Nicotine marketing
Nicotine marketing is the marketing of nicotine-containing products or use. Traditionally, the tobacco industry markets cigarette smoking, but it is increasingly marketing other products, such as electronic cigarettes and heated tobacco products. Products are marketed through social media, stealth marketing, mass media, and sponsorship (particularly of sporting events). Expenditures on nicotine marketing are in the tens of billions a year; in the US alone, spending was over US$1 million per hour in 2016;[1] in 2003, per-capita marketing spending was $290 per adult smoker, or $45 per inhabitant. Nicotine marketing is increasingly regulated; some forms of nicotine advertising are banned in many countries. The World Health Organization recommends a complete tobacco advertising ban.[2]
| Part of a series on |
| Tobacco |
|---|
 |
| History |
| Chemistry |
| Biology |
| Personal and social effects |
| Production |
Effects


The effectiveness of tobacco marketing in increasing consumption of tobacco products is widely documented.[3] Advertisements cause new people to become addicted, mostly when they are minors.[4][5][6][3] Ads also keep established smokers from quitting. Advertising peaks in January, when the most people are trying to quit, although the most people take up smoking in the summer.[3]: 61
.jpg.webp)
The tobacco industry has frequently claimed that ads are only about "brand preference", encouraging existing smokers to switch to and stick to their brand.[7] There is, however, substantial evidence that ads cause people to become, and stay, addicted.[7]
Marketing is also used to oppose regulation of nicotine marketing and other tobacco control measures, both directly and indirectly, for instance by improving the image of the nicotine industry and reducing criticism from youth and community groups. Industry charity and sports sponsorships are publicized (with publicity costing up to ten times the cost of the publicized act), portraying the industry as actively sharing the values of the target audience. Marketing is also used to normalize the industry ("Just Another Fortune 500 Company", "More Than a Tobacco Company").[3]: 198–201 Finally, marketing is used to give the impression that nicotine companies are responsible, "Open and Honest". This is done through an emphasis on informed choice and "anti-teen-smoking" campaigns,[3]: 198–201 although such ads have been criticized as counterproductive (causing more smoking) by independent groups.[3]: 190–196 [8]
Magazines, but not newspapers, that get revenue from nicotine advertising are less likely to run stories critical of nicotine products. Internal documents also show that the industry used its influence with the media to shape coverage of news, such as a decision not to mandate health warnings on cigarette packages or a debate over advertising restrictions.[3]: 345–350
Counter-marketing is also used, mostly by public health groups and governments. The addictiveness and health effects of nicotine use are generally described, as these are the themes missing from pro-tobacco marketing.[3]: 150
According to a 2019 study, television advertisement for tobacco "increased the share of smokers in the population by 5–15 percentage points, generating roughly 11 million additional smokers between 1946 and 1970."[9]
Regulation and evasion techniques

Because it harms public health, nicotine marketing is increasingly regulated.
Advertising restrictions typically shift marketing spending to unrestricted media. Banned on television, ads move to print; banned in all conventional media, ads shift to sponsorships; banned as in-store advertising and packaging, advertising shifts to shill (undisclosed) marketing reps, sponsored online content, viral marketing, and other stealth marketing techniques.[3]: 272–280 Unlike conventional advertising, stealth marketing is not openly attributed to the organization behind it. This neutralizes mistrust of tobacco companies, which is widespread among children and the teenagers who provide the industry with most new addicts.[3]: Ch.6&7
Another method of evading restrictions is to sell less-regulated nicotine products instead of the ones for which advertising is more regulated. For instance, while TV ads of cigarettes are banned in the United States, similar TV ads of e-cigarettes are not.[10]
The most effective media are usually banned first, meaning advertisers need to spend more money to addict the same number of people.[3]: 272 Comprehensive bans can make it impossible to effectively substitute other forms of advertising, leading to actual falls in consumption.[3]: 272–280 However, skillful use of allowed media can increase advertising exposure; the exposure of U.S. children to nicotine advertising is increasing as of 2018.[10]
Methods
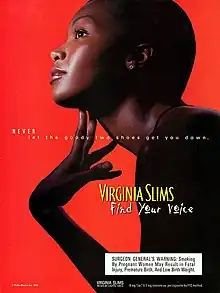
Nicotine advertising uses specific techniques, but often uses multiple methods simultaneously. For instance, the ad illustrated in this section uses many of the techniques discussed below. Its tagline reads "NEVER let the goody two shoes get you down",[11] making use of reactance; it has also been described as urging smokers to disregard health warnings.[12] The model's gesture echoes earlier ads which made more explicit claims of voice box benefits.[13][14] The 1999-2000 "Find your voice" ad campaign, of which this ad was a part, was criticized as offensive to smokers who have lost their voices to throat cancer,[12][15] and as targeting minority women and seeking to associate itself with empowerment, independence, self-expression, women's rights, and sexual allure.[16][17][12][18]

Rebellion
Nicotine marketing makes extensive use of reactance, the feeling that one is being unreasonably controlled. Reactance often motivates rebellion, in behavior or belief, which demonstrates that the control was ineffective, restoring the feeling of freedom.[19]
Ads thus rarely explicitly tell the viewer to use nicotine; this has been shown to be counter-productive. Instead, they frequently suggest using nicotine as a way to rebel and be free.[19] This marketing message is at odds with the feelings of smokers, who commonly feel trapped by their addiction and unable to quit.[20] Mention of addiction is avoided in nicotine advertising.[21]: 150
Reactance can be eliminated by successfully concealing attempts to manipulate or control behavior. Unlike conventional advertising, stealth marketing is not openly attributed to the organization behind it. This neutralizes mistrust of tobacco companies, which is widespread among children and the teenagers who provide the industry with most new addicts.[3]: Ch.6&7 The internet and social media are particularly suited to stealth and viral marketing, which is also cheap;[22] nicotine companies now spend tens of millions per year on online marketing.[23]
Counter-advertising also shows awareness of reactance; it rarely tells the viewer what to do. More commonly, it cites statistics about addictiveness and other health effects. Some anti-smoking ads dramatise the statistics (e.g. by piling 1200 body bags in front of the New York headquarters of Philip Morris, now Altria, to illustrate the number of people dying daily from smoking);[24] others document individual experiences.[25] Providing information does not generally provoke reactance.
