Signet ring cell carcinoma
Signet ring cell carcinoma (SRCC) is a rare form of highly malignant adenocarcinoma[1] that produces mucin. It is an epithelial malignancy characterized by the histologic appearance of signet ring cells.
| Signet ring cell carcinoma | |
|---|---|
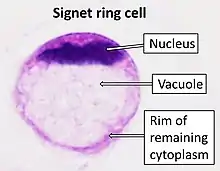 | |
| A signet ring cell, as seen in a case of colon adenocarcinoma with mucinous features, showing a tumor cell with a vacuole of mucin. H&E stain. | |
| Specialty | Oncology |
Primary SRCC tumors are most often found in the glandular cells of the stomach (SRCC originates in the stomach in 56 percent of patients),[2] and less frequently in the breast, gallbladder, urinary bladder, and pancreas.[3] SRCCs do not normally form in the lungs, though a few instances have been reported.
Among colorectal cancers, the prevalence of SRCC is less than one percent. Though incidence and mortality of gastric cancer has declined in many countries over the past 50 years, there has been an increase in occurrences of gastric SRCC-type cancers.[4]
SRCC tumors grow in characteristic sheets, which makes diagnosis using standard imaging techniques, like CT and PET scans, less effective.[5][6]
Causes
Some cases are inherited, and these cases are often caused by mutations in the CDH1 gene, which encodes the important cell–cell adhesion glycoprotein E-cadherin.[7][8] Somatic mutations of the APC gene have also been implicated in the development of gastric SRCCs.[9]
The role of other risk factors in gastric cancer such as salt-preserved food, smoking, auto-immune gastritis are not well studied in SRCC.[10]
Mechanism of formation
SRCCs are dedifferentiated adenocarcinomas that lose the capability for cell–cell interaction.
Highly differentiated adenocarcinomas form SRCCs via a loss of adherens and tight junctions that typically separate MUC4, a mucin protein, and ErbB2, an oncogenic receptor. When MUC4 and ErbB2 are able to interact, they trigger an activation loop. As a result, the ErbB2/ErbB3 signaling pathway becomes constitutively activated, cell–cell interactions are lost and signet carcinomas are formed. Constitutive action of the ErbB2/ErbB3 complex also enhances cell growth.[11]
The mechanism of this malignant cancer is still unclear; however, it has been found that a colon carcinoma cell known as HCC2998 causes an increase in differentiated tumor production. The reason for this increase is due to active PI3K that are converted to a SRCC-like cells.[12]
Metastasis
The pattern of metastasis is different for gastric signet cell carcinoma than for intestinal-type gastric carcinoma. The SRCC tumor is often seen in the peritoneum and has also been known to spread to lymphatic permeation of the lungs and to the ovaries, creating Krukenberg tumors.[13] Cases of gastric carcinomas metastasizing to the breast and forming signet-ring cells have also been reported. One study suggests that when signet-ring cells are found in a breast tumor, the presence of gastric cancer should also be considered.[14]
Histology
SRCCs are named due to their resemblance to signet rings, which result from the formation of large vacuoles full of mucin that displaces the nucleus to the cell's periphery.[15]
Stomach cancers with both adenocarcinoma and some SRC (known as mixed-SRCC) exhibit more aggressive behavior than purely SRCC or non-SRCC histologies.[16]
A study of SRCC colorectal cancers compared mucin-rich SRCC tumors and mucin-poor SRCC tumors. They concluded that the latter more frequently demonstrated adverse histologic features such as lymphatic invasion, venous invasion and perineural invasion.[17]
Treatment
Chemotherapy has relatively poor curative efficacy in SRCC patients and overall survival rates are lower compared to patients with more typical cancer pathology. SRCC cancers are usually diagnosed during the late stages of the disease, so the tumors generally spread more aggressively than non-signet cancers, making treatment challenging.[18] In the future, case studies indicate that bone marrow metastases will likely play a larger role in the diagnosis and management of signet ring cell gastric cancer.[19]
In SRCC of the stomach, removal of the stomach cancer is the treatment of choice. There is no combination of chemotherapy which is clearly superior to others, but most active regimens include 5-Fluorouracil (5-FU), Cisplatin, and/or Etoposide. Some newer agents, including Taxol and Gemcitabine (Gemzar) are under investigation.[20]
In a single case study of a patient with SRCC of the bladder with recurrent metastases, the patient exhibited a treatment response to palliative FOLFOX-6 chemotherapy.[21]
There are reports of occasional pulmonary tumour thrombotic microangiopathy leading to pulmonary hypertension and coagulation problems that could be successfully treated with Imatinib.
