Accessory bone
An accessory bone or supernumerary bone is a bone that is not normally present in the body, but can be found as a variant in a significant number of people. It poses a risk of being misdiagnosed as bone fractures on radiography.[2]
Wrist and hand
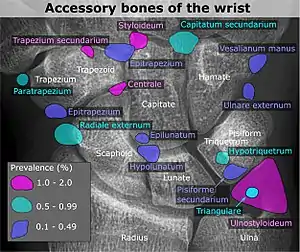

| Accessory bone | Prevalence on the right (R) and left (L)[5] |
|---|---|
| Os ulnostyloideum | 1.5% R, 2.4% L |
| Os centrale | 1.3% R, 2.1% L |
| Os trapezium secundarium | 0.5% R, 2.1% L |
| Os styloideum | 1.2% R, 1.2% L |
| Os radiale externum | 1% R, 0.9% L |
| Os triangulare | 1% R, 0.9% L |
| Os paratrapezium | 0.3% R, 0.9% L |
| Os capitatum secundarium | 0.8% R, 0.3% L |
| Os Hypotriquetrum | 0.5% R |
| Os hypolunatum | 0.3% L |
| Os epilunatum | 0.3% R, 0.3% L |
| Os ulnare externum | 0.3% L |
| Os pisiforme secundarium | 0.3% R |
| Os epitrapezium | 0.3% L |
| Os vesalianum manus | 0.3% L |
Os ulnostyloideum
The os ulnostyloideum is an ulnar styloid process that is not fused to the rest of the ulna bone.[6] On X-rays, an os ulnostyloideum is sometimes mistaken for an avulsion fracture of the styloid process. However, the distinction between these is extremely difficult.[6][7] It is alleged that the os ulnostyloideum has a close relationship with or is synonymous with the os triquetrum secundarium.[8]
Os centrale
The os carpi centrale (also briefly os centrale) is, where present, located on the dorsal side of the wrist between the scaphoid, the trapezoid and capitate, radially to the deep fossa of the capitate. The bone is present in almost every human embryo of 17–49 mm length, but then usually fuses with the ulnar side of the scaphoid. Sometimes it fuses with the capitate or the trapezoid. The literature also refers to an os centrale at the palm of the carpus, but this existence is questioned.[6]
In most primates, including orangutans and gibbons, the os centrale is an independent bone that is attached to the scaphoid by strong ligaments. Conversely, in African apes and humans, the os centrale normally fuses to the scaphoid early in development.[9] In chimpanzees, the bone fuses with the scaphoid first after birth, while in gibbons and orangutans this occurs first at older age.[10] A good number of scholars have construed the scaphoid-centrale fusion as a functional adaptation to knuckle-walking,[11] since a fused morphology would better cope with the increased shear stress on this joint during this kind of quadrupedal locomotion. The results from a simulation study have shown that fused scaphoid-centrales show lower stress values as compared to non fused morphologies, thus supporting a biomechanical explanation for the scaphoid-centrale fusion as a functional adaptation for knuckle-walking.[12]
Ankle

Accessory bones at the ankle mainly include:
- Os subtibiale, with a prevalence of approximately 1%.[14] It is a secondary ossification center of the distal tibia that appears during the first year of life, and which in most people fuses with the shaft at approximately 15 years in females and approximately 17 years in males.[14]
- Os subfibulare, with a prevalence of approximately 0.2%.[15]
Os trigonum (further described below) may also be seen on an ankle X-ray.
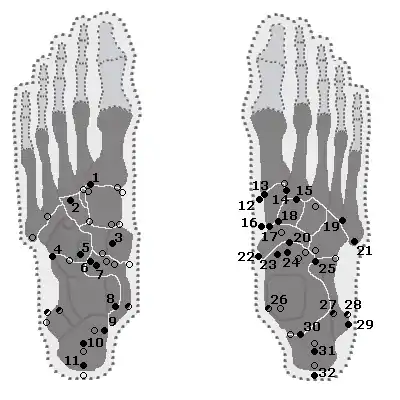
Foot