Social conformity

Despite products being marketed as individualistic and non-conformist, people generally actually start using due to peer pressure. Being offered a cigarette is one of the largest risk factors for smoking.[3]: 256–257 Boys with a high degree of social conformity are also more likely to start smoking.[3]: 216
Social pressure is deliberately used in marketing, often using stealth marketing techniques to avoid triggering reactance. "Roachers", selected for good looks, style, charm,[3]: 110 and being slightly older than the targets,[26] are hired to offer samples of the product.[3]: 110 "Hipsters" are also recruited clandestinely from the bar and nightclub scene to sell cigarettes, and ads are placed in alternative media publications with "hip credibility".[3]: 108–110 Other strategies include sponsoring bands and seeking to give an impression of usage by scattering empty cigarette packages.[27]
Ads also use the threat of social isolation, implied or explicit (e.g. "Nobody likes a quitter").[28] Great care is taken to maintain the impression that a brand is popular and growing in popularity, and that people who smoke the brand are popular[3]: 217

Marketing seeks to create a desirable identity as a user, or a user of a specific brand. It seeks to associate nicotine use with rising social identities (see, for instance, the illustrating ad, and history of nicotine marketing in the woman's and civil rights movements, and its use of western affluence in the developing world, below). It seeks to associate nicotine use with positive traits, such as intelligence, fun, sexiness, sociability, high social status, wealth, health, athleticism, and pleasant outdoor pursuits. Many of these associations are fairly implausible; smoking is not generally considered an intelligent choice, even by smokers; most smokers feel miserable about smoking,[20] smoking causes impotence,[29][30][31] many smokers feel socially stigmatized for smoking,[20] and smoking is expensive and unhealthy.
Marketing also uses associations with loyalty, which not only defend a brand, but put a positive spin on not quitting. A successful campaign playing on loyalty and identity was the "rather fight than switch" campaign, in which the makeup the models wore made it seem as if they had black eyes, by implication from a fight with smokers of other cigarettes (campaign by a subsidiary of American Tobacco Company, now owned by British American Tobacco).[32]
Mood changes
Nicotine is also advertised as good for "nerves", irritability, and stress. Again, ads have moved from explicit claims ("Never gets on your nerves") to implicit claims ("Slow down. Pleasure up"). Although nicotine products temporarily relieve nicotine withdrawal symptoms, an addiction causes worse stress and mood, due to mild withdrawal symptoms between hits. Nicotine addicts need the nicotine to temporarily feel normal.[33][34] Nicotine addiction seems to worsen mental health problems,[33] but industry marketing has claimed that nicotine is both less harmful and therapeutic for people with mental illness, and is a form of "self-medication". Marketing has also claimed that quitting will worsen rather than improve mental health symptoms. These claims have been criticized by independent researchers as inaccurate.[35]
It is thought that nicotine withdrawal is worse for those who are already stressed or depressed, making quitting more difficult.[33][34] About 40% of the cigarettes sold in the U.S. are smoked by people with mental health issues. Smoking rates in the U.S. military were also high, and over a third started smoking after entering the military; deployment was also a risk factor.[36] Disabled people are more likely to smoke; smoking causes disability, but the stress of disability might also cause smoking.[37]
According to the CDC Tobacco Product Use Among Adults 2015 report, people who are American Indian/Alaska Native, non-Hispanic, less-educated (0–12 years education; no diploma, or General Educational Development), lower-income (annual household income <$35,000), the uninsured, and those under serious psychological distress have the highest reported percentage of any tobacco product use.[38]
"Clearly, the sole reason for B&W's interest in the black and Hispanic communities is the actual and potential sales of B&W products within these communities and the profitability of those sales...."
Brown & Williamson, a now-defunct subsidiary of British American Tobacco (7 September 1984). Total minority marketing plan (Report)., also cited in[39]
Poorer people also smoke more. When marketing cigarettes to the developing world, tobacco companies associate their product with an affluent Western lifestyle.[40] However, in the developed world, smoking has almost vanished among the affluent. Smoking rates among the American poor are much higher than among the rich, with rates of over 40% for those with a high school equivalency diploma.[41] These differences have been attributed to both lack of healthcare and to selective marketing to socio-economic, racial, and sexual minorities.[41][42] The tobacco industry targeted young rural men by creating advertisements with images of cowboys, hunters, and race car drivers. Teens in rural areas are less likely to be exposed to anti-tobacco messages in the media. Low-income and predominantly minority neighborhoods often have more tobacco retailers and more tobacco advertising than other neighborhoods.[43]
The tobacco industry focusses marketing towards vulnerable groups, contributing to the large disparity in smoking and health problems.[44] The tobacco industry has marketed heavily to African Americans,[39] sexual minorities,[45] and even the homeless and the mentally ill.[46] In 1995, Project SCUM, which targeted sexual and racial minorities and homeless people in San Francisco, was planned by R. J. Reynolds Tobacco Company (a British American Tobacco subsidiary).[47][48]
Tobacco companies have often been progressive in their hiring policies, employing women and people of colour when this was controversial. They also donate some of their profits to a variety of organizations that help people in need.[49][39]
Non-addictiveness and healthiness

Reference to the addictiveness of nicotine is avoided in marketing.[21]: 150 Indeed, the addictiveness of nicotine was explicitly denied into the nineties;[50] in 1994, seven tobacco executives stated that nicotine was not addictive while on oath before the US Congress.[51][50] Industry feared that, if continuing to smoke was not seen as a "free choice", they would be exposed to legal and social liabilities.[50]
The nicotine industry frequently markets its products as healthy, safe, and harmless; it has even marketed them as beneficial to health. These marketing messages were initially explicit, but over the decades, they became more implicit and indirect. Explicitly claiming something that the consumer knows to be untrue tend to make them distrust and reject the message, so the effectiveness of explicit claims dropped as evidence of the harms of cigarettes became more widely known. Explicit claims also have the disadvantage that they remind smokers of the health harms of the product.[21]: 63
Implicit claims include slogans with connotations of health and vitality, such as "Alive with pleasure", and imagery (of instance, images of athletic, healthy people, the presence of healthy children, healthy natural environments, and medical settings).[21]: 62–65 [3]
"Modified risk" products
"Modified risk" nicotine products, alternate nicotine products that are implied to be less harmful, are an old strategy.[52][53] These products are used to discourage quitting, by offering unwilling smokers an alternative to quitting, and implying that using the alternate product will reduce the hazards of smoking.[21]: 62–65 [3] "Modified risk" products also attract new smokers.[52]