Prognosis by organ
These aggressive tumors are generally diagnosed at advanced stages and survival is generally shorter. The prognosis of SRCC and its chemosensitivity with specific regimens are still controversial as SRCC is not specifically identified in most studies and its poor prognosis may be due to its more advanced stage.[22] One study suggests that its dismal prognosis seems to be caused by its intrinsic tumor biology, suggesting an area for further research.[23]
Bladder
Primary signet-ring cell carcinoma of the urinary bladder is extremely rare and patient survival is very poor and occurs mainly in men ages 38 to 83. However, one such patient treated with a radical cystectomy followed by combined S-1 and Cisplatin adjuvant chemotherapy did demonstrate promising long-term survival of 90 months.[24]
Colorectal
Primary signet ring cell carcinoma of the colon and rectum (PSRCCR) is rare, with a reported incidence of less than 1 percent. It has a poor prognosis because symptoms often develop late and it is usually diagnosed at an advanced stage. Five-year survival rates in previous studies ranged from nine to 30 percent. Average survival was between 20 and 45 months.[25] It tends to affect younger adults with higher likelihood of lymphovascular invasion. It is worth noting that the overall survival rate of patients with SRCC was significantly poorer than that of patients with mucinous or poorly differentiated adenocarcinoma.[26]
In advanced gastric cancers, the prognosis for patients with the SRCCs was significantly worse than for the other histological types, which can be explained by the finding that advanced SRCC gastric cancers have a larger tumor size, more lymph node metastasis, a deeper invasive depth and more Borrmann type 4 lesions than other types.[27]
Stomach
When compared to adenocarcinoma stomach, SRCC in the stomach occurs more often in women and younger patients.[28] Patients with SRCC of the stomach show similar clinicopathological features to patients with undifferentiated histology. A recent study found that patients with SRCC had a better prognosis than patients with undifferentiated gastric carcinoma. However, when narrowed to patients with only advanced stage gastric cancer, those with SRCC had a worse prognosis than other cell types.[29]
.jpg.webp)
References
- el-Zimaity HM, Itani K, Graham DY (October 1997). "Early diagnosis of signet ring cell carcinoma of the stomach: role of the Genta stain". Journal of Clinical Pathology. 50 (10): 867–868. doi:10.1136/jcp.50.10.867. PMC 500272. PMID 9462273.
- Benesch MG, Mathieson A (June 2020). "Epidemiology of Signet Ring Cell Adenocarcinomas". Cancers. 12 (6): E1544. doi:10.3390/cancers12061544. PMC 7352645. PMID 32545410.
- Belli S, Aytac HO, Karagulle E, Yabanoglu H, Kayaselcuk F, Yildirim S (2014-01-01). "Outcomes of surgical treatment of primary signet ring cell carcinoma of the colon and rectum: 22 cases reviewed with literature". International Surgery. 99 (6): 691–698. doi:10.9738/INTSURG-D-14-00067.1. PMC 4254225. PMID 25437572.
- Henson DE, Dittus C, Younes M, Nguyen H, Albores-Saavedra J (July 2004). "Differential trends in the intestinal and diffuse types of gastric carcinoma in the United States, 1973-2000: increase in the signet ring cell type". Archives of Pathology & Laboratory Medicine. 128 (7): 765–770. doi:10.5858/2004-128-765-DTITIA. PMID 15214826.
