Neglected tropical diseases in India
Neglected tropical diseases in India are a group of bacterial, parasitic, viral, and fungal infections that are common in low income countries but receive little funding to address them. Neglected tropical diseases are common in India.
India's population is about 1.3 billion as of 2018, which is the second largest in the world.[1] However, high population does not explain the greater frequently of neglected tropical diseases in India than in other countries.[1] Neglected tropical diseases in India occur in areas of both urban and rural poverty.[1]
The neglected tropical diseases which especially affect India include ascariasis, hookworm infection, trichuriasis, dengue fever, lymphatic filariasis, trachoma, melioidosis, cysticercosis, leprosy, echinococcosis, visceral leishmaniasis, and rabies.[2]
List
Various organizations will include different diseases under the umbrella term of "neglected tropical diseases," but most diseases listed as such occur in tropical climates, lack global public attention, and have high infection rates. The World Health Organization recognizes 20 neglected tropical diseases,[3] of which 12 are present in India.
- Protozoan infections
- Helminth infections
- Taeniasis/Cysticercosis
- Dracunculiasis (Guinea-worm disease)
- Echinococcosis
- Lymphatic filariasis
- Soil-transmitted helminthiases
- Viral infections
- Bacterial infections
- Leprosy (Hansen's disease)
- Trachoma
- Melioidosis
- Fungal infections
- Mycetoma, chromoblastomycosis, and other deep mycoses
- Ectoparasitic infections
- Scabies and other ectoparasites
- Others
Protozoan
Visceral leishmaniasis (kala-azar)
India has a goal for the elimination of kala-azar.[4] The steps to eliminating the disease include passive and active case detection, early diagnosis and treatment, and vector control integrated into medical treatment.[4][5]
Before the year 2000 there was hope and expectation that India could eliminate kala-azar from the country.[6] In those years there were various programs to continue usual treatments and develop new ones.[6] Around year 2000 there were reports that parasites which cause kala-azar had developed drug resistance to pentavalent antimonial, which was the popular drug for treating this disease for the last 50 years.[7][8] The disease spread to become a problem again and now more difficult to treat.[6] In poorer areas of India underreporting of the disease was a problem, allowing the disease to spread.[9] The newer treatments of that time were expensive.[10]
The treatment of kala-azar in India since about year 2000 has been difficult.[11] In 2017 the Indian government had contained kala-azar in certain regions with the goal of providing easy access to medical treatment to eliminate it from the country.[12] The intent was that by 2020 the disease should be very uncommon and also should never spread or grow again.[13] Physicians use a drug to treat kala-azar both before and after the patient seems cured, but take care to use a safe amount.[14] The work that health agencies in India have done to reduce kala-azar are learning models for India or any other country to apply to other public health programs to eliminate infectious disease.[15]
African trypanosomiasis
African trypanosomiasis (sleeping sickness) is not a problem in India.[16] Researchers do monitor watching for the disease.[16] In 2005, an Indian farmer became ill following an unusual infection with an Indian species of this parasite called Trypanosoma evansi.[17]
Chagas disease
Chagas disease is not a problem in India.[16] Chagas disease, like African trypanosomiasis, has a Trypanosoma parasite as its cause.[16][17] This parasite is not in India.[16][17]
Worms
Soil-transmitted helminthiasis
Soil-transmitted helminthiasis is a group of various parasitic diseases which different roundworms cause. The large roundworm causes Ascariasis, the hookworm causes Hookworm infection, and the whipworm causes Trichuriasis. These worms are related and there are strategies for prevention which apply to all of them.[18] The World Health Organization estimated that in 2015, 75% of the children in India who had Soil-transmitted helminthiasis also got treatment.[1][19]
Lymphatic filariasis
India has 40% of the world's lymphatic filariasis (LF) cases.[20] For the patient, one of the major costs of treating the disease is having to take a lot of time off work.[20] A year 2000 survey reported that about half of the people in India were at risk of contracting LF.[21] Men and women can get this disease equally, but in the past, there have been barriers to women accessing treatment in the normal way.[22]
In 1955 the Indian government established the National Filaria Control Programme to reduce LF.[23] In 1997 India joined a World Health Assembly resolution to eliminate LF by 2020.[23] In India to achieve this goal healthcare must be very accessible to almost everyone at risk for the disease.[24] In 2015 the Indian government launched a health campaign called Hathipaon Mukt Bharat (Filaria Free India) to encourage public participation in eliminating LF.[25]
Following some missed deadlines in 2015 and before a 2020 target date for eliminating LF, various media outlets discussed how India might meet the goal or what it should happen next if more time is required.[26][27][28]
The Ayurvedic text Sushruta Samhita described lymphatic filariasis.[23]
Echinococcosis
Echinococcosis is a parasitic disease of tapeworms.[29][30][31][32]
Cysticercosis
Taeniasis and cysticercosis are both parasitic diseases caused by tapeworms in the family Taeniidae.
Eliminated – guinea worm
Guinea-worm disease was a neglected tropical disease in India until 2000 when it was eradicated.[33] In 2006 India announced the eradication of yaws after going since 2003 with no reported cases of the disease.[34]
Foodborne trematode infection
Foodborne trematode infection is not a problem in India.