Many "modified risk" nicotine products are actually just as risky as the products they were marketed against.[21]: 25–27 [54][55] As the long-term harms of cigarette smoking emerge after ~20 years of use, claims of reduced long-term harms for a new product cannot immediately be refuted.[56] Products may become popular on the basis of false health claims before the research is done that proves them false.[56]
Explicit claims of health benefits carry legal risks. They may also require regulatory pre-approval.[53] Reduced levels of specific harmful chemicals are often advertised; people tend to wrongly interpret these as claims of reduced harm.[53] To imply that some nicotine products are healthier than others without making explicit claims, marketing has used descriptions like "light", "mild", "natural", "gentle", "calm", "soft", and "smooth".[21]: 62–65 [3]
Both adults and youth have been shown to misinterpret marketing claims about changes in risk. They falsely interpret them as meaning that the product is safe. They are more likely to start using it, and less likely to quit, as a result.[57]
"Mild" and "roasted" cigarettes
In the 1920s to 1950s, ads often focused on throat irritation and coughs, claiming that specific brands were better. This also distracted from the more serious harms of smoking,[58] which were being revealed by research at the time.[59] Claims were made that toasting tobacco removed irritants (which were said to have been sold on to chemical companies).[58]
Menthol cigarettes
Menthol cigarettes have also been marketed as healthier from the 1930s onwards. They were even inaccurately advertised as medicinal, a treatment for smokers that would sooth a throat irritated by smoking, or as a treatment for a cold. Where this is illegal, they are marketed as healthier by implication, using words like "mild", "natural", "gentle", "calm", "soft", "smooth", and imagery of healthy natural environments.[21]: 62–65 There is no evidence that menthol cigarettes are healthier, but there is evidence that they are somewhat easier to become addicted to and harder to quit.[21]: 25–27
Reaching the Black market in the United States
Historian Keith Wailoo argues the cigarette industry targeted a new market in the black audience starting in the 1960s. It took advantage of several converging trends. First was the increased national attention on the dangers of lung cancer. Cigarette companies took the initiative in fighting back. they developed menthol-flavored brands like Kool, which seemed to be more soothing to the throat, and advertised these as good for your health. A second trend was the Federal ban on tobacco advertising on radio and television. There was no ban on advertising in the print media, so the industry responded by large scale advertising in Black newspapers and magazines. They erecting billboards in inner city neighborhoods. The third trend was the Civil rights movement of the 1960s. Big Tobacco responded by investing heavily in the Civil Rights Movement, winning the gratitude of many national and local leaders. Menthol flavored cigarette brands systematically sponsored local events in the black community, and subsidized major black organizations especially the NAACP (National Association for the Advancement of Colored People). They also subsidized many churches and schools. The marketing initiative was a success as the rate of smoking in the black community grew, while it declined among whites, Furthermore three or four black smokers purchased menthol cigarettes.[60]
Filter cigarettes
In the fifties, filters were added to cigarettes, and heavily marketed, until they faced regulatory action as false advertising.[58] Initially, efforts were made to develop filters that actually reduced harms; as it became obvious that this was not economically possible, filters were instead designed to turn brown with use.[61][54]
Ventilated ("light") cigarettes
Ventilated cigarettes (marketed as "light", "low-tar", "low-nicotine" etc.) do feel cooler, airier, and less harsh, and a smoking machine will give lower tar and nicotine readings for them. But they do not actually reduce human intake or health risks, as a human responds to the lower resistance to breathing through them by taking bigger puffs.[62] They were also designed to be equally addictive, as manufacturers did not want to lose customers.[55] They were introduced in the 1970s, responding to regulation requiring that nicotine and tar yields be included in cigarette ads. Light cigarettes became so popular that, as of 2004, half of American smokers preferred them over regular cigarettes,[63] According to the US federal government's National Cancer Institute (NCI), light cigarettes provide no benefit to smokers' health.[64][65] However, people using "light" cigarettes are less likely to quit.[66]
Heated tobacco products
Heated tobacco products, presented as heat-not-burn products, are marketed as less harmful than regular cigarettes since 1988.[67] There is no reliable evidence that these products are any less harmful than regular cigarettes.[68] A reduced harm from using these products has not been proven.[69] These products are marketed as a "smoke-free" alternative to regular cigarettes.[70] These products do generate smoke.[69] Companies are using similar strategies and channels as previously used for traditional cigarettes.[71]
Electronic cigarettes
A 2014 review said, "the e-cigarette companies have been rapidly expanding using aggressive marketing messages similar to those used to promote cigarettes in the 1950s and 1960s."[72] Unsupported claims on safety and quitting smoking are made.[73]: p.9 Common marketing messages on brand websites, claiming that e-cigarettes are safe and healthy, have been described as "concerning".[74] It is commonly claimed that e-cigarettes emit merely "harmless water vapor", which is not the case.[72] E-cigarette e-liquids marketed as "nicotine-free" have been found to contain nicotine.[75]
Targets
"[A]dvertising for low delivery or traditional brands should be constructed in ways so as not to provoke anxiety about health, but to alleviate it, and enable the smoker to feel assured about the habit and confident in maintaining it over time."
Unwilling smokers: customer retention
On average, smokers start as adolescents and make over 30 quit attempts, at a rate of about 1 per year, before breaking a nicotine addiction in their 40s or 50s.[76] Most say they feel addicted, and feel misery and disgust at their inability to quit (in surveys, 71–91% regret having started, over 80% intend to quit, around 15% plan to quit within the next month).[20] The industry calls this group "concerned smokers" and seeks to retain them as customers.[7] Techniques for lowering their quit rate include dissuading them from wanting to quit and offering them meaningless product choices which help them feel in control of their habit. For instance, downplaying the risks, and encouraging them to take pride in smoking as an identity, reduces desire to quit.
Suggesting that addicts can reduce their risk by choosing to switch to another product (branded to suggest that it is less harmful or addictive) can reduce their cognitive dissonance[21]: 63 and sense of lack of control, without offering a health improvement.[77][78][62][21]: 62–65 Switching to a product branded to suggest that it is less harmful or addictive ("mild", "light", "low-tar", "filtered" etc.) is, in terms of health effects, meaningless.[79][77][78][62]
Youth: new customers
_2.jpg.webp)
The intended audience of tobacco advertising has changed throughout the years, with some brands specifically targeted towards a particular demographic. According to Reynolds American Inc, the Joe Camel campaign in the United States was created to advertise Camel brand to young adult smokers. Class action plaintiffs and politicians described the Joe Camel images as a "cartoon" intended to advertise the product to people below the legal smoking age. Under pressure from various anti-smoking groups, the Federal Trade Commission, and the U.S. Congress, Camel ended the campaign on 10 July 1997.
