Hypothalamic–pituitary–gonadal axis
The hypothalamic–pituitary–gonadal axis (HPG axis, also known as the hypothalamic–pituitary–ovarian/testicular axis) refers to the hypothalamus, pituitary gland, and gonadal glands as if these individual endocrine glands were a single entity. Because these glands often act in concert, physiologists and endocrinologists find it convenient and descriptive to speak of them as a single system.
The HPG axis plays a critical part in the development and regulation of a number of the body's systems, such as the reproductive and immune systems. Fluctuations in this axis cause changes in the hormones produced by each gland and have various local and systemic effects on the body.
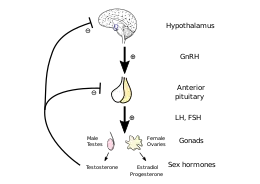
The axis controls development, reproduction, and aging in animals. Gonadotropin-releasing hormone (GnRH) is secreted from the hypothalamus by GnRH-expressing neurons. The anterior portion of the pituitary gland produces luteinizing hormone (LH) and follicle-stimulating hormone (FSH), and the gonads produce estrogen and testosterone.
In oviparous organisms (e.g. fish, reptiles, amphibians, birds), the HPG axis is commonly referred to as the hypothalamus-pituitary-gonadal-liver axis (HPGL-axis) in females. Many egg-yolk and chorionic proteins are synthesized heterologously in the liver, which are necessary for ovocyte growth and development. Examples of such necessary liver proteins are vitellogenin and choriogenin.
The HPA, HPG, and HPT axes are three pathways in which the hypothalamus and pituitary direct neuroendocrine function.
Location and regulation
.svg.png.webp)
The hypothalamus is located in the brain and secretes GnRH.[1] GnRH travels down the anterior portion of the pituitary via the hypophyseal portal system and binds to receptors on the secretory cells of the adenohypophysis.[2] In response to GnRH stimulation these cells produce LH and FSH, which travel into the blood stream.[3]
These two hormones play an important role in communicating to the gonads. In females FSH and LH act primarily to activate the ovaries to produce estrogen and inhibin and to regulate the menstrual cycle and ovarian cycle. Estrogen forms a negative feedback loop by inhibiting the production of GnRH in the hypothalamus. Inhibin acts to inhibit activin, which is a peripherally produced hormone that positively stimulates GnRH-producing cells. Follistatin, which is also produced in all body tissue, inhibits activin and gives the rest of the body more control over the axis. In males LH stimulates the interstitial cells located in the testes to produce testosterone, and FSH plays a role in spermatogenesis. Only small amounts of estrogen are secreted in males. Recent research has shown that a neurosteroid axis exists, which helps the cortex to regulate the hypothalamus's production of GnRH.[4]
In addition, leptin and insulin have stimulatory effects and ghrelin has inhibitory effects on gonadotropin-releasing hormone (GnRH) secretion from the hypothalamus.[5] Kisspeptin also influences GnRH secretion.[6]
Function
Reproduction
One of the most important functions of the HPG axis is to regulate reproduction by controlling the uterine and ovarian cycles.[7] In females, the positive feedback loop between estrogen and luteinizing hormone help to prepare the follicle in the ovary and the uterus for ovulation and implantation. When the egg is released, the empty follicle sac begins to produce progesterone to inhibit the hypothalamus and the anterior pituitary thus stopping the estrogen-LH positive feedback loop. If conception occurs, the placenta will take over the secretion of progesterone; therefore the mother cannot ovulate again. If conception does not occur, decreasing excretion of progesterone will allow the hypothalamus to restart secretion of GnRH. These hormone levels also control the uterine (menstrual) cycle causing the proliferation phase in preparation for ovulation, the secretory phase after ovulation, and menstruation when conception does not occur. The activation of the HPG axis in both males and females during puberty also causes individuals to acquire secondary sex characteristics.
