Arytenoid adduction
Arytenoid adduction is a surgical procedure used to treat vocal cord paralysis. A suture is used to emulate the action of the lateral cricoarytenoid muscle and position the paralyzed vocal cord closer to the midline. This allows the two vocal cords to meet and can improve speaking and swallowing ability for affected patients. Arytenoid adduction is often performed in conjunction with medialization thyroplasty.
Vocal Cord Paralysis
One of the key functions of the larynx is phonation, the production of sound. Phonation requires the vocal cords to be adducted (positioned towards the midline) so that they can meet and vibrate together as air is expelled between them. Physiologically, the glottis is closed by intrinsic laryngeal muscles such as the lateral cricoarytenoid, thyroarytenoid, and interarytenoid muscles.[1] These muscles act on the arytenoid cartilages at the posterior ends of the vocal cords and are innervated by the left and right recurrent laryngeal nerves. Damage to these nerves results in vocal cord paralysis - the reduced mobility and inability to adduct one or both vocal cords. Many cases of vocal cord paralysis result from trauma during surgery.[2] Symptoms include hoarseness of voice, difficulty projecting, difficulty swallowing, and throat pain.
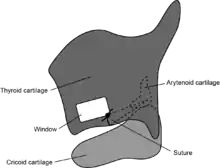
The arytenoid adduction procedure alleviates these symptoms by manually positioning the paralyzed vocal cord towards the midline. This is accomplished by passing a suture between the muscular process of the arytenoid cartilage and the thyroid cartilage.[3] This rotates the arytenoid cartilage and adducts the vocal cord.
Procedure
- Local anesthesia is preferred for arytenoid adduction so that the voice can be tested during the procedure.
- A horizontal skin incision is made at the inferior border of the thyroid cartilage.
- A window is cut in the thyroid cartilage for a suture to be passed through later in the procedure.
- The strap muscles, pharynx, and larynx are dissected to expose the muscular process of the arytenoid cartilage.
- A permanent suture is passed through the muscular process.
- A tunnel is made in the thyroid cartilage and one end of the suture is passed through it.
- The suture is tied and secured to the window made in the thyroid cartilage.
- The vocal cords are observed endoscopically to ensure proper rotation of the arytenoid.
- The patient is asked to phonate to evaluate voice quality and the potential need for a concurrent thyroplasty.
Indications
Options for surgical treatment of vocal cord paralysis include vocal cord injection, medialization thyroplasty, and arytenoid adduction.[4] Each of these techniques results in medialization of the paralyzed vocal cord. However, arytenoid adduction is preferred in cases where there is a large posterior glottal gap or vertical misalignment between the vocal folds. Arytenoid adduction is often performed at the same time as a medialization thyroplasty. Animal model studies suggest that combining the two procedures produces better outcomes than when performing either alone.[5]
Posterior glottal gap
The paralyzed vocal cord may rest close to or far from the midline. An extremely laterally positioned vocal cord can result in a large posterior glottal gap - an opening between the two vocal cords even when the functioning vocal cord is fully medialized. Vocal cord injection is ineffective for closing a large glottal gap.[6] Arytenoid adduction is more effective than medialization thyroplasty for closing a posterior gap. It has been suggested that this is because arytenoid adduction directly rotates the arytenoid cartilage and thus more actively medializes the posterior aspect of the vocal cord.[7]
Vertical glottal gap
The paralyzed vocal cord may rest on a different plane than the opposite vocal cord. This results in a vertical gap between the two vocal cords that cannot be resolved using vocal cord injection or medialization thryoplasty. The suture placed in the arytenoid adduction procedure mimics the action of the lateral cricoarytenoid muscle and pulls the vocal process of the arytenoid cartilage medially and inferiorly.[8] Thus arytenoid adduction can correct the vertical position of an elevated vocal cord.
Outcomes
Arytenoid adduction with or without medialization thyroplasty significantly improves quality of life for patients with vocal cord paralysis. Subjective outcome measures of voice quality include the Grade, Roughness, Breathiness, Asthenia, Strain (GBRAS) voice scale, Voice Handicap Index, and closure of the glottic gap. Objective outcome measures include mean and maximum phonation time, phonatory airflow, and signal-to-noise ratio.[9] Arytenoid adduction produces improvements in all of these parameters.[10][11][12][13]
Disadvantages and Complications
Arytenoid adduction is more technically challenging than either vocal cord injection or medialization thyroplasty and has a high learning curve.[12] Increased incidence of complications have been reported for arytenoid adduction compared to medialization thyroplasty.[14]
Potential complications include:
- Wound infection
- Edema
- Hematoma
- Vocal cord spasms
Intubation and/or tracheotomy may be required as a result of these complications.
