hospital Pediatric Radiology Image Gallery". Cleveland Clinic. 2010. Archived from the original on June 27, 2010. Retrieved June 14, 2010.
- "Neuroradiology – Chiari malformation (I-IV)". Archived from the original on January 23, 2009.
- Arnold-Chiari+Malformation at the U.S. National Library of Medicine Medical Subject Headings (MeSH)
- "Chiari Malformations – Department of Neurological Surgery". Archived from the original on May 16, 2008.
- Yu F, Jiang QJ, Sun XY, Zhang RW (June 2015). "A new case of complete primary cerebellar agenesis: clinical and imaging findings in a living patient". Brain. 138 (Pt 6): e353. doi:10.1093/brain/awu239. PMC 4614135. PMID 25149410.
- Udayakumaran S (March 2012). "Chiari V or Chiari II plus?". Child's Nervous System. 28 (3): 337–8, author reply 339. doi:10.1007/s00381-011-1654-z. PMID 22159553. S2CID 26545840.
- "Neuropathology For Medical Students". Archived from the original on July 8, 2008.
- "Dr. Bland Discusses Chiari & EDS 4(10)". Conquerchiari.org. November 20, 2006. Archived from the original on June 25, 2013. Retrieved November 4, 2011.
- "Chiari malformation". Dorlands Medical Dictionary. Archived from the original on September 1, 2009.
- Kaipo T. Pau. "Chapter XVIII.16. Developmental Brain Anomalies". In Jeffrey K. Okamoto; et al. (eds.). Case Based Pediatrics For Medical Students and Residents. Archived from the original on May 28, 2010.
- "Code 453.0: Budd-Chiari Syndrome". 2008 ICD-9-CM Diagnosis. Archived from the original on December 5, 2008.
- "Spontaneous Spinal Cerebrospinal Fluid Leaks: Diagnosis". Archived from the original on December 11, 2011.
- Imperato A, Seneca V, Cioffi V, Colella G, Gangemi M (December 2011). "Treatment of Chiari malformation: who, when and how". Neurological Sciences. 32 (Suppl 3): S335-9. doi:10.1007/s10072-011-0709-y. PMID 21822700. S2CID 7602738. Archived from the original on May 15, 2022.
- Klekamp J, Batzdorf U, Samii M, Bothe HW (1996). "The surgical treatment of Chiari I malformation". Acta Neurochirurgica. 138 (7): 788–801. doi:10.1007/BF01411256. PMID 8869706. S2CID 6777364.
- "Chiari Malformation Fact Sheet | National Institute of Neurological Disorders and Stroke". Archived from the original on October 27, 2011. Retrieved January 9, 2015.
- "The Chiari Center - WI Chiari Center". Archived from the original on July 4, 2011. Retrieved December 28, 2012.
- Nolte J. The human brain: an introduction to its functional anatomy. Philadelphia: Mosby; 2002
- Furtado SV, Reddy K, Hegde AS (November 2009). "Posterior fossa morphometry in symptomatic pediatric and adult Chiari I malformation". Journal of Clinical Neuroscience. 16 (11): 1449–54. doi:10.1016/j.jocn.2009.04.005. PMID 19736012. S2CID 37527076.
- Sgouros S, Kountouri M, Natarajan K (September 2007). "Skull base growth in children with Chiari malformation Type I". Journal of Neurosurgery. 107 (3 Suppl): 188–92. doi:10.3171/PED-07/09/188. PMID 17918522.
- Schijman E (May 2004). "History, anatomic forms, and pathogenesis of Chiari I malformations". Child's Nervous System. 20 (5): 323–8. doi:10.1007/s00381-003-0878-y. PMID 14762679. S2CID 2735964.
- Enersen, Daniel. "Julius Arnold". Whonamedit A dictionary of medical eponyms. Archived from the original on February 4, 2015. Retrieved February 4, 2015.
- "CSI: Crime Scene Investigation–'Internal Combustion'". CSI Files. Retrieved March 28, 2023.
- "A Gifted Man - In Case of Separation Anxiety". CBS. Archived from the original on October 17, 2011.
- "Rizzoli & Isles 7x03 - Cops vs Zombies - Recap". June 15, 2016.
- @RizzoliIslesWB (June 14, 2016). "A Chiari Malformation?! That sounds really scary. *Googling now* #RizzoliandIsles" (Tweet) – via Twitter.
- Archived at Ghostarchive and the Wayback Machine: "Chiari Malformation". YouTube.
- "Rosanne Cash recovering from brain surgery – Entertainment – Celebrities". Today.com. October 26, 2011. Archived from the original on October 17, 2015. Retrieved November 4, 2011.
- Julia Clukey (January 21, 2014). "Olympian: Brain disorder made me stronger". CNN. Archived from the original on August 12, 2015. Retrieved August 26, 2015.
- Paton, Maureen (September 18, 2006). "We all make fantastic blunders…". The Daily Telegraph. Archived from the original on April 3, 2015. Retrieved March 13, 2015.
- ESPN.com news services (August 22, 2011). "J.B. Holmes to have brain surgery". espn.com. Archived from the original on July 8, 2017. Retrieved November 24, 2019.
- "Marissa's story" (PDF). Great Neck, NY, U.S.A.: The Chiari Institute and MedNet Technologies, Inc. Archived from the original (PDF) on September 6, 2015. Retrieved August 26, 2015.
- "Bobby Jones Society | Chiari & Syringomyelia Foundation". Csfinfo.org. Archived from the original on October 7, 2011. Retrieved November 4, 2011.
- "Paratriathlete Allysa Seely on prosthetics and PRs". ESPN. July 5, 2016. Archived from the original on August 4, 2017.
- David Renshaw (October 18, 2014). "Black Rebel Motorcycle Club cancel LA gig as drummer undergoes brain surgery". NME. Archived from the original on September 25, 2015. Retrieved August 26, 2015.
- Gary Kingston (May 31, 2008). "Lonely at the Top". The Vancouver Sun. Archived from the original on October 17, 2015. Retrieved August 27, 2015.
- mjid, Safia (September 14, 2018). "Mort à 59 ans, Rachid Taha souffrait d'une maladie génétique – H24info". H24info (in French). Retrieved September 22, 2018.
- Cronshaw, Damon (January 30, 2018). "Sabre Norris shares her story about her health and medical condition". Newcastle Herald. Archived from the original on August 28, 2021. Retrieved April 21, 2021.