In males, the production of GnRH, LH, and FSH are similar, but the effects of these hormones are different.[8] FSH stimulates sustentacular cells to release androgen-binding protein, which promotes testosterone binding. LH binds to the interstitial cells, causing them to secrete testosterone. Testosterone is required for normal spermatogenesis and inhibits the hypothalamus. Inhibin is produced by the spermatogenic cells, which, also through inactivating activin, inhibits the hypothalamus. After puberty these hormones levels remain relatively constant.
Life cycle
The activation and deactivation of the HPG axis also helps to regulate life cycles.[7] At birth FSH and LH levels are elevated, and females also have a lifetime supply of primary oocytes. These levels decrease and remain low through childhood. During puberty the HPG axis is activated by the secretions of estrogen from the ovaries or testosterone from the testes. This activation of estrogen and testosterone causes physiological and psychological changes. Once activated, the HPG axis continues to function in men for the rest of their life but becomes deregulated in women, leading to menopause. This deregulation is caused mainly by the lack of oocytes that normally produce estrogen to create the positive feedback loop. Over several years, the activity the HPG axis decreases and women are no longer fertile.[9]
Although males remain fertile until death, the activity of the HPG axis decreases. As males age, the testes begin to produce less testosterone, leading to a condition known as post-pubertal hypogonadism.[8] The cause of the decreased testosterone is unclear and a current topic of research. Post-pubertal hypogonadism results in progressive muscle mass decrease, increase in visceral fat mass, loss of libido, impotence, decreased attention, increased risk of fractures, and abnormal sperm production.
Sexual dimorphism and behavior
Sex steroids also affect behavior, because sex steroids affect the brains structure and functioning. During development, hormones help determine how neurons synapse and migrate to result in sexual dimorphisms.[10] These physical differences lead to differences in behavior. While GnRH has not been shown to have any direct influence on regulating brain structure and function, gonadotropins, sex steroids, and activin have been shown to have such effects. It is thought that FSH may have an important role in brain development and differentiation.
Testosterone levels have been shown to relate to prosocial behavior.[11] This helps create synaptogenesis by promoting neurite development and migration. Activin promotes neural plasticity throughout the lifespan and regulates the neurotransmitters of peripheral neurons. Environment can also affect hormones and behavior interaction.[12]
Clinical relevance
Disorders
Disorders of the hypothalamic–pituitary–gonadal axis are classified by the World Health Organization (WHO) as:[13]
- WHO group I of ovulation disorders: Hypothalamic–pituitary failure
- WHO group II of ovulation disorders: Hypothalamic–pituitary dysfunction. WHO group II is the most common cause of ovulation disorders, and the most common causative member is polycystic ovary syndrome (PCOS).[14]
Gene mutations
Genetic mutations and chromosomal abnormalities are two sources of HPG axis alteration.[15] Single mutations usually lead to changes in binding ability of the hormone and receptor leading to inactivation or over activation. These mutations can occur in the genes coding for GnRH, LH, and FSH or their receptors. Depending on which hormone and receptor are unable to bind different effects occur but all alter the HPG axis.
For example, the male mutation of the GnRH coding gene could result in hypogonadotrophic hypogonadism. A mutation that cause a gain of function for LH receptor can result in a condition known as testotoxicosis, which cause puberty to occur between ages 2–3 years. Loss of function of LH receptors can cause male pseudohermaphroditism. In females mutations would have analogous effects. Hormone replacement can be used to initiate puberty and continue if the gene mutation occurs in the gene coding for the hormone. Chromosomal mutations tend to affect the androgen production rather than the HPG axis.
Suppression
The HPG axis can be suppressed by hormonal birth control administration. Although often described as preventing pregnancy by mimicking the pregnancy state, hormonal birth control is effective because it works on the HPG axis to mimic the luteal phase of a woman's cycle. The primary active ingredients are synthetic progestins, which mimic biologically derived progesterone. The synthetic progestin prevents the hypothalamus from releasing GnRH and the pituitary from releasing LH and FSH; therefore it prevents the ovarian cycle from entering the menstrual phase and prevents follicle development and ovulation. Also as a result, many of the side effects are similar to the symptoms of pregnancy. Alzheimer's has been shown to have a hormonal component, which could possibly be used as a method to prevent the disease.[16] Male contraceptives utilizing sex hormones approach the problem in a similar way.