From 1969 to 2012 there have only been a few reports of a few people in India getting fasciolosis (foodborne trematode infection).[35] The disease is endemic among cows, buffalo, sheep, and goats in India.[36] A 2012 paper which reported two human infections urged for attention that human infection might be more prevalent.[37]
Onchocerciasis
Onchocerciasis (river blindness) is not a problem in India.
Onchocerciasis has been found in India in an unusual case.[38]
Schistosomiasis
Schistosomiasis is not a problem in India.
A 2015 report described that while India has no routine reports of schistosomiasis, the disease might be present and unreported.[39] A 1952 paper described the disease present in an Indian village and how WHO investigators treated the disease and tried to identify its source.[40][41] In retrospect, that older paper was unusual, and either this disease is uncommon in India or difficult to detect.[40]
Fungus
Mycetoma
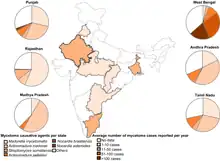
Mycetoma is an infection under the skin which in India may have either a fungus or a bacterium as cause.[42] In Rajasthan the cause is usually a fungus, but elsewhere in India a bacterium usually causes the disease.[42]
Small health surveys have shown that mycetoma is common in central India.[43]
The disease is difficult to treat.[44] The treatment for fungus will not work on the bacteria and vice versa.[44] When it is a bacterium the treatment period is long.[44]
In 1874 Henry Vandyke Carter, a British surgeon, wrote a book titled On mycetoma, or the fungus disease of India.[45]
Bacteria
Leprosy
From 1983 until 2005 India organized successful programs to eliminate leprosy as a public health problem.[46] While these programs reduced the number of people in India with leprosy from 58 in 10,000 to 1 in 10,000, they did not eliminate leprosy entirely.[46] Completely eliminating the disease is possible in the near future.[47] The National Leprosy Eradication Program is part of the government solution to ending the disease.
Without health intervention, it is possible that leprosy rates could rise and all the progress could be lost.[48]
A 2018 study reported that India does well at detecting leprosy in poor areas, but more often misses cases in places with more money.[49]
A 2019 report described how newly available technology should make detecting and treating leprosy in India more easy.[50]
Trachoma
In December 2017 the health minister of India announced that India was free of trachoma.[51][52] This announcement included a statement that there were no children in India who had an active case of trachoma.[53]
A 2011 paper had speculated that India could eliminate trachoma within 10 years.[54]
Yaws
The Indian government began programs to eliminate yaws in the 1950s.[55] India began its Yaws Eradication Program in 1996 and identified 735 cases at its start.[56] In 2004 the Indian government announced that the health program seemed to have eliminated the disease.[56] Even after yaws seemed to be gone, the government continued monitoring and searching for cases heavily through 2006.[56] Following that, there was a program to investigate rumors of yaws through 2011.[55]
In May 2016 the World Health Organization declared India free of yaws.[57] India was the first country where yaws was endemic and which eliminated it.[58] This success in India led to excite for other countries to also try to eliminate yaws by year 2020 using techniques which India developed.[59]
Buruli ulcer
Buruli ulcer is not a problem in India.
In 2019 physicians identified a case of Buruli ulcer in India, but the patient was from Nigeria where the disease is present.[60]
Viruses
Dengue fever and chikungunya fever
The WHO groups dengue and chikungunya fever together, but these are separate conditions.
India had chikungunya cases before 1973 when the disease was nearly eliminated. In 2005 India got another case of this.[61][62] Checkungunya cases are rising in India [63]
Rabies
Rabies has been a problem in India since ancient times.[64] Rabies often comes from dog bites.[64]
In India there are many stray dogs and many people report being bitten by them.[65] To determine whether someone requires treatment for rabies or only treatment for the bite, the physician should have information about the incidence of rabies in animals in the area.[66] In India about 2% of people who are bitten get a rabies vaccine.[65][67] A 2012 paper argued that there was now enough information about rabies in India to plan to contain and prevent the disease nationally.[68]
For people in India who get rabies the death rate is nearly 100%.[69]
Other
Scabies
Incidence of scabies in India ranges from 13 to 59% throughout observed areas.[70] Little research exists on how much this condition affects Indian people's work, leisure, and sleep.[70]
Various epidemiological studies exist reporting the number of people in India with scabies in various times and places.[71][72]
Topical Permethrin and oral ivermectin are commonly available in India for treatment.[73][74]
Snakebites

The envenomation is the danger of the snakebite, and not the bite itself.[75][76] The four snakes in India which account for most bites are the Indian cobra, common krait, Russell's viper, and saw-scaled viper.[77] Besides these four there are various other snakes which bite enough to require an organized medical response.[77]
In May 2018 the World Health Organization declared that responding to snake bites is a global health priority.[78]