Vending machines, individually sold single cigarettes, and product displays near schools, next to candy and sweet drinks, and at the eye-level of young children are all used around the world to sell nicotine-containing products. Even large brands are frequently advertised in ways that break local regulations.[81][82] In many countries, such marketing methods are not illegal. Where they are illegal, enforcement is often a problem. For instance, Dr. Suresh Kumar Arora, New Delhi's chief tobacco control officer, said: "We were wasting our time fining cigarette vendors and distributors. They had no idea of the law. Most are illiterate. Our teams would tear down posters and in no time, they would be up again because the real culprits were the big tobacco companies – ITC, Philip Morris (now Altria), Godfrey Phillip. I told them to stop giving posters to their dealers otherwise I would drag them through the courts. Since last May, Delhi has been free of tobacco posters, 100% free". He has, however, been unable to keep mobile vendors from illegally selling cigarettes next to schools.[81]
Easily circumvented age verification at company websites enables minors to access and be exposed to marketing for e-cigarettes.[83] Tobacco businesses intensely market e-cigarettes to youth[84] using cartoon characters and candy flavors.[85] E-cigarettes are also marketed on Facebook, where age restrictions are in many cases not implemented.[86]
"Harm reduction" advertising
Some tobacco companies have sponsored ads that claim to discourage teen smoking. Such ads are unregulated. However, these ads have been shown, in independent studies, to increase the self-reported likelihood that teens will start smoking. They also cause adults to see tobacco companies as more responsible and less in need of regulation. Unlike promotional ads, tobacco companies do not track the effects of these ads themselves. These ads differ from independently produced antismoking ads in that they do not mention the health effects of smoking, and present smoking as exclusively an "adult choice", undesirable "if you're a teen".[3]: 190–196 There is more exposure to industry-sponsored "antismoking" ads than to antismoking ads run by public health agencies.[3]: 189
Tobacco companies have also funded "anti-smoking" groups. One such organization, funded by Lorillard, entered into exclusive sponsorship agreements with sports organizations. This means that no other anti-smoking campaigns are allowed to be involved with the sporting organization. Such sponsorships have been criticized by health groups.[8]
Recapturing former smokers
Companies have also sought to recapture people who have successfully broken a nicotine dependency. Ex-smokers tend to view these attempts very negatively, and their existence has frequently been denied. Methods discussed in industry documents include price drops, increasing acceptance of smoking by nonsmokers, making products more socially acceptable, and making "healthier" cigarettes (scare quotes in original).[66]
Economics
As tobacco companies keep spending money on marketing until it stops being profitable, marginal changes in marketing typically have no measurable effect, but the total amount of marketing has a strong effect.[3]: 276
Econometric studies have been done into the endogeneity[87] and other aspects of bans.[88][89]
Budgets
Tobacco companies have had particularly large budgets for their advertising campaigns. The Federal Trade Commission claimed that cigarette manufacturers spent $8.24 billion on advertising and promotion in 1999, the highest amount ever at that time. The FTC later claimed that in 2005, cigarette companies spent $13.11 billion on advertising and promotion, down from $15.12 billion in 2003, but nearly double what was spent in 1998. The increase, despite restrictions on the advertising in most countries, was an attempt at appealing to a younger audience, including multi-purchase offers and giveaways such as hats and lighters, along with the more traditional store and magazine advertising.[90]
Marketing consultants ACNielsen announced that, during the period September 2001 to August 2002, tobacco companies advertising in the UK spent £25 million, excluding sponsorship and indirect advertising, broken down as follows:
- £11 million on press advertising
- £13.2 million on billboards
- £714,550 on radio advertising
- £106,253 on direct mail advertising
Figures from around that time also estimated that the companies spent £8m a year sponsoring sporting events and teams (excluding Formula One) and a further £70m on Formula One in the UK.[91]
The £25 million spent in the UK amounted to approximately US$0.60 per person in 2002. The 15.12 billion spent in the United States in 2003 amounted to more than $45 for every person in the United States, more than $36 million per day, and more than $290 for each U.S. adult smoker.
Television and radio e-cigarette advertising in some countries may be indirectly advertising traditional cigarette smoking.[72] A 2014 review said, "the e-cigarette companies have been rapidly expanding using aggressive marketing messages similar to those used to promote cigarettes in the 1950s and 1960s."[72] In the US, six large e-cigarette businesses spent $59.3 million on promoting e-cigarettes in 2013.[92] E-cigarettes are increasingly sold by the traditional tobacco multinationals.[93]
Gallery
.jpg.webp)
.jpg.webp) An 1897 newspaper display ad emphasizes the product's "genuine" nature
An 1897 newspaper display ad emphasizes the product's "genuine" nature 1900 cigarette ad targeting women
1900 cigarette ad targeting women Hans Rudi Erdt: Problem Cigarettes, 1912
Hans Rudi Erdt: Problem Cigarettes, 1912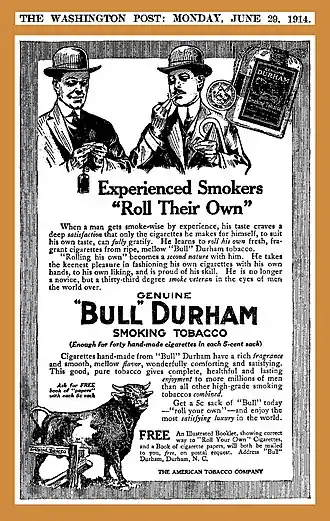 This 1914 display ad appealed to the experienced smoker—the "thirty-third degree smoke veteran"—touting the "satisfaction" derived only from making one's own cigarettes, calling the product "good, pure" tobacco that gives "complete, healthful and lasting enjoyment".
This 1914 display ad appealed to the experienced smoker—the "thirty-third degree smoke veteran"—touting the "satisfaction" derived only from making one's own cigarettes, calling the product "good, pure" tobacco that gives "complete, healthful and lasting enjoyment".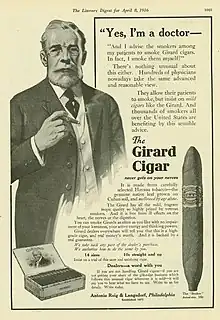 A 1916 ad showing a fictional doctor endorsing a cigar brand. At the time, it was considered a breach of medical ethics to advertise; doctors who did so would risk losing their license.[94]
A 1916 ad showing a fictional doctor endorsing a cigar brand. At the time, it was considered a breach of medical ethics to advertise; doctors who did so would risk losing their license.[94]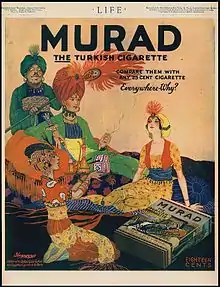 Advertisement for "Murad" Turkish cigarettes 1918
Advertisement for "Murad" Turkish cigarettes 1918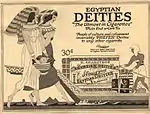 Advertisement for "Egyptian Deities" cigarettes 1919
Advertisement for "Egyptian Deities" cigarettes 1919 A 1921 cigar ad claiming that a fictional doctor called this brand "harmless" and "never gets on your nerves" (a term then used for nicotine withdrawal symptoms)
A 1921 cigar ad claiming that a fictional doctor called this brand "harmless" and "never gets on your nerves" (a term then used for nicotine withdrawal symptoms)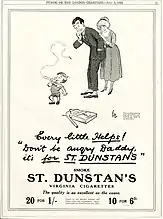 In a 1922 ad, a small child, smoking a cigarette, tells his amused parents not to worry, as he is smoking for a veteran's charity. Children were often used in early cigarette ads, where they helped normalize smoking as part of family living, and gave associations of purity, vibrancy, and life.[95]
In a 1922 ad, a small child, smoking a cigarette, tells his amused parents not to worry, as he is smoking for a veteran's charity. Children were often used in early cigarette ads, where they helped normalize smoking as part of family living, and gave associations of purity, vibrancy, and life.[95] "We claim no curative powers for Phillip Morris" says this 1943 ad featuring actor Johnny Roventini, in the small text.
