Ménétrier's disease
Ménétrier disease is a rare, acquired, premalignant disease of the stomach characterized by massive gastric folds, excessive mucous production with resultant protein loss, and little or no acid production. The disorder is associated with excessive secretion of transforming growth factor alpha (TGF-α).[1] It is named after a French physician Pierre Eugène Ménétrier, 1859–1935.
| Ménétrier disease | |
|---|---|
| Other names | Hypoproteinemic hypertrophic gastropathy |
 | |
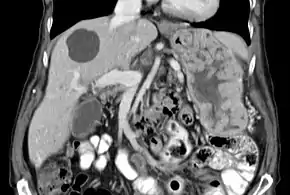
| Biopsy of the stomach in Ménétrier disease showing the substantial pit hyperplasia makes the large rugal folds appear to be covered by myriad polyps resembling hyperplastic polyps. The muscularis propria is the folded structure at the bottom center. | |
| Specialty | Gastroenterology |
Signs and symptoms
Individuals with the disease present with upper abdominal pain (epigastric), at times accompanied by nausea, vomiting, loss of appetite, edema, weakness, and weight loss. A small amount of gastrointestinal bleeding may occur, which is typically due to superficial mucosal erosions; large volume bleeding is rare.[2] 20% to 100% of patients, depending on time of presentation, develop a protein-losing gastropathy accompanied by low blood albumin and edema.[2][3]
Symptoms and pathological features of Ménétrier disease in children are similar to those in adults, but disease in children is usually self-limited and often follows respiratory infection.[4]
Cause
The cause of Ménétrier disease is unknown, but it has been associated with HCMV infection in children and H. pylori infections in adults.[5] Additionally, increased TGF-α has been noted in the gastric mucosa of patients with the disease.[1]
Pathology
With Ménétrier disease, the stomach is characterized by large, tortuous gastric folds in the fundus and body, with the antrum generally spared, giving the mucosa a cobblestone or cerebriform (brain-like) appearance.[5] Histologically, the most characteristic feature is massive foveolar hyperplasia (hyperplasia of surface and glandular mucous cells).[3] The glands are elongated with a corkscrew-like appearance and cystic dilation is common. Inflammation is usually only modest, although some cases show marked intraepithelial lymphocytosis. Diffuse or patchy glandular atrophy, evident as hypoplasia of parietal and chief cells, is typical.[4]
Although ICD-10 classifies it under "Other gastritis" (K29.6), and the lamina propria may contain mild chronic inflammatory infiltrate, Ménétrier disease is not considered a form of gastritis.[3] It is rather considered one of the two most well understood hypertrophic gastropathies; the other being Zollinger–Ellison syndrome.[4]
Diagnosis
The large folds of the stomach, as seen in Ménétrier disease, are easily detected by x-ray imaging following a barium meal or by endoscopic methods. Endoscopy with deep mucosal biopsy (and cytology) is required to establish the diagnosis and exclude other entities that may present similarly. A non-diagnostic biopsy may lead to a surgically obtained full-thickness biopsy to exclude malignancy.[3] CMV and helicobacter pylori serology should be a part of the evaluation.
Twenty-four-hour pH monitoring reveals hypochlorhydria or achlorhydria, and a chromium-labelled albumin test reveals increased GI protein loss.[5] Serum gastrin levels will be within normal limits.
Other possible causes (eg differential diagnosis) of large folds within the stomach include: Zollinger-Ellison syndrome, cancer, infection (cytomegalovirus/CMV, histoplasmosis, syphilis), and infiltrative disorders such as sarcoidosis.[3]
Treatment
Cetuximab is the first-line therapy for Ménétrier disease.[2] Cetuximab is a monoclonal antibody against epidermal growth factor receptor (EGFR), and has been shown to be effective in treating Ménétrier disease.[6]
Several medications have been used in the treatment of the condition, with variable efficacy. Such medications include: anticholinergic agents, prostaglandins, proton pump inhibitors, prednisone, and H2 receptor antagonists. Anticholinergics decrease protein loss. A high-protein diet should be recommended to replace protein loss in patients with low levels of albumin in the blood (hypoalbuminemia). Any ulcers discovered during the evaluation should be treated in standard fashion.
Severe disease with persistent and substantial protein loss despite cetuximab may require total removal of the stomach, especially when the disease is debilitating or irretractable or when there is a high risk for developing gastric cancer.[7] Subtotal gastrectomy is performed by some; it may be associated with higher morbidity and mortality secondary to the difficulty in obtaining a patent and long-lasting anastomosis between normal and hyperplastic tissue. In adults, there is no FDA approved treatment other than gastrectomy and a high-protein diet. Cetuximab is approved for compassionate use in the treatment of the disease.[8]
Pediatric cases are normally treated for symptoms with the disease clearing up in weeks to months.
Epidemiology
The average age of onset is 40 to 60 years, and men are affected more often than women.[2] Risk of gastric adenocarcinoma is increased in adults with Ménétrier disease.[4][5]
References
- Coffey, Robert J.; Washington, Mary Kay; Corless, Christopher L.; Heinrich, Michael C. (2 January 2007). "Ménétrier disease and gastrointestinal stromal tumors: hyperproliferative disorders of the stomach". Journal of Clinical Investigation. 117 (1): 70–80. doi:10.1172/JCI30491. PMC 1716220. PMID 17200708.
- Kasper, Dennis L.; Fauci, Anthony S.; Hauser, Stephen L.; Longo, Dan L.; Jameson, J. Larry; Loscalzo, Joseph (2015). Harrison's Principles of Internal Medicine (19th ed.). McGraw Hill Professional. p. 1932. ISBN 978-0-07-180216-1.
- Longo, Dan; Fauci, Anthony; Kasper, Dennis; Hauser, Stephen; Jameson, J.; Loscalzo, Joseph (2011). Harrison's Principles of Internal Medicine (18th ed.). McGraw Hill Professional. p. 2459. ISBN 978-0-07-174890-2.
- Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon C. (2009). Robbins & Cotran Pathologic Basis of Disease. Elsevier Health Sciences. p. 782. ISBN 978-1-4377-2015-0.
- Kumar et al., Pathologic Basis of Disease, 2e , pg 768
- Burdick, J. Steven; Chung, EunKyung; Tanner, Gordon; Sun, Mei; Paciga, June E.; Cheng, Jin Q.; Washington, Kay; Goldenring, James R.; Coffey, Robert J. (7 December 2000). "Treatment of Ménétrier's Disease with a Monoclonal Antibody against the Epidermal Growth Factor Receptor". New England Journal of Medicine. 343 (23): 1697–1701. doi:10.1056/NEJM200012073432305. PMID 11106719.
- Huh, Won Jae; Coffey, Robert J.; Washington, Mary Kay (January 2016). "Ménétrier's Disease: Its Mimickers and Pathogenesis". Journal of Pathology and Translational Medicine. 50 (1): 10–16. doi:10.4132/jptm.2015.09.15. PMC 4734964. PMID 26689786.
- Fiske, William H.; Tanksley, Jarred; Nam, Ki Taek; Goldenring, James R.; Slebos, Robbert J. C.; Liebler, Daniel C.; Abtahi, Amir M.; La Fleur, Bonnie; Ayers, Gregory D.; Lind, Christopher D.; Washington, Mary K.; Coffey, Robert J. (25 November 2009). "Efficacy of Cetuximab in the Treatment of Ménétrier's Disease". Science Translational Medicine. 1 (8): 8ra18. doi:10.1126/scitranslmed.3000320. PMC 3638759. PMID 20368185.