Some places in India use traditional folk medicine with plants to treat snakebite.[79]
Designing antivenom is a challenge because different snakes require different antivenom to treat, and there are many types of snakes in India.[80]
97% of snake bites occur in rural areas.[81]
Snakes have a special place in Indian society and culture.[82] Because of this, many people who receive a snakebite treat their illness with less medical urgency than they would some other disease.[82]
A 2010 review of snake bite in India found that there is underreporting of the problem and also insufficient health care treatment available.[83]
A 1954 study tracked snake bites since 1940. This study estimated 300,000-400,000 bites a year with 10% of those being deadly.[84]
Treatment which should be available but which are sometimes hard to get includes a whole blood clotting test and a venom detection kit.[85]
Epidemiology
India and South Asia have about half of the world's cases of kala azar, lymphatic filariasis, and leprosy.[86] The region also has about a third of rabies deaths and a quarter of the South Asia, in addition to one-third of the rabies deaths, one-quarter of the intestinal helminth infections.[86] As of 2014 there was not good information about dengue and Japanese encephalitis, but these diseases are a major burden in India also.[86]
Of the 17 neglected tropical diseases which the World Health Organization recognized in 2017, six are common in India.[87] Those 6 diseases are Lymphatic filariasis, kala-azar (Visceral leishmaniasis), Leptospirosis, Rabies, Soil-transmitted helminthiasis, and Dengue fever.[87]
The Global Burden of Disease Study is a regularly updated report which attempts to describe the extent to which each major disease in the world affects individuals with those diseases.[1] This report identifies surprising problems and described them to be unknown among many health professionals.[1] One surprising finding of the 2016 Global Burden of Disease study is that India has the most and worst cases of 11 of the 16 neglected tropical diseases it considered.[1] India has the most cases of all neglected tropical diseases which occur in India.[1]
| neglected tropical disease | Cases in India | Total cases globally | India's percent of global total |
India's incidence rank |
|---|---|---|---|---|
| Ascariasis | 222 million | 799 million | 28% | 1 |
| Hookworm infection | 102 million | 451 million | 23% | 1 |
| Trichuriasis | 68 million | 435 million | 16% | 1 |
| Dengue fever* | 53 million | 101 million | 53% | 1 |
| Lymphatic filariasis | 8.7 million | 29.4 million | 29% | 1 |
| Trachoma† | 1.8 million | 3.3 million | 53% | 1 |
| Cysticercosis | 819,538 | 2.7 million | 31% | 1 |
| Leprosy | 187,730 | 523,245 | 36% | 1 |
| Echinococcosis | 119,320 | 973,662 | 12% | 1 |
| Visceral leishmaniasis | 13,530 | 30,067 | 45% | 1 |
| Rabies* | 4,370 | 13,340 | 33% | 1 |
Prevention
Elimination of as many of these diseases as possible is a goal.[90]
The government of India collaborates with the World Health Organization in making financial investments in health care for the purpose of reducing and eliminating neglected tropical diseases in India.[91]
In 2005, the Indian Health Ministry, Bangladeshi Health Ministry, and the Nepali Health Ministry shared a memorandum of understanding to eliminate kala-azar in their shared region by 2015.[92]
A 2015 study reported that India's public health programs were reducing leprosy rates but not quickly enough to eliminate the disease from the region.[93]
In 2017 the Indian government began participating in the World Health Organization's plan to eliminate 10 of the neglected tropical diseases.[87] The government strategy was to reduce poverty, promote sanitation, do vector control, and provide public health education.[87]
Society and culture
The neglected tropical diseases are diseases of poverty and poverty reduction in society will reduce them.
Some people feel embarrassed to have a disease, but a disease is not anyone's fault.[94] The government of India sometimes has organized health campaigns to teach about diseases so that people feel comfortable coming for medical help when they need it.[94]
References
- Hotez, Peter J.; Damania, Ashish; Steinmann, Peter (22 March 2018). "India's neglected tropical diseases". PLOS Neglected Tropical Diseases. 12 (3): e0006038. doi:10.1371/journal.pntd.0006038. PMC 5863936. PMID 29565970.
- Lobo, Derek A.; Velayudhan, Raman; Chatterjee, Priya; Kohli, Harajeshwar; Hotez, Peter J. (25 October 2011). "The Neglected Tropical Diseases of India and South Asia: Review of Their Prevalence, Distribution, and Control or Elimination". PLOS Neglected Tropical Diseases. 5 (10): e1222. doi:10.1371/journal.pntd.0001222. PMC 3201909. PMID 22039553.
- "Neglected tropical diseases". World Health Organization. Archived from the original on 22 February 2014. Retrieved 24 November 2015.
- Hotez, Peter J.; Pecoul, Bernard (25 May 2010). ""Manifesto" for Advancing the Control and Elimination of Neglected Tropical Diseases". PLOS Neglected Tropical Diseases. 4 (5): e718. doi:10.1371/journal.pntd.0000718. PMC 2876053. PMID 20520793.
- Joshi, A; Narain, JP; Prasittisuk, C; Bhatia, R; Hashim, G; Jorge, A; Banjara, M; Kroeger, A (June 2008). "Can visceral leishmaniasis be eliminated from Asia?". Journal of Vector Borne Diseases. 45 (2): 105–11. PMID 18592839.