"We claim no curative powers for Phillip Morris" says this 1943 ad featuring actor Johnny Roventini, in the small text. This WWII ad shows a woman sending her soldier husband a carton of cigarettes, and urges others to do the same. In an echo of the claim that doctors prefer the brand, it claims that men in the military prefer it, too. A mention of War Stamps associates the brand still more closely to war patriotism.
This WWII ad shows a woman sending her soldier husband a carton of cigarettes, and urges others to do the same. In an echo of the claim that doctors prefer the brand, it claims that men in the military prefer it, too. A mention of War Stamps associates the brand still more closely to war patriotism. Women in the War cigarette ad showing a woman signalling civilian aircraft. The ad associates taking a "man's job" and smoking cigarettes like a man: "Co-ed leaves Campus to fill a Man's job. She's "in the service" -- even to her choice of cigarettes..."
Women in the War cigarette ad showing a woman signalling civilian aircraft. The ad associates taking a "man's job" and smoking cigarettes like a man: "Co-ed leaves Campus to fill a Man's job. She's "in the service" -- even to her choice of cigarettes..." French Painted Mural Advertisement
French Painted Mural Advertisement Tobacco display in a store Munich in 2008
Tobacco display in a store Munich in 2008
See also
- Advertising to children
- Cigarette packets in Australia
- Circuit de Spa-Francorchamps
- Foundation for a Smoke-Free World
- Framework Convention on Tobacco Control
- History of nicotine marketing
- Philip Morris v. Uruguay
- Plain tobacco packaging
- Smoking ban
- Tobacco marketing and African Americans
- Tobacco packaging warning messages
- Tobacco usage in sport
- Torches of Freedom
- Jeff Wigand – former tobacco company executive and whistleblower
References
- "Economic Trends in Tobacco: Tobacco-Related Spending". Centers for Disease Control and Prevention. 4 May 2018.
- WHO Report on the Global Tobacco Epidemic, 2008: The MPOWER Package. Geneva, Switzerland: World Health Organization. 2008. p. 38. ISBN 978-92-4-159628-2. Archived from the original on 17 February 2010.
- Davis RM, Gilpin EA, Loken B, Viswanath K, Wakefield MA (2008). The role of the media in promoting and reducing tobacco use (PDF). National Cancer Institute tobacco control monograph series. U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute. p. 684.
- Biener, L.; Siegel, M. (2000). "Tobacco marketing and adolescent smoking: More support for a causal inference". American Journal of Public Health. 90 (3): 407–411. doi:10.2105/AJPH.90.3.407. PMC 1446173. PMID 10705860.
- Choi WS, Ahluwalia JS, Harris KJ, Okuyemi K (May 2002). "Progression to established smoking: the influence of tobacco marketing". American Journal of Preventive Medicine. 22 (4): 228–33. doi:10.1016/S0749-3797(02)00420-8. PMID 11988378.
- Saffer H, Chaloupka F (November 2000). "The effect of tobacco advertising bans on tobacco consumption". Journal of Health Economics. 19 (6): 1117–37. CiteSeerX 10.1.1.468.6530. doi:10.1016/S0167-6296(00)00054-0. PMID 11186847.
- Pollay RW (June 2000). "Targeting youth and concerned smokers: evidence from Canadian tobacco industry documents". Tobacco Control. 9 (2): 136–47. doi:10.1136/tc.9.2.136. PMC 1748318. PMID 10841849.
- "Letter to NBA Commissioner" (PDF). Campaign for Tobacco-Free Kids. 19 July 2002.
- Thomas, Michael (4 June 2019). "Was Television Responsible for a New Generation of Smokers?". Journal of Consumer Research. 46 (4): 689–707. doi:10.1093/jcr/ucz024. hdl:10.1093/jcr/ucz024. ISSN 0093-5301.
- Rapaport L (6 April 2018). "More U.S. teens seeing e-cigarette ads". Business Insider. Archived from the original on 5 July 2018. Retrieved 18 May 2018.
- 1999 advertisement, in the collection of Stanford Research Into the Impact of Tobacco Advertising Archived 6 September 2018 at the Wayback Machine
- "Philip Morris Removes Slogan From Ads in Second Attempt Responding to Critics - WSJ". Wall Street Journal. 13 June 2000. Retrieved 10 July 2018.
- Pages, The Society. "Cigarette Ads: Then and Now - Sociological Images". Retrieved 27 June 2018.
- Classic vs. modern Archived 26 February 2021 at the Wayback Machine ad comparison, Stanford Research into the Impact of Tobacco Advertising ad database.
- Sakai K, Kojima A, Hisanaga N, Shibata E, Huang J, Ono Y, Takeuchi Y, Aoki T, Takagi H, Ando T (September 1991). "[Asbestos concentration and fiber size in lungs of the urban residents]". [Nihon Koshu Eisei Zasshi] Japanese Journal of Public Health. 38 (9): 762–70. doi:10.1136/tc.10.2.91. PMC 1747554. PMID 1747554.
- Toll BA, Ling PM (June 2005). "The Virginia Slims identity crisis: an inside look at tobacco industry marketing to women". Tobacco Control. 14 (3): 172–80. doi:10.1136/tc.2004.008953. PMC 1748044. PMID 15923467.
- Laura Bach (20 June 2018). "Tobacco Industry targeting of women and girls" (PDF). Campaign for Tobacco-Free Kids. Retrieved 18 August 2018.
- "[Box], Virginia Slims: A Case Study in Marketing Success". March 2001.
- Grandpre J, Alvaro EM, Burgoon M, Miller CH, Hall JR (2003). "Adolescent reactance and anti-smoking campaigns: a theoretical approach". Health Communication. 15 (3): 349–66. doi:10.1207/S15327027HC1503_6. PMID 12788679. S2CID 2511851.
- Pechacek TF, Nayak P, Slovic P, Weaver SR, Huang J, Eriksen MP (November 2017). "Reassessing the importance of 'lost pleasure' associated with smoking cessation: implications for social welfare and policy". Tobacco Control. 27 (e2): tobaccocontrol–2017–053734. doi:10.1136/tobaccocontrol-2017-053734. PMC 6176518. PMID 29183920.
- Tobacco Products Scientific Advisory Committee (TPSAC) of the Center for Tobacco Products of the Food and Drug Administration (FDA) (21 July 2011). Menthol Cigarettes and Public Health: Review of the Scientific Evidence and Recommendations (PDF). US Food and Drug Administration. p. 252. Archived from the original (PDF) on 17 May 2017. Retrieved 24 May 2018.
