Graded exercise therapy
Graded exercise therapy (GET) is a programme of physical activity that starts very slowly and gradually increases over time, intended as a treatment for chronic fatigue syndrome (CFS or ME/CFS). Most public health bodies, including the CDC and NICE, consider it ineffective, and its safety is disputed.[1][2][3] However, GET still enjoys support among a minority of clinicians and organizations.
| Graded exercise therapy | |
|---|---|
| Other names | GET |
| Specialty | Physical therapy |
Description
A graded exercise programme starts with a physiotherapist or exercise therapist assessing the patient's current abilities and negotiating goals. The patient then begins exercising at a level within their capabilities. The patient and therapist increase the duration of sessions, typically by 10-20% every 1-2 weeks, until they can perform 30 minutes of light exercise five times a week. Then the intensity is raised if desired.[4][5][6]
The exercise can be any activity that can be titrated, such as walking, jogging, swimming, using exercise machines, and these may be mixed to add variety. Increasing the intensity can be more challenging than increasing duration, and a heart rate monitor may be employed to track intensity. If exercise exacerbates a patient's symptoms, they may be encouraged to pause the increases until symptoms become manageable again.[4][5] In other cases, the patient is expected to continue fixed increases in activity regardless of the degree of post-exertional malaise they experience.[7]
Patients are told that if exercise provokes symptoms, it is a typical response to becoming more active rather than a pathological process that causes permanent damage. Adverse effects may be increased if the practitioner is unfamiliar with CFS or exercise is not ramped up appropriately.[4]
Model
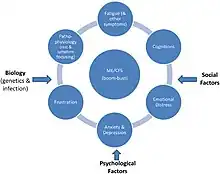
GET is based on the discredited model that people with ME/CFS avoid exerting themselves due to fear of triggering symptoms such as pain and fatigue, which causes deconditioning and further worsening of symptoms.[2][8] Excessive focus on symptoms and attributing illness to biological factors are also said perpetuate the illness.[8][5]
This model lacks evidence, contradicts patient experience, and fails to account for the biological evidence that ME/CFS is a serious medical condition.[8][9][10] Further, mental health problems or deconditioning do not cause ME/CFS.[11][12][13]
Effectiveness
Graded exercise therapy is generally considered to be an ineffective, outdated standard of care that can worsen the condition.[2] GET does not enable patients to increase their activity levels (as objectively measured by actigraphy)[14] or return to work.[15]
Major public health bodies recommend against GET. The CDC stopped recommending GET in 2017,[16] and says that people with ME/CFS do not tolerate vigorous exercise. NICE's 2021 guidance for ME/CFS removed graded exercise, which was recommended in the previous 2007 version,[17] and cautions against "any programme that...uses fixed incremental increases in physical activity or exercise, for example, graded exercise therapy."[18][7] According to NICE, studies of GET have been of poor or very poor quality.
Two regional departments of health, in New York state and Victoria, Australia, say GET is ineffective and potentially dangerous.[12][11] The Mayo Clinic consensus recommendations for the treatment of ME/CFS say GET is an outdated standard of care that can worsen the condition.[2]
ME/CFS patient organizations strongly oppose GET because they disagree that mental health problems are a cause of their illness and because many patients anecdotally report harms due to GET.[8]
As of 2015, the Royal Australian College of General Practitioners still supported graded exercise for CFS.[4]
Research
The available research into GET is of poor or very poor quality.[7][2] These studies generally have limited tracking of adverse effects,[3][2] employ outdated definitions of ME/CFS that do not require post-exertional malaise,[3] and rely on subjective self-reported outcome measures within unblinded trials, making them prone to placebo effects.[15]
The largest study on GET, the 2011 PACE trial, reported that GET and cognitive-behavioral therapy were safe and resulted in recovery for 22% of participants and improvement for 60%. There has since been considerable debate over the validity of the results. Outcome measures were modified mid-trial without a clear rationale.[19] When the data were reanalyzed utilising the original protocol, the rate of improvement was only 21%, and recovery was just 4%.[19] While trial participants reported subjective improvement, there was no clinically significant improvement in fitness according to the 6-minute walk test, an objective outcome.[15]
