Diprenorphine
Diprenorphine (brand name Revivon; former developmental code name M5050),[1] also known as diprenorfin, is a non-selective, high-affinity, weak partial agonist of the μ- (MOR), κ- (KOR), and δ-opioid receptor (DOR) (with equal affinity) which is used in veterinary medicine as an opioid antagonist.[2][3][4] It is used to reverse the effects of super-potent opioid analgesics such as etorphine and carfentanil that are used for tranquilizing large animals. The drug is not approved for use in humans.[5]
 | |
| Clinical data | |
|---|---|
| Trade names | Revivon |
| Other names | Diprenorfin; M5050 |
| AHFS/Drugs.com | International Drug Names |
| ATCvet code | |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.034.826 |
| Chemical and physical data | |
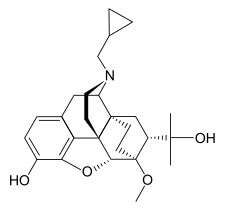
| Formula | C26H35NO4 |
| Molar mass | 425.569 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
| | |
Diprenorphine is the strongest opioid antagonist that is commercially available (some 100 times more potent as an antagonist than nalorphine),[6] and is used for reversing the effects of very strong opioids for which the binding affinity is so high that naloxone does not effectively or reliably reverse the narcotic effects.[7] These super-potent opioids, with the single exception of buprenorphine (which has an improved safety-profile due to its partial agonism character[8]), are not used in humans because the dose for a human is so small that it would be difficult to measure properly , so there is an excessive risk of overdose leading to fatal respiratory depression. However conventional opioid derivatives are not strong enough to rapidly tranquilize large animals, like elephants and rhinos, so drugs such as etorphine and carfentanil are available for this purpose.
Diprenorphine is considered to be the specific reversing agent/antagonist for etorphine and carfentanil,[9] and is normally used to remobilise animals once veterinary procedures have been completed.[10] Since diprenorphine also has partial agonistic properties of its own, it should not be used on humans if they are accidentally exposed to etorphine or carfentanil. Naloxone or naltrexone is the preferred human opioid receptor antagonist.[11]
In theory, diprenorphine could also be used as an antidote for treating overdose of certain opioid derivatives which are used in humans, particularly buprenorphine for which the binding affinity is so high that naloxone does not reliably reverse the narcotic effects. However, diprenorphine is not generally available in hospitals; instead a vial of diprenorphine is supplied with etorphine or carfentanil specifically for reversing the effects of the drug, so the use of diprenorphine for treating a buprenorphine overdose is not usually carried out in practice.
Because diprenorphine is a weak partial agonist of the opioid receptors rather than a silent antagonist, it can produce some opioid effects in the absence of other opioids at sufficient doses.[12] Moreover, due to partial agonism of the KOR, where it appears to possess significantly greater intrinsic activity relative to the MOR, diprenorphine can produce sedation as well as, in humans, hallucinations.[3][5][13][14][15]
References
- US 3433791, "Endoethano Nor Oripavines & Nor Thebaines"
- Lewis JW, Husbands SM (2004). "The orvinols and related opioids--high affinity ligands with diverse efficacy profiles". Current Pharmaceutical Design. 10 (7): 717–32. doi:10.2174/1381612043453027. PMID 15032698.
- Biegon A, Volkow ND (24 February 1995). Sites of Drug Action in the Human Brain. CRC Press. pp. 149–. ISBN 978-0-8493-7653-5.
- Shorvon SD, Perucca E, Fish D, Dodson WE (15 April 2008). The Treatment of Epilepsy. John Wiley & Sons. pp. 657–. ISBN 978-0-470-75245-6.
- Clarke KW, Trim CM (28 June 2013). Veterinary Anaesthesia. Elsevier Health Sciences. pp. 93–. ISBN 978-0-7020-5423-5.
- Furst S, Hosztafi S, Friedmann T (1995). "Structure-Activity Relationships of Synthetic and Semisynthetic Opioid Agonists and Antagonists". Current Medicinal Chemistry. 1 (6): 423–440.
- Takemori AE, Hayashi G, Smits SE (October 1972). "Studies on the quantitative antagonism of analgesics by naloxone and diprenorphine". European Journal of Pharmacology. 20 (1): 85–92. doi:10.1016/0014-2999(72)90219-1. PMID 4637947.
- "Medication Assisted Treatment". SAMHSA.gov. September 2015. p. 1.
- Jessup DA, Clark WE, Jones KR, Clark R, Lance WR (December 1985). "Immobilization of free-ranging desert bighorn sheep, tule elk, and wild horses, using carfentanil and xylazine: reversal with naloxone, diprenorphine, and yohimbine". Journal of the American Veterinary Medical Association. 187 (11): 1253–4. PMID 4077657.
- Alford BT, Burkhart RL, Johnson WP (April 1974). "Etorphine and diprenorphine as immobilizing and reversing agents in captive and free-ranging mammals". Journal of the American Veterinary Medical Association. 164 (7): 702–5. PMID 4817959.
- Caulkett NA, Arnemo JM (2007). "Chemical Immobilization of Free-Ranging Terrestrial Mammals.". In Tranquilli WJ, Thurmon JC, Grimm KA (eds.). Lumb and Jones' Veterinary Anesthesia and Analgesia (4th ed.). Philadelphia: Lippincott, Williams and Wilkins. p. 815.
- Wolfensohn S, Lloyd M (15 April 2008). Handbook of Laboratory Animal Management and Welfare. John Wiley & Sons. pp. 110–. ISBN 978-1-4051-4777-4.
- Miller RE, Fowler ME (11 July 2011). Fowler's Zoo and Wild Animal Medicine Current Therapy. Elsevier Health Sciences. pp. 1863–. ISBN 978-1-4377-1985-7.
- Harrie LS (1 July 1998). Problems of Drug Dependence: 1996 Proceedings of the 59th Annual Scientific Symposium. DIANE Publishing. pp. 155–. ISBN 978-0-7881-8130-6.
- Traynor JR, Corbett AD, Kosterlitz HW (May 1987). "Diprenorphine has agonist activity at opioid kappa-receptors in the myenteric plexus of the guinea-pig ileum". European Journal of Pharmacology. 137 (1): 85–9. doi:10.1016/0014-2999(87)90185-3. PMID 3038579.