The HPG axis can also be suppressed by GnRH antagonists or continuous administration of GnRH agonist, such as in the following applications
- Ovarian suppression as breast cancer management, to prevent the body's formation of estrogen which may stimulate breast cancer cells. This is generally done by continuous administration of GnRH agonist.
- Ovulation suppression as part of controlled ovarian hyperstimulation in in vitro fertilization, in order to prevent the spontaneous ovulation of ovarian follicles before they can be harvested.
Stimulation
Ovulation induction is usually initially performed by giving an antiestrogen such as clomifene citrate or letrozole in order to decrease negative feedback on the pituitary gland, resulting in an increase in FSH with the aim of increasing folliculogenesis. It is the main initial medical treatment for anovulation.
Environment factors
Environment can have large impact on the HPG axis. For example, women with eating disorders tend to have oligomenorrhea and secondary amenorrhea. Starvation from anorexia nervosa or bulimia causes the HPG axis to deactivate causing women's ovarian and uterine cycles to stop. Stress, physical exercise, and weight loss have been correlated with oligomenorrhea and secondary amenorrhea.[17] Similarly environmental factors can also affect men such as stress causing impotence. Prenatal exposure to alcohol can affect the hormones regulating fetal development resulting in foetal alcohol spectrum disorder.[18]
Comparative anatomy
The HPG axis is highly conserved in the animal kingdom.[19] While reproductive patterns may vary, the physical components and control mechanisms remain the same. The same hormones are used with some minor evolutionary modifications. Much of the research is done on animal models, because they mimic so well the control mechanism of humans. It is important to remember humans are the only species to hide their fertile period, but this effect is a difference in the effect of the hormones rather than a difference in the HPG axis.
See also
References
- Millar RP, Lu ZL, Pawson AJ, Flanagan CA, Morgan K, Maudsley SR (April 2004). "Gonadotropin-releasing hormone receptors". Endocr. Rev. 25 (2): 235–75. doi:10.1210/er.2003-0002. PMID 15082521.
- Charlton H (June 2008). "Hypothalamic control of anterior pituitary function: a history". J. Neuroendocrinol. 20 (6): 641–6. doi:10.1111/j.1365-2826.2008.01718.x. PMID 18601683. S2CID 16955603.
- Vadakkadath Meethal S, Atwood CS (February 2005). "The role of hypothalamic-pituitary-gonadal hormones in the normal structure and functioning of the brain". Cell. Mol. Life Sci. 62 (3): 257–70. doi:10.1007/s00018-004-4381-3. PMID 15723162.
- Meethal SV, Liu T, Chan HW, Ginsburg E, Wilson AC, Gray DN, Bowen RL, Vonderhaar BK, Atwood CS (August 2009). "Identification of a regulatory loop for the synthesis of neurosteroids: a steroidogenic acute regulatory protein-dependent mechanism involving hypothalamic-pituitary-gonadal axis receptors". J. Neurochem. 110 (3): 1014–27. doi:10.1111/j.1471-4159.2009.06192.x. PMC 2789665. PMID 19493163.
- Comninos, A. N.; Jayasena, C. N.; Dhillo, W. S. (2013). "The relationship between gut and adipose hormones, and reproduction". Human Reproduction Update. 20 (2): 153–74. doi:10.1093/humupd/dmt033. PMID 24173881.
- Skorupskaite, K.; George, J. T.; Anderson, R. A. (2014). "The kisspeptin-GnRH pathway in human reproductive health and disease". Human Reproduction Update. 20 (4): 485–500. doi:10.1093/humupd/dmu009. ISSN 1355-4786. PMC 4063702. PMID 24615662.
- Katja Hoehn; Marieb, Elaine Nicpon (2007). Human anatomy & physiology. San Francisco: Pearson Benjamin Cummings. pp. 1090–1110. ISBN 978-0-8053-5909-1.