A 2022 review commissioned by the CDC concluded that weak evidence suggests that GET has "small to moderate" benefits, including reduced fatigue, decreased depression and anxiety, and better sleep. It said these results are of uncertain relevance to people with severe ME/CFS, a diagnosis according to modern criteria, or post-exertional malaise. According to the review, limited evidence suggests that GET is not harmful, but that reporting of harms was "suboptimal."[20]
A 2019 Cochrane review of 8 studies concluded that GET "probably" reduces fatigue but that evidence on long-term effectiveness and potential harms are very limited. The studies analyzed employed older definitions of CFS, so the effects on current patient cohorts may be different.[21] An independent analysis of the same studies reached the opposite conclusion based on the unreliability of subjective outcomes in unblinded trials, lack of objective improvements in physical fitness and employment, and insufficient tracking of adverse events.[15]
The ME Association asserts that GET causes a significant fraction of patients to get worse: 30% to 50% in self-reported patient questionnaires.[22] According to the Mayo Clinic Proceedings recommendations, 54% to 74% reported harm.[2]
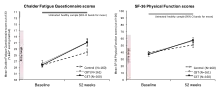
In 2021, a small study was published concerning the efficiency of GET at a specialist clinic in London, England. The patients were adults had an confirmed diagnosis of CFS according to NICE guidelines ("fatigue to be present for at least four months"). The study concluded that "GET therapy is a safe and efficacious treatment for patients with CFS/ME in a clinical specialist environment". Over the course of the treatment the average SF-36 Physical Functioning Subscale rose from 45.42 to 54.44, and the Work and Social Adjustment Scale (WSAS) fell from 25.25 to 21.48.[23] However, an independent review of this study showed that fewer than half of the patients actually completed the full number of treatment sessions suggesting they were poorly tolerated, and that the data did not support the conclusion of "efficacious treatment"; a Physical functioning (SF-36) score of 65 or less still equates to "severe disability" and a WSAS score of greater than 20 indicates "moderately severe disability".[24]
Graded exercise therapy has also been tested against fatigue and post-exertional malaise in long COVID, but found ineffective.[25]
References
- "Myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS) - Treatment". nhs.uk. 2017-10-20. Retrieved 2023-01-20.
- Bateman L, Bested AC, Bonilla HF, Chheda BV, Chu L, Curtin JM, et al. (November 2021). "Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management". Mayo Clinic Proceedings. 96 (11): 2861–2878. doi:10.1016/j.mayocp.2021.07.004. PMID 34454716. S2CID 237419583.
- Diagnosis and Management of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Agency for Healthcare Research and Quality. 2016.
- "Graded exercise therapy: chronic fatigue syndrome". Royal Australian College of General Practitioners. March 2015. Archived from the original on 2022-11-11.
- Sharpe M, Chalder T, White PD (February 2022). "Evidence-Based Care for People with Chronic Fatigue Syndrome and Myalgic Encephalomyelitis". Journal of General Internal Medicine. 37 (2): 449–452. doi:10.1007/s11606-021-07188-4. PMC 8811058. PMID 34791590.
- Larun L, Brurberg KG, Odgaard-Jensen J, Price JR, et al. (Cochrane Common Mental Disorders Group) (October 2019). "Exercise therapy for chronic fatigue syndrome". The Cochrane Database of Systematic Reviews. 10 (10): CD003200. doi:10.1002/14651858.CD003200.pub8. PMC 6953363. PMID 31577366.
- "Chronic fatigue syndrome/myalgic encephalomyelitis (or encephalopathy): diagnosis and management | Guidance | NICE". www.nice.org.uk.
- Geraghty K, Jason L, Sunnquist M, Tuller D, Blease C, Adeniji C (2019). "The 'cognitive behavioural model' of chronic fatigue syndrome: Critique of a flawed model". Health Psychology Open. 6 (1): 2055102919838907. doi:10.1177/2055102919838907. PMC 6482658. PMID 31041108.
- Shepherd CB (August 2017). "PACE trial claims for recovery in myalgic encephalomyelitis/chronic fatigue syndrome - true or false? It's time for an independent review of the methodology and results". Journal of Health Psychology. 22 (9): 1187–1191. doi:10.1177/1359105317703786. PMID 28805522. S2CID 22307162.