References
- Haughey, Bruce; Lund, Valerie; Niparko, John; Robbins, K; Thomas, J; Lesperance, Marci (2014). Cummings Otolaryngology. Elsevier Saunders. ISBN 978-1455746965.
- Stager, SV (December 2014). "Vocal fold paresis: etiology, clinical diagnosis and clinical management". Current Opinion in Otolaryngology & Head and Neck Surgery. 22 (6): 444–9. doi:10.1097/MOO.0000000000000112. PMID 25254404. S2CID 23164908.
- Sulica, Lucian; Blitzer, Andrew (2006). Vocal fold paralysis. Berlin: Springer. ISBN 978-3540237655.
- Sulica, Lucian (8 May 2013). "Vocal Fold Paresis: An Evolving Clinical Concept". Current Otorhinolaryngology Reports. 1 (3): 158–162. doi:10.1007/s40136-013-0019-4.
- Green, DC; Berke, GS; Ward, PH (April 1991). "Vocal fold medialization by surgical augmentation versus arytenoid adduction in the in vivo canine model". The Annals of Otology, Rhinology, and Laryngology. 100 (4 Pt 1): 280–7. doi:10.1177/000348949110000404. PMID 2018285. S2CID 3898335.
- Choi, J; Son, YI; So, YK; Byun, H; Lee, EK; Yun, YS (March 2012). "Posterior glottic gap and age as factors predicting voice outcome of injection laryngoplasty in patients with unilateral vocal fold paralysis". The Journal of Laryngology and Otology. 126 (3): 260–6. doi:10.1017/S0022215111002702. PMID 22017979. S2CID 25859165.
- Thompson, DM; Maragos, NE; Edwards, BW (May 1995). "The study of vocal fold vibratory patterns in patients with unilateral vocal fold paralysis before and after type I thyroplasty with or without arytenoid adduction". The Laryngoscope. 105 (5 Pt 1): 481–6. doi:10.1288/00005537-199505000-00006. PMID 7760662.
- Miller, Frank R.; Bryant, Grady L.; Netterville, James L. (March 1999). "Arytenoid adduction in vocal fold paralysis". Operative Techniques in Otolaryngology–Head and Neck Surgery. 10 (1): 36–41. doi:10.1016/S1043-1810(99)80047-5.
- Siu, J; Tam, S; Fung, K (July 2016). "A comparison of outcomes in interventions for unilateral vocal fold paralysis: A systematic review". The Laryngoscope. 126 (7): 1616–24. doi:10.1002/lary.25739. PMID 26485674. S2CID 40706249.
- Isshiki, N; Tanabe, M; Sawada, M (October 1978). "Arytenoid adduction for unilateral vocal cord paralysis". Archives of Otolaryngology. 104 (10): 555–8. doi:10.1001/archotol.1978.00790100009002. PMID 697632.
- McCulloch, TM; Hoffman, HT; Andrews, BT; Karnell, MP (August 2000). "Arytenoid adduction combined with Gore-Tex medialization thyroplasty". The Laryngoscope. 110 (8): 1306–11. doi:10.1097/00005537-200008000-00015. PMID 10942131. S2CID 19858206.
- Chhetri, DK; Gerratt, BR; Kreiman, J; Berke, GS (December 1999). "Combined arytenoid adduction and laryngeal reinnervation in the treatment of vocal fold paralysis". The Laryngoscope. 109 (12): 1928–36. doi:10.1097/00005537-199912000-00006. PMID 10591349. S2CID 26857534.
- Kanazawa, T; Watanabe, Y; Komazawa, D; Indo, K; Misawa, K; Nagatomo, T; Shimada, M; Iino, Y; Ichimura, K (February 2014). "Phonological outcome of laryngeal framework surgery by different anesthesia protocols: a single-surgeon experience". Acta Oto-Laryngologica. 134 (2): 193–200. doi:10.3109/00016489.2013.847283. PMID 24215214. S2CID 11738878.
- Abraham, MT; Gonen, M; Kraus, DH (August 2001). "Complications of type I thyroplasty and arytenoid adduction". The Laryngoscope. 111 (8): 1322–9. doi:10.1097/00005537-200108000-00003. PMID 11568563. S2CID 23974212.