Agonist-antagonist
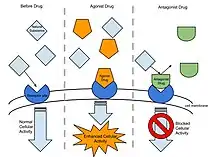
In pharmacology the term agonist-antagonist or mixed agonist/antagonist is used to refer to a drug which under some conditions behaves as an agonist (a substance that fully activates the receptor that it binds to) while under other conditions, behaves as an antagonist (a substance that binds to a receptor but does not activate and can block the activity of other agonists).
Types of mixed agonist/antagonist include receptor ligands that act as agonist for some receptor types and antagonist for others[1] or agonist in some tissues while antagonist in others (also known as selective receptor modulators).
Synaptic receptors
For synaptic receptors, an agonist is a compound that increases the activation of the receptor by binding directly to it or by increasing the amount of time neurotransmitters are in the synaptic cleft. An antagonist is a compound that has the opposite effect of an agonist. It decreases the activation of a synaptic receptor by binding and blocking neurotransmitters from binding or by decreasing the amount of time neurotransmitters are in the synaptic cleft. These actions can be achieved via multiple mechanisms. A common mechanism for agonists is reuptake inhibition, where the agonist blocks neurotransmitters from reentering the pre-synaptic axon terminal. This gives the neurotransmitter more time in the synaptic cleft to act on the synaptic receptors. Conversely, antagonists often bind directly to receptors in the synaptic cleft, effectively blocking neurotransmitters from binding.
At the alpha adrenoceptors, (R)-3-nitrobiphenyline is an α2C selective agonist as well as being a weak antagonist at the α2A and α2B subtypes.[2][3]
Agonist-antagonist opioids
The best known agonist-antagonists are opioids. Examples of such opioids are:
- pentazocine, agonist at the kappa (κ) and sigma (σ) and has a weak antagonist action at the mu opioid receptor (μ)[4]
- butorphanol, partial agonist at μ- and a pure agonist at κ-opioid receptor and antagonist activity at the delta opioid receptor (δ)[5]
- nalbuphine, κ-agonist/μ-antagonist analgesic[6]
Agonist–antagonist opioids usually have a ceiling effect – over particular dose they don't increase their potency.[7] Hence agonist–antagonist opioids have a lower addiction potential but also lower analgesic efficacy and are more likely to produce psychotomimetic effects.[8]
Agonist–antagonist opioids that block delta while activating mu opioid receptors produce analgesia without the development of tolerance.[9]
References
- Hoskin PJ, Hanks GW (March 1991). "Opioid agonist-antagonist drugs in acute and chronic pain states". Drugs. 41 (3): 326–44. doi:10.2165/00003495-199141030-00002. PMID 1711441. S2CID 27694903.
- Crassous PA, Cardinaletti C, Carrieri A, Bruni B, Di Vaira M, Gentili F, et al. (August 2007). "Alpha2-adrenoreceptors profile modulation. 3.1 (R)-(+)-m-nitrobiphenyline, a new efficient and alpha2C-subtype selective agonist". Journal of Medicinal Chemistry. 50 (16): 3964–8. doi:10.1021/jm061487a. PMID 17630725.
- Del Bello F, Mattioli L, Ghelfi F, Giannella M, Piergentili A, Quaglia W, et al. (November 2010). "Fruitful adrenergic α(2C)-agonism/α(2A)-antagonism combination to prevent and contrast morphine tolerance and dependence". Journal of Medicinal Chemistry. 53 (21): 7825–35. doi:10.1021/jm100977d. PMID 20925410.
- Hollister LE (17 July 1991). "AMA Drug Evaluations Annual 1991". JAMA: The Journal of the American Medical Association. 266 (3): 97. doi:10.1001/jama.1991.03470030126039.
- Commiskey S, Fan LW, Ho IK, Rockhold RW (June 2005). "Butorphanol: effects of a prototypical agonist-antagonist analgesic on kappa-opioid receptors". Journal of Pharmacological Sciences. 98 (2): 109–16. doi:10.1254/jphs.CRJ05001X. PMID 15942128.
- Schmidt WK, Tam SW, Shotzberger GS, Smith DH, Clark R, Vernier VG (February 1985). "Nalbuphine". Drug and Alcohol Dependence. 14 (3–4): 339–62. doi:10.1016/0376-8716(85)90066-3. PMID 2986929.
- Benson GJ, Tranquilli WJ (March 1992). "Advantages and guidelines for using opioid agonist-antagonist analgesics". The Veterinary Clinics of North America. Small Animal Practice. 22 (2): 363–5. doi:10.1016/S0195-5616(92)50637-4. PMID 1585578.
- Lasagna L (December 1987). "Benefit-risk ratio of agonist-antagonist analgesics". Drug and Alcohol Dependence. 20 (4): 385–93. doi:10.1111/j.1360-0443.1989.tb00595.x. PMID 2894291.
- Dietis N, Guerrini R, Calo G, Salvadori S, Rowbotham DJ, Lambert DG (July 2009). "Simultaneous targeting of multiple opioid receptors: a strategy to improve side-effect profile". British Journal of Anaesthesia. 103 (1): 38–49. doi:10.1093/bja/aep129. PMID 19474215.