- Bora, D (1999). "Epidemiology of visceral leishmaniasis in India". The National Medical Journal of India. 12 (2): 62–8. PMID 10416321.
- Sundar, Shyam (November 2001). "Drug resistance in Indian visceral leishmaniasis". Tropical Medicine and International Health. 6 (11): 849–854. doi:10.1046/j.1365-3156.2001.00778.x. PMID 11703838. S2CID 25623920.
- Sundar, Shyam; More, Deepak K.; Singh, Manoj K.; Singh, Vijay P.; Sharma, Sashi; Makharia, Anand; Kumar, Prasanna C. K.; Murray, Henry W. (October 2000). "Failure of Pentavalent Antimony in Visceral Leishmaniasis in India: Report from the Center of the Indian Epidemic". Clinical Infectious Diseases. 31 (4): 1104–1107. doi:10.1086/318121. PMID 11049798.
- Singh, S. P.; Reddy, D. C. S.; Rai, M.; Sundar, S. (June 2006). "Serious underreporting of visceral leishmaniasis through passive case reporting in Bihar, India". Tropical Medicine and International Health. 11 (6): 899–905. doi:10.1111/j.1365-3156.2006.01647.x. PMID 16772012. S2CID 23316562.
- Sundar, S; Chatterjee, M (March 2006). "Visceral leishmaniasis – current therapeutic modalities". The Indian Journal of Medical Research. 123 (3): 345–52. PMID 16778315.
- Ponte-Sucre, A; Gamarro, F; Dujardin, JC; Barrett, MP; López-Vélez, R; García-Hernández, R; Pountain, AW; Mwenechanya, R; Papadopoulou, B (December 2017). "Drug resistance and treatment failure in leishmaniasis: A 21st century challenge". PLOS Neglected Tropical Diseases. 11 (12): e0006052. doi:10.1371/journal.pntd.0006052. PMC 5730103. PMID 29240765.
- Zijlstra, EE; Alves, F; Rijal, S; Arana, B; Alvar, J (November 2017). "Post-kala-azar dermal leishmaniasis in the Indian subcontinent: A threat to the South-East Asia Region Kala-azar Elimination Programme". PLOS Neglected Tropical Diseases. 11 (11): e0005877. doi:10.1371/journal.pntd.0005877. PMC 5689828. PMID 29145397.
- Sundar, S; Singh, OP; Chakravarty, J (November 2018). "Visceral leishmaniasis elimination targets in India, strategies for preventing resurgence". Expert Review of Anti-infective Therapy. 16 (11): 805–812. doi:10.1080/14787210.2018.1532790. PMC 6345646. PMID 30289007.
- Pijpers, J; den Boer, ML; Essink, DR; Ritmeijer, K (February 2019). "The safety and efficacy of miltefosine in the long-term treatment of post-kala-azar dermal leishmaniasis in South Asia – A review and meta-analysis". PLOS Neglected Tropical Diseases. 13 (2): e0007173. doi:10.1371/journal.pntd.0007173. PMC 6386412. PMID 30742620.
- Hirve, S; Kroeger, A; Matlashewski, G; Mondal, D; Banjara, MR; Das, P; Be-Nazir, A; Arana, B; Olliaro, P (October 2017). "Towards elimination of visceral leishmaniasis in the Indian subcontinent-Translating research to practice to public health". PLOS Neglected Tropical Diseases. 11 (10): e0005889. doi:10.1371/journal.pntd.0005889. PMC 5638223. PMID 29023446.
- Joshi, Prashant P. "Human Trypanosomiasis in India: Is it an Emerging New Zoonosis?" (PDF). apiindia.org. Association of Physicians in India. pp. 10–13. Archived from the original (PDF) on 2015-03-18. Retrieved 2020-01-20.
- Joshi, PP; Shegokar, VR; Powar, RM; Herder, S; Katti, R; Salkar, HR; Dani, VS; Bhargava, A; Jannin, J; Truc, P (September 2005). "Human trypanosomiasis caused by Trypanosoma evansi in India: the first case report". The American Journal of Tropical Medicine and Hygiene. 73 (3): 491–5. doi:10.4269/ajtmh.2005.73.491. PMID 16172469.
- Abraham, Dilip; Kaliappan, SaravanakumarPuthupalayam; Walson, JuddL; Rao Ajjampur, SitaraSwarna (2018). "Intervention strategies to reduce the burden of soil-transmitted helminths in India". Indian Journal of Medical Research. 147 (6): 533–544. doi:10.4103/ijmr.IJMR_881_18. PMC 6118140. PMID 30168484.
- "PCT databank – Soil-transmitted helminthiases". WHO. Archived from the original on January 22, 2009. Retrieved 3 August 2017.
- Ramaiah, Kapa D; Das, Pradeep K; Michael, Edwin; Guyatt, Helen L (June 2000). "The Economic Burden of Lymphatic Filariasis in India". Parasitology Today. 16 (6): 251–253. doi:10.1016/S0169-4758(00)01643-4. PMID 10827432.
- Sabesan, S.; Palaniyandi, M.; Das, P. K.; Michael, E. (3 Jul 2000). "Mapping of lymphatic filariasis in India". Annals of Tropical Medicine & Parasitology. 94 (6): 591–606. doi:10.1080/00034983.2000.11813582. PMID 11064761. S2CID 35526107.