- Woerndl M, Papagiannidis S, Bourlakis M, Li F (2008). "Internet-induced marketing techniques: Critical factors in viral marketing campaigns". International Journal of Business Science and Applied Management. 3 (1).
- Bach L (10 April 2018), "Tobacco Product Marketing on the Internet" (PDF), Campaign for Tobacco-Free Kids, retrieved 25 May 2018
- Newman AA (10 August 2014). "A Less Defiant Tack in a Campaign to Curb Smoking by Teenagers". The New York Times. Retrieved 24 May 2018.
- Newman AA (24 July 2014). "Hard-to-Watch Commercials to Make Quitting Smoking Easier". The New York Times. Retrieved 24 May 2018.
- "Recommendations of the 1991 "Archetype Project"". commissioned by Philip Morris (now Altria) from Rapaille Associates.
- "Except from an internal industry document". Stanford Research into the Impact of Tobacco Advertising. Archived from the original on 24 February 2021. Retrieved 25 May 2018.
- Source for example quote is an ad for blu e-cigarettes, accessible at: Stanford Research into the Impact of Tobacco Advertising database. "Nobody likes a quitter". tobacco.stanford.edu. Stanford University. Archived from the original on 20 February 2017. Retrieved 14 October 2018.
- Peate I (2005). "The effects of smoking on the reproductive health of men". British Journal of Nursing. 14 (7): 362–6. doi:10.12968/bjon.2005.14.7.17939. PMID 15924009.
- "The Tobacco Reference Guide". Archived from the original on 15 July 2006. Retrieved 15 July 2006.
- Kendirci M, Nowfar S, Hellstrom WJ (January 2005). "The impact of vascular risk factors on erectile function". Drugs of Today. 41 (1): 65–74. doi:10.1358/dot.2005.41.1.875779. PMID 15753970.
- Elliott S (6 February 2004). "James J. Jordan, advertising sloganeer, dies at 73". The New York Times. Archived from the original on 7 May 2006. Retrieved 2 August 2006.
- Parrott AC (April 2003). "Cigarette-derived nicotine is not a medicine" (PDF). The World Journal of Biological Psychiatry. 4 (2): 49–55. doi:10.3109/15622970309167951. PMID 12692774. S2CID 26903942. Archived from the original (PDF) on 9 August 2017. Retrieved 10 October 2018.
- Parrott AC (March 2006). "Nicotine psychobiology: how chronic-dose prospective studies can illuminate some of the theoretical issues from acute-dose research". Psychopharmacology. 184 (3–4): 567–76. doi:10.1007/s00213-005-0294-y. PMID 16463194. S2CID 11356233.
- Prochaska JJ, Hall SM, Bero LA (May 2008). "Tobacco use among individuals with schizophrenia: what role has the tobacco industry played?". Schizophrenia Bulletin. 34 (3): 555–67. doi:10.1093/schbul/sbm117. PMC 2632440. PMID 17984298.
- Wan W (24 August 2017). "New ads accuse Big Tobacco of targeting soldiers and people with mental illness". The Washington Post. ISSN 0190-8286. Retrieved 27 May 2018.
- "Burden of Tobacco Use in the U.S.: Current Cigarette Smoking Among U.S. Adults Aged 18 Years and Older". Centers for Disease Control and Prevention. 23 April 2018.
- Phillips E, Wang TW, Husten CG, Corey CG, Apelberg BJ, Jamal A, Homa DM, King BA (November 2017). "Tobacco Product Use Among Adults - United States, 2015". MMWR. Morbidity and Mortality Weekly Report. 66 (44): 1209–1215. doi:10.15585/mmwr.mm6644a2. PMC 5679591. PMID 29121001.
- Yerger VB, Malone RE (December 2002). "African American leadership groups: smoking with the enemy". Tobacco Control. 11 (4): 336–45. doi:10.1136/tc.11.4.336. PMC 1747674. PMID 12432159.
- Nichter M, Cartwright E (1991). "Saving the Children for the Tobacco Industry". Medical Anthropology Quarterly. 5 (3): 236–56. doi:10.1525/maq.1991.5.3.02a00040. JSTOR 648675.
- Wan W (13 June 2017). "America's new tobacco crisis: The rich stopped smoking, the poor didn't". The Washington Post. ISSN 0190-8286. Retrieved 27 May 2018.
- "#STOPPROFILING: Tobacco is a social justice issue". Truth Initiative. 9 February 2017. Retrieved 27 May 2018.
- "Tobacco-Related Disparities - Tobacco Use by Geographic Region - Smoking & Tobacco Use". CDC's Office on Smoking and Health. 5 September 2018. Retrieved 1 November 2017.
- Baig SA, Pepper JK, Morgan JC, Brewer NT (June 2017). "Social identity and support for counteracting tobacco company marketing that targets vulnerable populations". Social Science & Medicine. 182: 136–141. doi:10.1016/j.socscimed.2017.03.052. PMC 5474382. PMID 28427731.
- Lee JG, Griffin GK, Melvin CL (August 2009). "Tobacco use among sexual minorities in the USA, 1987 to May 2007: a systematic review". Tobacco Control. 18 (4): 275–82. doi:10.1136/tc.2008.028241. PMID 19208668.
- Apollonio DE, Malone RE (December 2005). "Marketing to the marginalised: tobacco industry targeting of the homeless and mentally ill". Tobacco Control. 14 (6): 409–15. doi:10.1136/tc.2005.011890. PMC 1748120. PMID 16319365.
- Engardio JP (2 May 2001). "Smoking Gun". SF Weekly. Archived from the original on 4 July 2015. Retrieved 25 May 2018.
Tobacco industry documents expose an R.J. Reynolds marketing plan targeting S.F. gays and homeless people. Its name: Project SCUM.
- "Original document from Project SCUM". Stanford Research into the Impact of Tobacco Advertising. Archived from the original on 2 March 2021. Retrieved 25 May 2018.
- Rosenblatt R (20 March 1994). "How Do Tobacco Executives Live With Themselves?". The New York Times. ISSN 0362-4331. Retrieved 25 May 2018.
- Bates C, Rowell A. "Tobacco explained: The truth about the tobacco industry ...in its own words" (PDF). Tobacco Free Initiative. Archived from the original (PDF) on 18 July 2004. Retrieved 20 October 2018.
- "Tobacco CEO's Statement to Congress 1994 | UCSF Academic Senate". senate.ucsf.edu.
- Mallock N, Böss L, Burk R, Danziger M, Welsch T, Hahn H, Trieu HL, Hahn J, Pieper E, Henkler-Stephani F, Hutzler C, Luch A (June 2018). "Levels of selected analytes in the emissions of "heat not burn" tobacco products that are relevant to assess human health risks". Archives of Toxicology. 92 (6): 2145–2149. doi:10.1007/s00204-018-2215-y. PMC 6002459. PMID 29730817.
