Beck–Fahrner syndrome
Beck–Fahrner syndrome, also known as BEFAHRS and TET3 deficiency, is a rare genetic disorder caused by mutations of the TET3 gene. It can occur de novo or can be inherited in an autosomal dominant manner. Mutations in the TET3 gene disrupts DNA demethylation (an epigenetic mechanism) during early embryogenesis and neural development. Most common clinical presentation includes global developmental delay, psychomotor retardation, neurodevelopmental disorders, hypotonia, epilepsy and dysmorphic features. It is diagnosed using molecular and genetic testing in setting of typical symptoms. Management is supportive and intended to improve quality of life.
| Beck–Fahrner syndrome | |
|---|---|
| Other names | BEFAHRS, TET3 deficiency |
 | |
| Specialty | Medical genetics, pediatrics |
| Symptoms | global developmental delay, psychomotor retardation, neurodevelopmental disorders, psychiatric disorders, hypotonia, epilepsy, dysmorphic features, strabismus, hearing loss, congenital heart defects |
| Usual onset | Present at birth |
| Duration | Lifelong |
| Types | de novo, autosomal dominant |
| Causes | Mutations of the TET3 gene |
| Diagnostic method | molecular diagnostics, genetic testing |
| Treatment | physical therapy, occupational therapy, educational therapy, speech therapy, assistive technology, anticonvulsant |
| Named after | David B. Beck, Jill A. Fahrner |
Signs and symptoms
Beck–Fahrner syndrome is also known as "BEFAHRS", which is a mnemonic for its most common features: behavioral differences, epilepsy, facial features, autistic features, hypotonia, retardation of psychomotor development, and size differences.[1]
Global developmental delay is the most common symptom with psychomotor retardation, speech delay, disrupted fine and gross motor skills.[2] Intellectual disability and learning disability are often present, sometimes concurrently.[3] Over two-thirds of affected individuals have autism spectrum disorder or social communication disorder.[4] Attention deficit hyperactivity disorder, obsessive–compulsive tendencies, anxiety, depression and psychosis have also been noted.[2][5]
Neurodevelopmental anomalies, motor and movement disorders such as hypotonia (most common), dystonia, spasticity, tic disorder, myoclonus, dysmetria and abnormal posturing have been observed with varying intensity and frequency.[2] Epilepsy affects over one-third individuals with Beck–Fahrner syndrome;[4] generalized tonic-clonic seizures,[1] complex partial seizures,[3] absence seizures, epileptic spasms[2] and electrical status epilepticus during slow-wave sleep have been seen.[6] Neuroimaging yields non-specific findings in some cases, such as ventriculomegaly, periventricular leukomalacia,[2] cerebellar hypoplasia and agenesis of the corpus callosum.[4]
Craniofacial abnormalities include myopathic facies, long face syndrome sometimes with wide forehead, brachycephaly, protruding ear, epicanthic folds, downslanted palpebral fissures, short nose with long philtrum, asymmetrical jaw, open-mouth appearance, high-arched palate, cleft lip and cleft palate. Musculoskeletal abnormalities such as kyphosis, scoliosis, joint hypermobility, hip dysplasia, pes planus and inguinal hernia have been reported. Individuals that exhibited overgrowth sometimes had macrocephaly and tall stature; one such case also had concurrent nephromegaly and cardiomegaly. Undergrowth, when present, is associated with microcephaly and short stature.[2][5][4]
Strabismus is the most commonly seen ophthalmologic abnormality. Ophthalmoplegia, nystagmus, ptosis, myopia, hyperopia, microphthalmia and lacrimal duct stenosis can also occur.[4] Otologic involvement can result in sensorineural hearing loss, conductive hearing loss and microtia.[1][3] Congenital heart defects such as tetralogy of Fallot, pulmonic stenosis, aortic insufficiency and ventricular septal defect have been reported. Infants with Beck–Fahrner syndrome can experience feeding difficulties and constipation. One case of associated pyloric stenosis has been seen. Hypospadias and cryptorchidism have been observed.[4]
Genetics
TET3 gene encodes for Tet methylcytosine dioxygenase 3 (TET3) which—similar to other TET enzymes—helps in mediating active DNA demethylation.[upper-alpha 1][7] TET3 catalyzes oxidative reaction of converting 5-methylcytosine (5mC) to 5-hydroxymethylcytosine (5hmC),[8] which is an intermediate step in DNA demethylation and hypothesized to be essential for neural development.[9] TET3 is expressed in embryonic stem cells, where it helps in sustaining neural stem cells and terminal differentiation of neurons.[10]
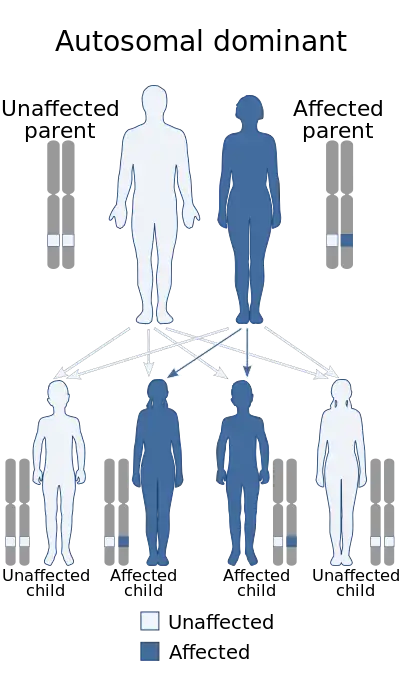