- Bandyopadhyay, Lalita (May 1996). "Lymphatic filariasis and the women of India". Social Science & Medicine. 42 (10): 1401–1410. doi:10.1016/0277-9536(95)00288-X. PMID 8735896.
- Sabesan, S; Vanamail, P; Raju, KH.K; Raju, P (2010). "Lymphatic filariasis in India: Epidemiology and control measures". Journal of Postgraduate Medicine. 56 (3): 232–8. doi:10.4103/0022-3859.68650. PMID 20739779.
- Agrawal, VK; Sashindran, VK (October 2006). "Lymphatic Filariasis in India : Problems, Challenges and New Initiatives". Medical Journal Armed Forces India. 62 (4): 359–362. doi:10.1016/S0377-1237(06)80109-7. PMC 5034168. PMID 27688542.
- Bagcchi, Sanjeet (April 2015). "India tackles lymphatic filariasis". The Lancet Infectious Diseases. 15 (4): 380. doi:10.1016/S1473-3099(15)70116-7. PMID 25809895.
- TNN (17 November 2017). "Filariasis in india: The epidemic you don't know about". The Times of India. The Times Group.
- Basu, Snigdha (8 March 2018). "Not Stigma But Awareness A Hurdle To Eliminate Lymphatic Filariasis By 2020". NDTV.
- Rath, Nibedita; Dash, Sambit (22 August 2017). "India Is Set To Fail Its Target Of Eradicating Filariasis By 2020". HuffPost India. AOL.
- Singh, BB; Dhand, NK; Ghatak, S; Gill, JP (1 January 2014). "Economic losses due to cystic echinococcosis in India: Need for urgent action to control the disease". Preventive Veterinary Medicine. 113 (1): 1–12. doi:10.1016/j.prevetmed.2013.09.007. PMID 24148988.
- Vaidya, VM; Zende, RJ; Paturkar, AM; Gatne, ML; Dighe, DG; Waghmare, RN; Moon, SL; Bhave, SS; Bengale, KG; Nikale, NV (26 June 2018). "Cystic echinococcosis in animals and humans of Maharashtra State, India". Acta Parasitologica. 63 (2): 232–243. doi:10.1515/ap-2018-0027. PMID 29654685. S2CID 4879144.
- Rawat, S; Kumar, R; Raja, J; Singh, RS; Thingnam, SKS (September 2019). "Pulmonary hydatid cyst: Review of literature". Journal of Family Medicine and Primary Care. 8 (9): 2774–2778. doi:10.4103/jfmpc.jfmpc_624_19. PMC 6820383. PMID 31681642.
- Bhutani, N; Kajal, P (December 2018). "Hepatic echinococcosis: A review". Annals of Medicine and Surgery (2012). 36: 99–105. doi:10.1016/j.amsu.2018.10.032. PMC 6226561. PMID 30450204.
- Sharma, R (11 March 2000). "India eradicates guinea worm disease". BMJ (Clinical Research Ed.). 320 (7236): 668. PMC 1117704. PMID 10710568.
- World Health Organization (14 July 2016). "India's triumph over yaws adds momentum to global eradication". who.int. Geneva: World Health Organization. Archived from the original on July 15, 2016.
- Gideon (30 December 2017). "Fascioliasis in India". Global Infectious Diseases and Epidemiology Online Network.
- Garg, Rajat; Yadav, C. L.; Kumar, R. R.; Banerjee, P. S.; Vatsya, Stuti; Godara, Rajesh (21 May 2009). "The epidemiology of fasciolosis in ruminants in different geo-climatic regions of north India". Tropical Animal Health and Production. 41 (8): 1695–1700. doi:10.1007/s11250-009-9367-y. PMID 19455400. S2CID 23875973.
- Varghese, GM; Ramachandran, J; Ajjampur, SSR; Chandramohan, A (2012). "Cases of human fascioliasis in India: Tip of the iceberg". Journal of Postgraduate Medicine. 58 (2): 150–2. doi:10.4103/0022-3859.97180. PMID 22718061.
- Barua, P; Sharma, A; Hazarika, NK; Barua, N; Bhuyan, S; Alam, ST (November 2011). "A rare case of ocular onchocerciasis in India". The Southeast Asian Journal of Tropical Medicine and Public Health. 42 (6): 1359–64. PMID 22299403.
- Kali, Arunava (2015). "Schistosome Infections: An Indian Perspective". Journal of Clinical and Diagnostic Research. 9 (2): DE01-4. doi:10.7860/JCDR/2015/10512.5521. PMC 4378741. PMID 25859459.
- Agrawal, M. C.; Rao, V. G. (2011). "Indian Schistosomes: A Need for Further Investigations". Journal of Parasitology Research. 2011: 250868. doi:10.1155/2011/250868. PMC 3205607. PMID 22132307.
- Gadgil, R. K.; Shah, S. N. (1952). "Human schistosomiasis in India". Journal of Medical Science. 6: 760–763.