- El-Toukhy S, Baig SA, Jeong M, Byron MJ, Ribisl KM, Brewer NT (August 2018). "Impact of modified risk tobacco product claims on beliefs of US adults and adolescents". Tobacco Control. 27 (Suppl 1): tobaccocontrol–2018–054315. doi:10.1136/tobaccocontrol-2018-054315. PMC 6202195. PMID 30158212.
- Harris B (May 2011). "The intractable cigarette 'filter problem'". Tobacco Control. 20 Suppl 1 (Suppl_1): i10–6. doi:10.1136/tc.2010.040113. PMC 3088411. PMID 21504917.
- Pollay RW, Dewhirst T (March 2002). "The dark side of marketing seemingly "Light" cigarettes: successful images and failed fact". Tobacco Control. 11 (Suppl 1): I18–31. doi:10.1136/tc.11.suppl_1.i18. PMC 1766068. PMID 11893811.
- Staal, YC; van de Nobelen, S; Havermans, A; Talhout, R (28 May 2018). "New Tobacco and Tobacco-Related Products: Early Detection of Product Development, Marketing Strategies, and Consumer Interest". JMIR Public Health and Surveillance. 4 (2): e55. doi:10.2196/publichealth.7359. PMC 5996176. PMID 29807884.
- McKelvey K, Popova L, Kim M, Lempert LK, Chaffee BW, Vijayaraghavan M, Ling P, Halpern-Felsher B (August 2018). "IQOS labelling will mislead consumers". Tobacco Control. 27 (Suppl 1): tobaccocontrol–2018–054333. doi:10.1136/tobaccocontrol-2018-054333. PMC 6252493. PMID 30158208.
- "For your Throat". Stanford Research into the Impact of Tobacco Advertising. Archived from the original on 2 June 2018. Retrieved 4 September 2018.
- Doll R (June 1998). "Uncovering the effects of smoking: historical perspective". Statistical Methods in Medical Research. 7 (2): 87–117. doi:10.1177/096228029800700202. PMID 9654637. S2CID 154707.
- Keith Wailoo, Pushing Cool: Big Tobacco, Racial Marketing, and the Untold Story of the Menthol Cigarette (2021) excerpt
- Kennedy P (6 July 2012). "Who Made That Cigarette Filter?". The New York Times. ISSN 0362-4331. Retrieved 4 September 2018.
- Kozlowski LT, O'Connor RJ (March 2002). "Cigarette filter ventilation is a defective design because of misleading taste, bigger puffs, and blocked vents". Tobacco Control. 11 (Suppl 1): I40–50. doi:10.1136/tc.11.suppl_1.i40. PMC 1766061. PMID 11893814.
- Light but just as deadly, by Peter Lavelle. The Pulse, 21 October 2004.
- The Truth About "Light" Cigarettes: Questions and Answers, from the National Cancer Institute factsheet
- 'Safer' cigarette myth goes up in smoke, by Andy Coghlan. New Scientist, 2004
- Ling, Pamela M; Glantz, Stanton A (2004). "Tobacco Industry Research on Smoking Cessation". Journal of General Internal Medicine. 19 (5 Pt 1): 419–426. doi:10.1111/j.1525-1497.2004.30358.x. ISSN 0884-8734. PMC 1492251. PMID 15109339.
- Caputi, TL (24 August 2016). "Industry watch: heat-not-burn tobacco products are about to reach their boiling point". Tobacco Control. 26 (5): 609–610. doi:10.1136/tobaccocontrol-2016-053264. PMID 27558827. S2CID 46170776.
- "Further development of the partial guidelines for implementation of Articles 9 and 10 of the WHO FCTC" (PDF). World Health Organization. 12 July 2016. pp. 5–6.
- Dautzenberg, B.; Dautzenberg, M.-D. (2018). "Le tabac chauffé : revue systématique de la littérature" [Systematic analysis of the scientific literature on heated tobacco]. Revue des Maladies Respiratoires (in French). 36 (1): 82–103. doi:10.1016/j.rmr.2018.10.010. ISSN 0761-8425. PMID 30429092.
- "Tobacco company charged over importing prohibited product". The New Zealand Herald. 18 May 2017.
- Jane Cheung (24 May 2019). "New forms of smoking catch on". The Standard.
- Grana R, Benowitz N, Glantz SA (May 2014). "E-cigarettes: a scientific review". Circulation. 129 (19): 1972–86. doi:10.1161/circulationaha.114.007667. PMC 4018182. PMID 24821826.
- World Health Organization. "Electronic nicotine delivery systems" (PDF). pp. 1–13. Retrieved 28 August 2014.
- England LJ, Bunnell RE, Pechacek TF, Tong VT, McAfee TA (August 2015). "Nicotine and the Developing Human: A Neglected Element in the Electronic Cigarette Debate". American Journal of Preventive Medicine. 49 (2): 286–93. doi:10.1016/j.amepre.2015.01.015. PMC 4594223. PMID 25794473.
- "New e-cigarette rules coming to Quebec". CBC News. Canadian Broadcasting Corporation.
- Chaiton M, Diemert L, Cohen JE, Bondy SJ, Selby P, Philipneri A, Schwartz R (June 2016). "Estimating the number of quit attempts it takes to quit smoking successfully in a longitudinal cohort of smokers". BMJ Open. 6 (6): e011045. doi:10.1136/bmjopen-2016-011045. PMC 4908897. PMID 27288378.
- National Cancer Institute (18 August 2005). ""Light" Cigarettes and Cancer Risk" (cgvFactSheet). National Cancer Institute. Retrieved 23 May 2018.
- Rigotti NA, Tindle HA (March 2004). "The fallacy of "light" cigarettes". BMJ. 328 (7440): E278–9. doi:10.1136/bmj.328.7440.E278. PMC 2901853. PMID 15016715.
- Kropp RY, Halpern-Felsher BL (October 2004). "Adolescents' beliefs about the risks involved in smoking "light" cigarettes". Pediatrics. 114 (4): e445–51. doi:10.1542/peds.2004-0893. PMID 15466070.
- Gilpin EA, White MM, Messer K, Pierce JP (August 2007). "Receptivity to tobacco advertising and promotions among young adolescents as a predictor of established smoking in young adulthood". American Journal of Public Health. 97 (8): 1489–95. doi:10.2105/AJPH.2005.070359. PMC 1931446. PMID 17600271.
- Boseley S, Collyns D, Lamb K, Dhillon A (9 March 2018). "How children around the world are exposed to cigarette advertising". The Guardian. ISSN 0261-3077. Retrieved 27 May 2018.
- "Big Tobacco, Tiny Targets". Campaign for Tobacco-Free Kids. Retrieved 27 May 2018.
