Occipital condyles
The occipital condyles are undersurface protuberances of the occipital bone in vertebrates, which function in articulation with the superior facets of the atlas vertebra.
| Occipital condyles | |
|---|---|
 Occipital bone. Outer surface. Occipital condyles are shown in red. | |
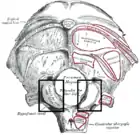 Occipital bone. Outer surface. (Condyle for artic. with atlas labeled at lower left.) | |
| Details | |
| Identifiers | |
| Latin | Condylus occipitalis |
| TA98 | A02.1.04.014 |
| TA2 | 557 |
| FMA | 52861 |
| Anatomical terminology | |
The condyles are oval or reniform (kidney-shaped) in shape, and their anterior extremities, directed forward and medialward, are closer together than their posterior, and encroach on the basilar portion of the bone; the posterior extremities extend back to the level of the middle of the foramen magnum.
The articular surfaces of the condyles are convex from before backward and from side to side, and look downward and lateralward.
To their margins are attached the capsules of the atlanto-occipital joints, and on the medial side of each is a rough impression or tubercle for the alar ligament.
At the base of either condyle the bone is tunnelled by a short canal, the hypoglossal canal.
Clinical significance
Fracture of an occipital condyle may occur in isolation, or as part of a more extended basilar skull fracture. Isolated condyle fracture is a type of craniocervical injury. The classification of Anderson and Montesano distinguishes three types of occipital condyle fracture:
- Type I: Isotated impaction fracture of the occipital condyle, due to compression by the atlas or dens. This injury is usually stable; significant displacement of fragments is rare.
- Type II: Occipital basilar skull fracture extending into the condyle, resulting from direct trauma. The craniocervical junction usually stays stable, but neurologic injury may occur from the blow to the head.
- Type III: Isolated avulsion of the condyle with displacement towards the alar ligament, due to forced rotation / lateral bending. This injury tends to be unstable and may co-occur with atlanto-occipital subluxation or dislocation. Neurological injury may occur and range from minor to instantly fatal.
Minimally displaced fractures are treated conservatively. Surgery may become necessary if there is significant compression of the brainstem, spinal cord, the lower cranial nerves or cervical arteries. Bilateral condyle fractures (e.g. as part of an atlanto-occipital dislocation or the "occipital ring fracture") are rare, but often fatal.
Symptoms of an isolated occipital condyle fracture resemble those of other craniocervical injuries, including high cervical pain, reduced range of motion, unusual head / neck posture, prevertebral swelling, and possibly lower cranial nerve (IX, X, XI, XII) deficits, tetraparesis or abnormal breathing. Among these, cranial nerve deficits are the most characteristic due to the proximity of the injury to the jugular foramen and hypoglossal canal. Onset of neurologic symptoms may be immediate or delayed.
The prevalence of occipital condyle fractures is not definitely known. Once thought to be a rare injury, it is nowadays believed to constitute 1-3% of all blunt craniocervical traumas. It is most commonly seen in high-energy trauma, often associated with other skull and/or cervical spine injuries.[1][2]
In reptiles and birds
The presence of a single occipital condyle in dinosaurs (including birds) and crocodilians contrasts with the condition in amphibians and synapsids (including mammals such as Homo sapiens), where two occipital condyles are present. Here, the occipital condyle is a single rounded projection that is present on the rear of the skull and articulates with the first cervical (neck) vertebra. Functionally it allows the head to move from side to side, up and down, as well as to rotate. A combination of a number of smaller bones (such as the basioccipital and exoccipitals) participate in the formation of this structure.
In most dinosaurs the occipital condyle is situated at the rear part of the skull, below the foramen magnum, and points toward the posterior of the animal. Some exceptions to this exist, such as in the iguanodontian Anabisetia saldiviai where the condyle points downward. In some dinosaurs, where the skull has not been preserved, the presence of a small occipital condyle suggests to some paleontologists that the skull of the dinosaur was relatively small.
See also
References
- Watts E (January 2020). "Occipital Condyle Fractures". Ortho Bullets. Lineage Medical, Inc. Retrieved 22 March 2018.
- Clayman DA, Sykes CH, Vines FS (August 1994). "Occipital condyle fractures: clinical presentation and radiologic detection" (PDF). AJNR. American Journal of Neuroradiology. 15 (7): 1309–15. PMID 7976943.
![]() This article incorporates text in the public domain from page 131 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 131 of the 20th edition of Gray's Anatomy (1918)
Further reading
- Anderson PA, Montesano PX (July 1988). "Morphology and treatment of occipital condyle fractures". Spine. 13 (7): 731–6. doi:10.1097/00007632-198807000-00004. PMID 3194779. S2CID 32286254.
- Nanda A, Vincent DA, Vannemreddy PS, Baskaya MK, Chanda A (February 2002). "Far-lateral approach to intradural lesions of the foramen magnum without resection of the occipital condyle". Journal of Neurosurgery. 96 (2): 302–9. doi:10.3171/jns.2002.96.2.0302. PMID 11841072.
- Bloom AI, Neeman Z, Slasky BS, Floman Y, Milgrom M, Rivkind A, Bar-Ziv J (March 1997). "Fracture of the occipital condyles and associated craniocervical ligament injury: incidence, CT imaging and implications". Clinical Radiology. 52 (3): 198–202. doi:10.1016/s0009-9260(97)80273-5. PMID 9091254.
- Tuli S, Tator CH, Fehlings MG, Mackay M (August 1997). "Occipital condyle fractures". Neurosurgery. 41 (2): 368–76, discussion 376-7. doi:10.1097/00006123-199708000-00006. PMID 9257304.
- Orbay T, Aykol S, Seçkin Z, Ergün R (May 1989). "Late hypoglossal nerve palsy following fracture of the occipital condyle". Surgical Neurology. 31 (5): 402–4. doi:10.1016/0090-3019(89)90076-1. PMID 2711317.
- Bolender N, Cromwell LD, Wendling L (October 1978). "Fracture of the occipital condyle". AJR. American Journal of Roentgenology. 131 (4): 729–31. doi:10.2214/ajr.131.4.729. PMID 102174.
- Vishteh AG, Crawford NR, Melton MS, Spetzler RF, Sonntag VK, Dickman CA (January 1999). "Stability of the craniovertebral junction after unilateral occipital condyle resection: a biomechanical study". Journal of Neurosurgery. 90 (1 Suppl): 91–8. doi:10.3171/spi.1999.90.1.0091. PMID 10413132.
- Clayman DA, Sykes CH, Vines FS (August 1994). "Occipital condyle fractures: clinical presentation and radiologic detection". AJNR. American Journal of Neuroradiology. 15 (7): 1309–15. PMID 7976943.
- Young WF, Rosenwasser RH, Getch C, Jallo J (February 1994). "Diagnosis and management of occipital condyle fractures". Neurosurgery. 34 (2): 257–60, discussion 260-1. doi:10.1097/00006123-199402000-00008. PMID 8177386.
- Spencer JA, Yeakley JW, Kaufman HH (July 1984). "Fracture of the occipital condyle". Neurosurgery. 15 (1): 101–3. doi:10.1097/00006123-198407000-00018. PMID 6472584.
External links
- lesson9 at The Anatomy Lesson by Wesley Norman (Georgetown University)
- "Anatomy diagram: 34256.000-2". Roche Lexicon - illustrated navigator. Elsevier. Archived from the original on 2014-01-01.
- "Anatomy diagram: 34257.000-1". Roche Lexicon - illustrated navigator. Elsevier. Archived from the original on 2014-01-01.
- occipital condyles on Triceratops