- van de Sande, Wendy W. J.; Vinetz, Joseph M. (7 November 2013). "Global Burden of Human Mycetoma: A Systematic Review and Meta-analysis". PLOS Neglected Tropical Diseases. 7 (11): e2550. doi:10.1371/journal.pntd.0002550. PMC 3820768. PMID 24244780.
- Sawatkar, GiteshU; Wankhade, VaishaliH; Supekar, BhagyashreeB; Pratap, RajeshPratap; Bhat, DharitriM; Tankhiwale, SupriyaS (2019). "Mycetoma: A common yet unrecognized health burden in central India". Indian Dermatology Online Journal. 10 (3): 256–261. doi:10.4103/idoj.IDOJ_358_18. PMC 6536075. PMID 31149567.
- Relhan, V; Mahajan, K; Agarwal, P; Garg, VK (2017). "Mycetoma: An Update". Indian Journal of Dermatology. 62 (4): 332–340. doi:10.4103/ijd.IJD_476_16. PMC 5527712. PMID 28794542.
- Carter, H.Vandyke (1874). On the Nature of Mycetoma, or the Fungus Disease of India. London: J. & A. Churchill.
- Rao, PN; Suneetha, S (2018). "Current Situation of Leprosy in India and its Future Implications". Indian Dermatology Online Journal. 9 (2): 83–89. doi:10.4103/idoj.IDOJ_282_17. PMC 5885632. PMID 29644191.
- Sengupta, Utpal (2018). "Elimination of leprosy in India: An analysis". Indian Journal of Dermatology, Venereology and Leprology. 84 (2): 131–136. doi:10.4103/ijdvl.IJDVL_1070_16. PMID 29451189. S2CID 46804892.
- Cousins, S (25 August 2018). "Experts fear a resurgence of leprosy in India". Lancet. 392 (10148): 624–625. doi:10.1016/S0140-6736(18)31982-2. PMID 30152333. S2CID 52099098.
- Grantz, Kyra H.; Chabaari, Winnie; Samuel, Ramolotja Kagiso; Gershom, Buri; Blum, Laura; Worden, Lee; Ackley, Sarah; Liu, Fengchen; Lietman, Thomas M.; Galvani, Alison P.; Prajna, Lalitha; Porco, Travis C. (27 March 2018). "Spatial distribution of leprosy in India: an ecological study". Infectious Diseases of Poverty. 7 (1): 20. doi:10.1186/s40249-018-0402-y. PMC 5870368. PMID 29580296.
- Sengupta, U (2019). "Recent Laboratory Advances in Diagnostics and Monitoring Response to Treatment in Leprosy". Indian Dermatology Online Journal. 10 (2): 106–114. doi:10.4103/idoj.IDOJ_260_18. PMC 6434766. PMID 30984583.
- Sharma, Neetu Chandra (8 December 2017). "India free from Trachoma, says health minister J.P. Nadda". Livemint.
- "India now free of infective trachoma, says JP Nadda". The New Indian Express.
- Tandon, Aditi (11 December 2017). "India free from active trachoma in children". The Tribune.
- Hotez, Peter (December 2011). "Enlarging the "Audacious Goal": Elimination of the world's high prevalence neglected tropical diseases". Vaccine. 29: D104–D110. doi:10.1016/j.vaccine.2011.06.024. PMID 22188933.
- Narain, JP; Jain, SK; Bora, D; Venkatesh, S (May 2015). "Eradicating successfully yaws from India: The strategy & global lessons". The Indian Journal of Medical Research. 141 (5): 608–13. doi:10.4103/0971-5916.159542 (inactive 1 August 2023). PMC 4510759. PMID 26139778.
{{cite journal}}: CS1 maint: DOI inactive as of August 2023 (link) - Bora, D; Dhariwal, AC; Lal, S (March 2005). "Yaws and its eradication in India--a brief review". The Journal of Communicable Diseases. 37 (1): 1–11. PMID 16637394.
- World Health Organization (11 May 2016). "WHO declares India free of yaws". World Health Organization. New Delhi. Archived from the original on December 25, 2016.
- Friedrich, M.J. (20 September 2016). "WHO Declares India Free of Yaws and Maternal and Neonatal Tetanus". JAMA. 316 (11): 1141. doi:10.1001/jama.2016.12649. PMID 27654592.
- Asiedu, Kingsley; Fitzpatrick, Christopher; Jannin, Jean; Small, Pamela L. C. (25 September 2014). "Eradication of Yaws: Historical Efforts and Achieving WHO's 2020 Target". PLOS Neglected Tropical Diseases. 8 (9): e3016. doi:10.1371/journal.pntd.0003016. PMC 4177727. PMID 25254372.
- George, Ajith John; Samuel, Vimalin; Samuel, Vasanth Mark; Gaikwad, Pranay (6 June 2019). "Buruli ulcer: Rare presentation of a chronic nonhealing ulcer in India". Indian Journal of Vascular and Endovascular Surgery. 6 (2): 138–140. doi:10.4103/ijves.ijves_76_18. S2CID 184479927.