- Veldhuis JD, Keenan DM, Liu PY, Iranmanesh A, Takahashi PY, Nehra AX (February 2009). "The aging male hypothalamic-pituitary-gonadal axis: pulsatility and feedback". Mol. Cell. Endocrinol. 299 (1): 14–22. doi:10.1016/j.mce.2008.09.005. PMC 2662347. PMID 18838102.
- Downs JL, Wise PM (February 2009). "The role of the brain in female reproductive aging". Mol. Cell. Endocrinol. 299 (1): 32–8. doi:10.1016/j.mce.2008.11.012. PMC 2692385. PMID 19063938.
- Hines M (July 1982). "Prenatal gonadal hormones and sex differences in human behavior". Psychol Bull. 92 (1): 56–80. doi:10.1037/0033-2909.92.1.56. PMID 7134329.
- Wibral M, Dohmen T, Klingmüller D, Weber B, Falk A (2012). "Testosterone Administration Reduces Lying in Men". PLOS ONE. 7 (10): e46774. Bibcode:2012PLoSO...746774W. doi:10.1371/journal.pone.0046774. PMC 3468628. PMID 23071635.
- Shepard KN, Michopoulos V, Toufexis DJ, Wilson ME (May 2009). "Genetic, epigenetic and environmental impact on sex differences in social behavior". Physiol. Behav. 97 (2): 157–70. doi:10.1016/j.physbeh.2009.02.016. PMC 2670935. PMID 19250945.
- Page 54 in: Guillebaud, John; Enda McVeigh; Roy Homburg (2008). Oxford handbook of reproductive medicine and family planning. Oxford [Oxfordshire]: Oxford University Press. ISBN 978-0-19-920380-2.
- Baird, D. T.; Balen, A.; Escobar-Morreale, H. F.; Evers, J. L. H.; Fauser, B. C. J. M.; Franks, S.; Glasier, A.; Homburg, R.; La Vecchia, C.; Devroey, P.; Diedrich, K.; Fraser, L.; Gianaroli, L.; Liebaers, I.; Sunde, A.; Tapanainen, J. S.; Tarlatzis, B.; Van Steirteghem, A.; Veiga, A.; Crosignani, P. G.; Evers, J. L. H. (2012). "Health and fertility in World Health Organization group 2 anovulatory women". Human Reproduction Update. 18 (5): 586–599. doi:10.1093/humupd/dms019. PMID 22611175.
- Isidori AM, Giannetta E, Lenzi A (2008). "Male hypogonadism". Pituitary. 11 (2): 171–80. doi:10.1007/s11102-008-0111-9. PMID 18404386. S2CID 20813241.
- Haasl RJ, Ahmadi MR, Meethal SV, Gleason CE, Johnson SC, Asthana S, Bowen RL, Atwood CS (2008). "A luteinizing hormone receptor intronic variant is significantly associated with decreased risk of Alzheimer's disease in males carrying an apolipoprotein E epsilon4 allele". BMC Med. Genet. 9: 37. doi:10.1186/1471-2350-9-37. PMC 2396156. PMID 18439297.
- Wiksten-Almströmer M, Hirschberg AL, Hagenfeldt K (2007). "Menstrual disorders and associated factors among adolescent girls visiting a youth clinic". Acta Obstet Gynecol Scand. 86 (1): 65–72. doi:10.1080/00016340601034970. PMID 17230292. S2CID 24096186.
- Weinberg J, Sliwowska JH, Lan N, Hellemans KG (April 2008). "Prenatal alcohol exposure: fetal programming, the hypothalamic-pituitary-adrenal axis and sex differences in outcome". J. Neuroendocrinol. 20 (4): 470–88. doi:10.1111/j.1365-2826.2008.01669.x. PMC 8942074. PMID 18266938. S2CID 4574957.
- Sower SA, Freamat M, Kavanaugh SI (March 2009). "The origins of the vertebrate hypothalamic-pituitary-gonadal (HPG) and hypothalamic-pituitary-thyroid (HPT) endocrine systems: new insights from lampreys". Gen. Comp. Endocrinol. 161 (1): 20–9. doi:10.1016/j.ygcen.2008.11.023. PMID 19084529.