- Shah RB, Zhou M (2011-09-29). Prostate Biopsy Interpretation: An Illustrated Guide. Springer Science & Business Media. ISBN 978-3-642-21369-4.
- Ro JY, Ayala AG, Shen SS (2012-04-20). Advances in Surgical Pathology: Prostate Cancer. Lippincott Williams & Wilkins. ISBN 978-1-60831-434-8.
- "Office of Rare Diseases Research: Diffuse Gastric Cancer". National Institute of Health. pp. 84–85. Retrieved 2012-11-21.
- Muta H, Noguchi M, Kanai Y, Ochiai A, Nawata H, Hirohashi S (August 1996). "E-cadherin gene mutations in signet ring cell carcinoma of the stomach". Japanese Journal of Cancer Research. 87 (8): 843–848. doi:10.1111/j.1349-7006.1996.tb02109.x. PMC 5921174. PMID 8797891.
- Nakatsuru S, Yanagisawa A, Ichii S, Tahara E, Kato Y, Nakamura Y, Horii A (November 1992). "Somatic mutation of the APC gene in gastric cancer: frequent mutations in very well differentiated adenocarcinoma and signet-ring cell carcinoma". Human Molecular Genetics. 1 (8): 559–563. doi:10.1093/hmg/1.8.559. PMID 1338691.
- Pernot S, Voron T, Perkins G, Lagorce-Pages C, Berger A, Taieb J (October 2015). "Signet-ring cell carcinoma of the stomach: Impact on prognosis and specific therapeutic challenge". World Journal of Gastroenterology. 21 (40): 11428–11438. doi:10.3748/wjg.v21.i40.11428. PMC 4616218. PMID 26523107.
- Fukui Y (August 2014). "Mechanisms behind signet ring cell carcinoma formation". Biochemical and Biophysical Research Communications. 450 (4): 1231–1233. doi:10.1016/j.bbrc.2014.07.025. PMID 25019985.
- Fukui Y (August 2014). "Mechanisms behind signet ring cell carcinoma formation". Biochemical and Biophysical Research Communications. 450 (4): 1231–1233. doi:10.1016/j.bbrc.2014.07.025. PMID 25019985.
- Duarte I, Llanos O (March 1981). "Patterns of metastases in intestinal and diffuse types of carcinoma of the stomach". Human Pathology. 12 (3): 237–242. doi:10.1016/S0046-8177(81)80124-4. PMID 7228019.
- Iesato A, Oba T, Ono M, Hanamura T, Watanabe T, Ito T, et al. (2014-12-29). "Breast metastases of gastric signet-ring cell carcinoma: a report of two cases and review of the literature". OncoTargets and Therapy. 8: 91–97. doi:10.2147/OTT.S67921. PMC 4284042. PMID 25565869.
- Portnoy LM (2006-05-05). Radiologic Diagnosis of Gastric Cancer: A new Outlook. Springer Science & Business Media. ISBN 978-3-540-29421-4.
- Huh CW, Jung DH, Kim JH, Lee YC, Kim H, Kim H, et al. (February 2013). "Signet ring cell mixed histology may show more aggressive behavior than other histologies in early gastric cancer". Journal of Surgical Oncology. 107 (2): 124–129. doi:10.1002/jso.23261. PMID 22991272. S2CID 206174013.
- Hartman DJ, Nikiforova MN, Chang DT, Chu E, Bahary N, Brand RE, et al. (July 2013). "Signet ring cell colorectal carcinoma: a distinct subset of mucin-poor microsatellite-stable signet ring cell carcinoma associated with dismal prognosis". The American Journal of Surgical Pathology. 37 (7): 969–977. doi:10.1097/PAS.0b013e3182851e2b. PMID 23681075. S2CID 19107084.