Beck–Fahrner syndrome is caused by homozygous, heterozygus or compound heterozygous mutations in the TET3 gene on chromosome 2 (2p13.1).[11] Nonsense, missense or frameshift mutations of the TET3 gene results in disruption of DNA demethylation during early embryogenesis and development of the nervous system.[2] It can occur de novo (genetic mutations occurring for the first time) or it can be inherited in an autosomal dominant manner with variable expressivity and hypomorphic alleles.[4] Some individuals affected with Beck–Fahrner syndrome have biallelic variants, which may indicate a possibility for autosomal recessive inheritance as well.[11] However, their family histories and DNA methylation profiling have been consistent with an autosomal dominant mode of inheritance.[4]
Diagnosis
Differential
Differential for Beck–Fahrner syndrome includes Bainbridge–Ropers syndrome, Fragile X syndrome, Heyn–Sproule–Jackson syndrome, Kabuki syndrome, Luscan–Lumish syndrome, Malan syndrome, Sotos syndrome, Tatton–Brown–Rahman syndrome, and other genetic disorders with similar clinical findings.[4]
Testing
While there is no consensus on criteria for diagnosis,[4] the presence of pathologic or likely-pathologic TET3 variants in setting of typical clinical findings helps in establishing the diagnosis.[12]
Levy et al. (2021) discovered a DNA methylation profile or epigenetic signature (episignature) specific to Beck–Fahrner syndrome, which demonstrates DNA hypermethylation.[1] This can be tested using whole blood genome-wide DNA methylation analysis, and can be used as an initial diagnostic test in suspected individuals.[13] It could also be used to confirm pathogenicity of a TET3 variant of uncertain significance.[4] Chromosomal microarray analysis—mainly used in work–up of neurodevelopmental disorders—has high sensitivity for identifying submicroscopic variations, microdeletions and duplications, and could also be used during initial testing.[14][4]
Several molecular and genetic testing methods are applied to identify mutations or variants. Multigene panels with TET3 gene, whole genome sequencing, exome sequencing, sequence analysis and single-gene testing followed by targeted gene deletion or duplication analysis could be used. Exome sequencing has been recommended in GeneReviews as the diagnostic test of choice due to the recency of Beck–Fahrner syndrome's delineation and TET3 gene analysis not being offered on most multigene panels.[4]
Management
Management is supportive and care is focused on improving quality of life. This is coordinated by medical genetics and pediatrics with a multidisciplinary team of specialists. Genetic counseling helps with educating the patients and their families about the condition, identifying the risk of other members having the condition, family planning, prenatal testing and preimplantation genetic diagnosis. Social work can be included to provide support to the families as needed; palliative, nursing home and respite care options can be explored when necessary.[4]
Autism therapies, early intervention and special education programs such as behavior therapy and speech therapy are recommended to mitigate complications of developmental delay and cognitive impairment. Additionally, clinical psychology and psychiatry would be consulted for management and treatment of behavioral and psychiatric disorders. Neurology would be involved when the patient develops epilepsy or if there is an indication for anticonvulsant therapy. Physical and occupational therapy can help with tone abnormalities and movement disorders; assistive technology such as mobility aid and standing frame can be used if required.[4]
Orthopedic surgery could be consulted for musculoskeletal deformities and dysmorphic features; back brace or surgical interventions can be explored as needed. Corrective surgery and monitoring for ophthalmic anomalies are per ophthalmology and optometry. Tympanostomy tube, hearing aids, cochlear implants are used as recommended by otorhinolaryngology and audiology. Cardiology and cardiothoracic surgery is involved for monitoring and correction of congenital heart defects. Feeding therapy can help address feeding difficulties; in cases of severe feeding difficulty nasogastric intubation or gastrostomy feeding tube placement is indicated. Urology evaluates and corrects genitourinary abnormalities when present.[4]
History
Beck–Fahrner syndrome was first described in 2020,[15] and was then termed "TET3 deficiency".[2] It was the first disorder impacting DNA demethylation to be delineated.[1] As of 2023, around 50 people have been diagnosed with this condition.[16]
Notes
- "TET" enzymes are a family of "ten-eleven translocation" methylcytosine dioxygenases.