- Grana RA, Ling PM (April 2014). ""Smoking revolution": a content analysis of electronic cigarette retail websites". American Journal of Preventive Medicine. 46 (4): 395–403. doi:10.1016/j.amepre.2013.12.010. PMC 3989286. PMID 24650842.
- "E-cigarettes and Lung Health". American Lung Association. 2015. Archived from the original on 4 October 2015.
- "Myths and Facts About E-cigarettes". American Lung Association. 2015. Archived from the original on 4 December 2015.
- Welch A (5 April 2018). "Facebook is used to promote tobacco, despite policies against it, study finds". CBS News. Retrieved 18 May 2018.
- Nelson JP (2003). "Cigarette Demand, Structural Change, and Advertising Bans: International Evidence, 1970-1995". Contributions in Economic Analysis & Policy. 2. doi:10.2202/1538-0645.1111. S2CID 8881878.
- Nelson JP (2006). "Cigarette advertising regulation: A meta-analysis". International Review of Law and Economics. 26 (2): 195–226. doi:10.1016/j.irle.2006.08.005.
- Nelson JP (March 2010). "What is learned from longitudinal studies of advertising and youth drinking and smoking? A critical assessment". International Journal of Environmental Research and Public Health. 7 (3): 870–926. doi:10.3390/ijerph7030870. PMC 2872298. PMID 20617009.
- Myers ML (27 March 2001). "Statement: Surgeon General's Report on Women and Tobacco Underscores Need for Congress to Grant FDA Authority Over Tobacco". Campaign for Tobacco-Free Kids.
- "Tobacco advertising and promotion". Action on Smoking and Health. May 2006. Archived from the original on 25 June 2007.
- Wasowicz A, Feleszko W, Goniewicz ML (October 2015). "E-Cigarette use among children and young people: the need for regulation". Expert Review of Respiratory Medicine. 9 (5): 507–9. doi:10.1586/17476348.2015.1077120. PMID 26290119. S2CID 207206915.
- "Big Tobacco Keeps Pushing into E-Cigarettes". Bloomberg.com. 17 June 2014. Retrieved 4 September 2018.
- "Doctors Hawk Cigarettes". Stanford Research Into the Impact of Tobacco Advertising (SRITA). Archived from the original on 25 May 2018. Retrieved 26 May 2018.
- "Children Smoking". Stanford Research Into the Impact of Tobacco Advertising (SRITA). Archived from the original on 21 May 2018. Retrieved 21 May 2018.
Further reading
- "Timeline: Smoking and disease". BBC News. 22 June 2004. Retrieved 12 July 2005.
- "Formula One tobacco advertising to go". BBC News. 3 December 1997. Retrieved 9 July 2005.
- "Formula One tobacco sponsorship ban scrapped". BBC News. 5 November 1997. Retrieved 9 July 2005.
- Wheeler B (13 February 2004). "Has the tobacco ad ban worked?". BBC News. Retrieved 18 July 2005.
- "Tobacco advert rules introduced". BBC News. 21 December 2004. Retrieved 18 July 2005.
- Leonard T (21 September 2005). "TV advertisers shift focus to placing products in shows". Telegraph.co.uk. Retrieved 24 September 2005.
- "The history of smoking". ForestOnline. 30 March 2006. Archived from the original on 5 January 2007. Retrieved 12 July 2005.
- "Women and smoking – A report of the Surgeon General 2001". Archived from the original on 22 February 2009. Retrieved 12 July 2005.
- "Tobacco advertising and promotion". ASH.org.uk. May 2006. Archived from the original on 25 June 2007.
- "ASH briefing: The UK ban on tobacco advertising". ASH.org.uk. June 2004. Archived from the original on 2 February 2007.
- Pritcher L. "More About Tobacco Advertising and the Tobacco Collections: Tobacco advertising". Emergence of Advertising in America (EAA). Retrieved 13 July 2005.
- "Tobacco Ads Will Be Removed from School Magazines". ConsumerAffairs.com. 20 June 2005. Archived from the original on 14 January 2006. Retrieved 18 July 2005.
- "RJ Reynolds hints at leaving NASCAR". The Sporting News. 5 February 2003. Archived from the original on 8 April 2004. Retrieved 10 September 2005.
- "Big Tobacco's Big Seduction: Women, Tobacco and the Glorification of Addiction, An interview with Mary Assunta". Multinational Monitor. 26 (5–6). May–June 2005.
- Steinhart Y, Carmon Z, Trope Y (September 2013). "Warnings of adverse side effects can backfire over time". Psychological Science. 24 (9): 1842–7. doi:10.1177/0956797613478948. PMID 23912069. S2CID 8445279.
External links
- Examples of Tobacco Advertising
- Snuff advertising in the collection of Helmetta Historical Society
- UCSF Tobacco Industry Videos Collection
- UCSF Tobacco Industry Audio Recordings Collection
- Gallery of vintage American tobacco print advertisements
- Extensive online tobacco advertising collection at Stanford University
- Cigarette Cards: ABCs, at the New York Public Library Digital Gallery
- Catalogue of heraldic tobacco and trading cards
- Duke Tobacco Company Cigarette Cards Archived 19 May 2008 at the Wayback Machine, at the Z. Smith Reynolds Library, Wake Forest University
- Stanford University research into the impact of tobacco advertising; website with an extensive gallery of historical and current nicotine adverts and related material
- Laws and legislation
- "Tobacco Advertising and Promotion Act 2002 (c. 36) Tobacco Advertising and Promotion Act 2002]" in the UK
- "Tobacco advertising" at the British Department of Health
- "RJR-MacDonald V. Canada" at Health Canada
- Anti-smoking organizations
- "Advertising Archived 18 May 2005 at the Wayback Machine" at SmokeHelp.org
- "Fact Sheet - Tobacco Advertising" by the Non Smokers' Movement of Australia
- Smoke Free Movies Campaign by the University of California, San Francisco
- Miscellaneous
- "Health and the Mass Media – Tobacco Archived 15 June 2005 at the Wayback Machine" at the School of Public Health, University of Sydney
- "Tobacco advertising Archived 15 June 2005 at the Wayback Machine" at Tobacco Control Factsheets
- Roswell Park Cancer Institute Tobacco Document Collections and Resources (Archived)
- "Tobacco and alcohol sports sponsorship" at The Globe Magazine
- Collection of Anti-Smoking TV Commercials
- Breathtaking Classic Cigarette Ads Archived 19 June 2010 at the Wayback Machine – slideshow by Life magazine
| Country and region |
| ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Religion | |||||||||||||
| Health | |||||||||||||
| Smoking ban |
| ||||||||||||
| Other | |||||||||||||
| |||||||||||||
| Types |  | ||
|---|---|---|---|
| Components | |||
| Peripherals | |||
| Culture | |||
| Health issues | |||
| Related products | |||
| Tobacco industry |
| ||
| Government and the law | |||
| Lists | |||
| |||