- Lahariya, C; Pradhan, SK (December 2006). "Emergence of chikungunya virus in Indian subcontinent after 32 years: A review". Journal of Vector Borne Diseases. 43 (4): 151–60. PMID 17175699.
- Muniaraj, M (March 2014). "Fading chikungunya fever from India: beginning of the end of another episode?". The Indian Journal of Medical Research. 139 (3): 468–70. PMC 4069744. PMID 24820844.
- "The resurgence of chikungunya in India". Ideas for India – Evidence based policy.
- Sudarshan, M.K.; Madhusudana, S.N.; Mahendra, B.J.; Rao, N.S.N.; Ashwath Narayana, D.H.; Abdul Rahman, S.; Meslin, F.-X.; Lobo, D.; Ravikumar, K.; Gangaboraiah (January 2007). "Assessing the burden of human rabies in India: results of a national multi-center epidemiological survey". International Journal of Infectious Diseases. 11 (1): 29–35. doi:10.1016/j.ijid.2005.10.007. PMID 16678463.
- Menezes, R. (26 February 2008). "Rabies in India". Canadian Medical Association Journal. 178 (5): 564–566. doi:10.1503/cmaj.071488. PMC 2244675. PMID 18299543.
- Ichhpujani, RL; Mala, C; Veena, M; Singh, J; Bhardwaj, M; Bhattacharya, D; Pattanaik, SK; Balakrishnan, N; Reddy, AK; Samnpath, G; Gandhi, N; Nagar, SS; Shiv, L (March 2008). "Epidemiology of animal bites and rabies cases in India. A multicentric study". The Journal of Communicable Diseases. 40 (1): 27–36. PMID 19127666.
- Sudarshan, MK; Mahendra, BJ; Madhusudana, SN; Ashwoath Narayana, DH; Rahman, A; Rao, NS; X-Meslin, F; Lobo, D; Ravikumar, K; Gangaboraiah (March 2006). "An epidemiological study of animal bites in India: results of a WHO sponsored national multi-centric rabies survey". The Journal of Communicable Diseases. 38 (1): 32–9. PMID 17370688.
- Kakkar, Manish; Venkataramanan, Vidya; Krishnan, Sampath; Chauhan, Ritu Singh; Abbas, Syed Shahid; Rupprecht, Charles E. (7 August 2012). "Moving from Rabies Research to Rabies Control: Lessons from India". PLOS Neglected Tropical Diseases. 6 (8): e1748. doi:10.1371/journal.pntd.0001748. PMC 3413711. PMID 22880139.
- Sharma, Sanchita (1 July 2018). "Vaccine-preventable rabies is India's most fatal infection". Hindustan Times.
- Nair, Pragya Ashok (2016). "A Study of Clinical Profile and Quality of Life in Patients with Scabies at a Rural Tertiary Care Centre". Journal of Clinical and Diagnostic Research. 10 (10): WC01–WC05. doi:10.7860/JCDR/2016/20938.8703. PMC 5121773. PMID 27891435.
- Gulati, P. V.; Bracanza, C.; Singh, K. P.; Borker, V. (September 1977). "Scabies in a Semiurban Area of India: An Epidemiologic Study". International Journal of Dermatology. 16 (7): 594–598. doi:10.1111/j.1365-4362.1977.tb00788.x. PMID 914413. S2CID 22089197.
- Sharma, R. S.; Mishra, R. S.; Pal, Dharam; Gupta, J. P.; Dutta, Mahendra; Datta, K. K. (15 November 2016). "An epidemiological study of scabies in a rural community in India". Annals of Tropical Medicine & Parasitology. 78 (2): 157–164. doi:10.1080/00034983.1984.11811789. PMID 6742927.
- Chandler, David J.; Fuller, Lucinda C. (2019). "A Review of Scabies: An Infestation More than Skin Deep". Dermatology. 235 (2): 79–90. doi:10.1159/000495290. PMID 30544123. S2CID 56485379.
- Sharma, R; Singal, A (2011). "Topical permethrin and oral ivermectin in the management of scabies: a prospective, randomized, double blind, controlled study". Indian Journal of Dermatology, Venereology and Leprology. 77 (5): 581–6. doi:10.4103/0378-6323.84063. PMID 21860157.
- Mohapatra, Bijayeeni; Warrell, David A.; Suraweera, Wilson; Bhatia, Prakash; Dhingra, Neeraj; Jotkar, Raju M.; Rodriguez, Peter S.; Mishra, Kaushik; Whitaker, Romulus; Jha, Prabhat; Gyapong, John Owusu (12 April 2011). "Snakebite Mortality in India: A Nationally Representative Mortality Survey". PLOS Neglected Tropical Diseases. 5 (4): e1018. doi:10.1371/journal.pntd.0001018. PMC 3075236. PMID 21532748.
- Kasturiratne, A; Wickremasinghe, AR; de Silva, N; Gunawardena, NK; Pathmeswaran, A; Premaratna, R; Savioli, L; Lalloo, DG; de Silva, HJ (4 November 2008). "The global burden of snakebite: a literature analysis and modelling based on regional estimates of envenoming and deaths". PLOS Medicine. 5 (11): e218. doi:10.1371/journal.pmed.0050218. PMC 2577696. PMID 18986210.