- Nitsche U, Zimmermann A, Späth C, Müller T, Maak M, Schuster T, et al. (November 2013). "Mucinous and signet-ring cell colorectal cancers differ from classical adenocarcinomas in tumor biology and prognosis". Annals of Surgery. 258 (5): 775–783. doi:10.1097/SLA.0b013e3182a69f7e. PMC 3888475. PMID 23989057.
- Dittus C, Mathew H, Malek A, Negroiu A (December 2014). "Bone marrow infiltration as the initial presentation of gastric signet ring cell adenocarcinoma". Journal of Gastrointestinal Oncology. 5 (6): E113–E116. doi:10.3978/j.issn.2078-6891.2014.050. PMC 4226827. PMID 25436133.
- "Signet Ring Cell Cancer | Oncolink - Cancer Resources". www.oncolink.org. Retrieved 2016-04-20.
- Pugashetti N, Yap SA, Lara PN, Gandour-Edwards R, Dall'Era MA (2015-01-01). "Metastatic signet-ring cell carcinoma of the urinary bladder: A novel management approach to a rare tumour". Canadian Urological Association Journal. 9 (3–4): E204–E207. doi:10.5489/cuaj.2447. PMC 4455640. PMID 26085880.
- Pernot S, Voron T, Perkins G, Lagorce-Pages C, Berger A, Taieb J (October 2015). "Signet-ring cell carcinoma of the stomach: Impact on prognosis and specific therapeutic challenge". World Journal of Gastroenterology. 21 (40): 11428–11438. doi:10.3748/wjg.v21.i40.11428. PMC 4616218. PMID 26523107.
- Nitsche U, Zimmermann A, Späth C, Müller T, Maak M, Schuster T, et al. (November 2013). "Mucinous and signet-ring cell colorectal cancers differ from classical adenocarcinomas in tumor biology and prognosis". Annals of Surgery. 258 (5): 775–783. doi:10.1097/SLA.0b013e3182a69f7e. PMC 3888475. PMID 23989057.
- Hamakawa T, Kojima Y, Naiki T, Kubota Y, Yasui T, Tozawa K, et al. (April 2013). "Long-term survival of a patient with invasive signet-ring cell carcinoma of the urinary bladder managed by combined s-1 and Cisplatin adjuvant chemotherapy". Case Reports in Urology. 2013: 915874. doi:10.1155/2013/915874. PMC 3664482. PMID 23738191.
- Belli S, Aytac HO, Karagulle E, Yabanoglu H, Kayaselcuk F, Yildirim S (2014-01-01). "Outcomes of surgical treatment of primary signet ring cell carcinoma of the colon and rectum: 22 cases reviewed with literature". International Surgery. 99 (6): 691–698. doi:10.9738/INTSURG-D-14-00067.1. PMC 4254225. PMID 25437572.
- Lee WS, Chun HK, Lee WY, Yun SH, Cho YB, Yun HR, et al. (September 2007). "Treatment outcomes in patients with signet ring cell carcinoma of the colorectum". American Journal of Surgery. 194 (3): 294–298. doi:10.1016/j.amjsurg.2006.12.041. PMID 17693269.
- Kim JP, Kim SC, Yang HK (August 1994). "Prognostic significance of signet ring cell carcinoma of the stomach". Surgical Oncology. 3 (4): 221–227. doi:10.1016/0960-7404(94)90037-x. PMID 7834113.
- Shah RB, Zhou M (2011-09-29). Prostate Biopsy Interpretation: An Illustrated Guide. Springer Science & Business Media. ISBN 978-3-642-21369-4.
- Kwon KJ, Shim KN, Song EM, Choi JY, Kim SE, Jung HK, Jung SA (January 2014). "Clinicopathological characteristics and prognosis of signet ring cell carcinoma of the stomach". Gastric Cancer. 17 (1): 43–53. doi:10.1007/s10120-013-0234-1. PMID 23389081. S2CID 8262409.