- "Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) | CDC". www.cdc.gov. 2022-12-29. Retrieved 2023-03-05.
(ME/CFS) is a serious, long-term illness...
- Department of Health & Human Services. "Chronic fatigue syndrome (CFS)". www.betterhealth.vic.gov.au. Retrieved 2023-03-05.
A person with ME/CFS should never be coaxed to push past their limit as this can be dangerous and cause long-term relapse.
- "Myalgic Encephalomyelitis ("Chronic Fatigue Syndrome")". health.ny.gov. Retrieved 2023-03-05.
- Ghali A, Lacombe V, Ravaiau C, Delattre E, Ghali M, Urbanski G, Lavigne C (June 2023). "The relevance of pacing strategies in managing symptoms of post-COVID-19 syndrome". Journal of Translational Medicine. 21 (1): 375. doi:10.1186/s12967-023-04229-w. PMC 10248991. PMID 37291581.
Nevertheless, a large number of studies demonstrated that deconditioning does not perpetuate or explain the symptoms in these patients.
- Vink M, Vink-Niese A (May 2022). "The Updated NICE Guidance Exposed the Serious Flaws in CBT and Graded Exercise Therapy Trials for ME/CFS". Healthcare. 10 (5): 898. doi:10.3390/healthcare10050898. PMC 9141828. PMID 35628033.
- Vink M, Vink-Niese F (2020-01-01). "Graded exercise therapy does not restore the ability to work in ME/CFS - Rethinking of a Cochrane review". Work. 66 (2): 283–308. doi:10.3233/WOR-203174. PMID 32568149. S2CID 219974354.
- Doucleff M (2017-10-02). "For People With Chronic Fatigue Syndrome, More Exercise Isn't Better". NPR. Retrieved 2023-03-05.
- Chronic fatigue syndrome/myalgic encephalomyelitis (or encephalopathy)—Diagnosis and management of CFS/ME in adults and children (PDF). National Institute of Clinical Excellence. 2007. p. 53. Archived from the original (PDF) on 2014-04-16.
- "Treatment of ME/CFS". Centers for Disease Control and Prevention. Retrieved November 19, 2019.
- Wilshire CE, Kindlon T, Courtney R, Matthees A, Tuller D, Geraghty K, Levin B (March 2018). "Rethinking the treatment of chronic fatigue syndrome-a reanalysis and evaluation of findings from a recent major trial of graded exercise and CBT". BMC Psychology. 6 (1): 6. doi:10.1186/s40359-018-0218-3. PMC 5863477. PMID 29562932.
- Management of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): An Updated Systematic Evidence Review (PDF). Centers for Disease Control and Prevention. 2022. pp. ii–iii, 23.
- Larun L, Brurberg KG, Odgaard-Jensen J, Price JR, et al. (Cochrane Common Mental Disorders Group) (October 2019). "Exercise therapy for chronic fatigue syndrome". The Cochrane Database of Systematic Reviews. 10 (10): CD003200. doi:10.1002/14651858.CD003200.pub8. PMC 6953363. PMID 31577366.
- "ME Association position on graded exercise therapy (GET) | 11 May 2008 | The ME Association". meassociation.org.uk. 2008-05-11.
- Smakowski A, Adamson J, Turner T, Chalder T (October 2022). "Graded exercise therapy for patients with chronic fatigue syndrome in secondary care - a benchmarking study". Disability and Rehabilitation. 44 (20): 5878–5886. doi:10.1080/09638288.2021.1949049. PMID 34498994. S2CID 237453889.
- Vink M, Vink-Niese A, Tyson SF (March 2022). "Patients with CFS remain severely disabled after treatment with graded exercise therapy in a specialist clinic in the UK Response to Smakowski et al". Disability and Rehabilitation: 1–2. doi:10.1080/09638288.2022.2048911. PMID 35306926. S2CID 247584261.
- Ghali A, Lacombe V, Ravaiau C, Delattre E, Ghali M, Urbanski G, Lavigne C (June 2023). "The relevance of pacing strategies in managing symptoms of post-COVID-19 syndrome". Journal of Translational Medicine. 21 (1): 375. doi:10.1186/s12967-023-04229-w. PMC 10248991. PMID 37291581.