- Senji Laxme, R. R.; Khochare, Suyog; de Souza, Hugo Francisco; Ahuja, Bharat; Suranse, Vivek; Martin, Gerard; Whitaker, Romulus; Sunagar, Kartik; BILLIALD, Philippe (5 December 2019). "Beyond the 'big four': Venom profiling of the medically important yet neglected Indian snakes reveals disturbing antivenom deficiencies". PLOS Neglected Tropical Diseases. 13 (12): e0007899. doi:10.1371/journal.pntd.0007899. PMC 6894822. PMID 31805055.
- "Snake bites labelled a 'health priority'". BBC. 26 May 2018.
- Samy, Ramar Perumal; Thwin, Maung Maung; Gopalakrishnakone, Ponnampalam; Ignacimuthu, Savarimuthu (January 2008). "Ethnobotanical survey of folk plants for the treatment of snakebites in Southern part of Tamilnadu, India". Journal of Ethnopharmacology. 115 (2): 302–312. doi:10.1016/j.jep.2007.10.006. PMID 18055146.
- Warrell, DA; Gutiérrez, JM; Calvete, JJ; Williams, D (2013). "New approaches & technologies of venomics to meet the challenge of human envenoming by snakebites in India". The Indian Journal of Medical Research. 138 (1): 38–59. PMC 3767246. PMID 24056555.
- Ray, Kalyan (23 January 2019). "India neglects snakebites despite 50K deaths each year". Deccan Herald.
- Roopa, Nupur (27 October 2017). "Venom, myth and medicine: India fights its reputation as world snakebite capital | Nupur Roopa". The Guardian.
- Alirol, Emilie; Sharma, Sanjib Kumar; Bawaskar, Himmatrao Saluba; Kuch, Ulrich; Chappuis, François; de Silva, Janaka (26 January 2010). "Snake Bite in South Asia: A Review". PLOS Neglected Tropical Diseases. 4 (1): e603. doi:10.1371/journal.pntd.0000603. PMC 2811174. PMID 20126271.
- AHUJA, ML; SINGH, G (October 1954). "Snake bite in India". The Indian Journal of Medical Research. 42 (4): 661–86. PMID 13232717.
- Abraham, Siju V. (2018). "Snake bite in India: A few matters to note". Toxicology Reports. 5: 839. doi:10.1016/j.toxrep.2018.08.010. PMC 6104458. PMID 30140616.
- Hotez, Peter J. (29 May 2014). "Ten Global "Hotspots" for the Neglected Tropical Diseases". PLOS Neglected Tropical Diseases. 8 (5): e2496. doi:10.1371/journal.pntd.0002496. PMC 4038631. PMID 24873825.
- Acharya, Anita Shankar; Kaur, Ravneet; Goel, Akhil Dhanesh (July 2017). "Neglected tropical diseases—Challenges and opportunities in India". Indian Journal of Medical Specialities. 8 (3): 102–108. doi:10.1016/j.injms.2017.07.006.
- all numbers are from the Institute for Health Metrics and Evaluation's 2016 Global Burden of Disease Study
- Institute for Health Metrics and Evaluation (2017). "Global Burden of Disease Study 2016 (GBD 2016) Data Resources". ghdx.healthdata.org. University of Washington.
- Dash, A.P.; Revankar, C. (June 2012). "Neglected tropical diseases targeted for elimination in South-East Asia – Progress so far". International Journal of Infectious Diseases. 16: e18. doi:10.1016/j.ijid.2012.05.048.
- World Health Organization (2015). Investing to overcome the global impact of neglected tropical diseases: third WHO report on neglected tropical diseases. Geneva: World Health Organization. ISBN 978-92-4-156486-1.
- Narain, Jai P; Dash, AP; Parnell, B; Bhattacharya, SK; Barua, S; Bhatia, R; Savioli, L (1 March 2010). "Elimination of neglected tropical diseases in the South-East Asia Region of the World Health Organization". Bulletin of the World Health Organization. 88 (3): 206–210. doi:10.2471/BLT.09.072322. PMC 2828791. PMID 20428388.
- Brook, Cara E.; Beauclair, Roxanne; Ngwenya, Olina; Worden, Lee; Ndeffo-Mbah, Martial; Lietman, Thomas M.; Satpathy, Sudhir K.; Galvani, Alison P.; Porco, Travis C. (22 October 2015). "Spatial heterogeneity in projected leprosy trends in India". Parasites & Vectors. 8 (1): 542. doi:10.1186/s13071-015-1124-7. PMC 4618538. PMID 26490137.
- Weiss, Mitchell G.; Utzinger, Juerg (14 May 2008). "Stigma and the Social Burden of Neglected Tropical Diseases". PLOS Neglected Tropical Diseases. 2 (5): e237. doi:10.1371/journal.pntd.0000237. PMC 2359851. PMID 18478049.
Further reading
- International Federation of Pharmaceutical Manufacturers & Associations; Global Health Progress; Organisation of Pharmaceutical Producers of India (2013), Action on Neglected Tropical Diseases in India (PDF), India: Global Health Progress