References
- Levy, Michael A.; et al. (2021-11-08). "Deficiency of TET3 leads to a genome-wide DNA hypermethylation episignature in human whole blood". npj Genomic Medicine. Springer Nature. 6 (1): 92. doi:10.1038/s41525-021-00256-y. PMC 8576018. PMID 34750377.
- Beck, David B.; et al. (2020-01-09). "Delineation of a human mendelian disorder of the DNA demethylation machinery: TET3 deficiency". American Journal of Human Genetics. American Society of Human Genetics. 106 (2): 234–245. doi:10.1016/j.ajhg.2019.12.007. PMC 7010978. PMID 31928709.
- Seyama, Rie; et al. (2021-11-01). "Two families with TET3-related disorder showing neurodevelopmental delay with craniofacial dysmorphisms". Journal of Human Genetics. Japan Society of Human Genetics. 67 (3): 157–164. doi:10.1038/s10038-021-00986-y. PMID 34719681. S2CID 240355829. Retrieved 2023-07-16.
- Fahrner, Jill A. (2023-05-18). "TET3-related Beck–Fahrner syndrome". GeneReviews. NCBI. PMID 37200470. Retrieved 2023-07-15.
- "Beck–Fahrner syndrome". MedGen. NCBI. Retrieved 2023-07-22.
- Sager, Safiye Gunes; et al. (2022-09-30). "A novel de novo TET3 loss-of-function variant in a Turkish boy presenting with neurodevelopmental delay and electrical status epilepticus during slow-wave sleep". Brain and Development. Japanese Society of Child Neurology. 45 (2): 140–145. doi:10.1016/j.braindev.2022.09.004. PMID 36192301. S2CID 252620163. Retrieved 2023-07-16.
- Wu, Xiaoji; Zhang, Yi (2017-09-01). "TET-mediated active DNA demethylation: mechanism, function and beyond". Nature Reviews Genetics. Springer Nature. 18 (9): 517–534. doi:10.1038/nrg.2017.33. PMID 28555658. S2CID 3393814. Retrieved 2023-07-30.
- Wang, Zhiqin; et al. (2016-03-07). "DNA methylation dynamics in neurogenesis". Epigenomics. Future Medicine. 8 (3): 401–414. doi:10.2217/epi.15.119. PMC 4864063. PMID 26950681.
- MacArthur, Ian C.; Dawlaty, Meelad M. (2021-02-18). "TET enzymes and 5-hydroxymethylcytosine in neural progenitor cell biology and neurodevelopment". Frontiers in Cell and Developmental Biology. Frontiers Media. 9: 645335. doi:10.3389/fcell.2021.645335. PMC 7930563. PMID 33681230.
- Li, Ting; et al. (2014-05-18). "Critical role of TET3 in neural progenitor cell maintenance and terminal differentiation". Molecular Neurobiology. Springer Nature. 51 (1): 142–154. doi:10.1007/s12035-014-8734-5. PMID 24838624. S2CID 15337793. Retrieved 2023-07-30.
- "Beck–Fahrner syndrome; BEFAHRS". Online Mendelian Inheritance in Man. Johns Hopkins University School of Medicine. 2020-03-04. Retrieved 2023-07-15.
- Richards, Sue; et al. (2015-05-01). "Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology". Genetics in Medicine. American College of Medical Genetics and Genomics. 17 (5): 405–424. doi:10.1038/gim.2015.30. PMC 4544753. PMID 25741868.
- Sadikovic, Bekim; et al. (2021-06-01). "Clinical epigenomics: genome-wide DNA methylation analysis for the diagnosis of Mendelian disorders". Genetics in Medicine. American College of Medical Genetics. 23 (6): 1065–1074. doi:10.1038/s41436-020-01096-4. PMC 8187150. PMID 33547396.
- Batzir, Nurit Assia; Shohat, Mordechai; Maya, Idit (2015-09-01). "Chromosomal microarray analysis (CMA): a clinical diagnostic tool in the prenatal and postnatal settings". Pediatric Endocrinology Reviews. YS Medical Media. 13 (1): 448–454. PMID 26540760. Retrieved 2023-07-21.
- "What is Beck–Fahrner Syndrome? (BEFAHRS)". Beck–Fahrner Syndrome Foundation. 2021-10-10. Retrieved 2023-07-22.
- Doherty, Megan (2023-06-16). "Ashley Clifford is one of only 50 people with Beck–Fahrner syndrome". The Canberra Times. Australian Community Media. Retrieved 2023-07-23.