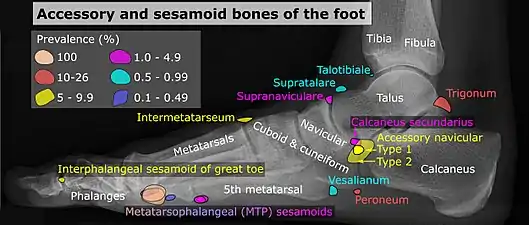
| Bone | Prevalence[17] |
|---|---|
| Sesamoid bones | |
| Sesamoids at the metatarsophalangeal (MTP) joint of the great toe | Always present |
| Sesamoid of the second metatarsal | 0.4% |
| Sesamoid of the third metatarsal | 0.2% |
| Sesamoid of the fourth metatarsal | 0.1% |
| Sesamoids of the fifth metatarsal | 4.3% |
| Sesamoid of the interphalangeal (IP) joint of the great toe | 2–13% |
| Ossicles | |
| Os trigonum (not visible in this dorsoplantar projection) | 7–25% |
| Os peroneum | Up to 26% |
| Accessory navicular | 2–21% |
| Os intermetatarseum | 1–13% |
| Os supranaviculare, also called the talonavicular bone | 1.0–3.5% |
| Os calcaneus secundarium | 0.6–7% |
| Os supratalare | 0.2–2.4% |
| Os vesalianum | 0.1–1% |
| Os talotibiale | 0.5% |
Accessory navicular

An accessory navicular bone, also called os tibiale externum, occasionally develops in front of the ankle towards the inside of the foot. This bone may be present in approximately 2–21% of the general population and is usually asymptomatic.[18][19][20] When it is symptomatic, surgery may be necessary.
The Geist classification divides the accessory navicular bones into three types.[20]
- Type 1: An os tibiale externum is a 2–3 mm sesamoid bone in the distal posterior tibialis tendon. Usually asymptomatic.
- Type 2: Triangular or heart-shaped ossicle measuring up to 12 mm, which represents a secondary ossification center connected to the navicular tuberosity by a 1–2 mm layer of fibrocartilage or hyaline cartilage. Portions of the posterior tibialis tendon sometimes insert onto the accessory ossicle, which can cause dysfunction, and therefore, symptoms.
- Type 3: A cornuate navicular bone represents an enlarged navicular tuberosity, which may represent a fused Type 2 accessory bone. Occasionally symptomatic due to bunion formation.
Os trigonum
The os trigonum or accessory talus represents a failure of fusion of the lateral tubercle of the posterior process of the talus bone. Is estimated to be present in 7–25% of adults.[17] It can be mistaken for an avulsion fracture of lateral tubercle of talus (Shepherd fracture) or a fracture of the Stieda process. In most cases, Os Trigonum will go unnoticed, but with some ankle injuries it can get trapped between the heel and ankle bones which irritates the surrounding structures, leading to Os Trigonum Syndrome.[21]




Less common accessory bones
Other locations
Neck
- Nodules in the posterior margin of the nuchal ligament form bone tissue in approximately 11% of males and 3–5% in females after the third decade of life, and may then be regarded to be sesamoid bones.[22]
Shoulder
.jpg.webp)
- An os acromiale forms when any of its four ossification centers fail to fuse. These four ossification centers are called (from tip to base) pre-acromion, meso-acromion, meta-acromion, and basi-acromion. In most cases, the first three fuse at 15–18 years, whereas the base part fuses to the scapular spine at 12 years. Such failure to fuse occurs in between 1% and 15% of cases.[23][24] It rarely causes pain.
Vertebral column
- An Oppenheimer ossicle is found in approximately 4% (range 1–7%) of individuals.[25] It is associated with the facet joints of lumbar spines. It usually occurs as a single, unilateral ossicle at the inferior articular processes, but can also occur at the superior articular processes.[25]
See also
References
- Luijkx, Tim; Knipe, Henry. "Fabella". Radiopaedia. Retrieved 2015-09-18.
- T.E. Keats, M.W. Anderson, Atlas of normal roentgen variants that may simulate disease. 7th edition, Mosby Inc. 2001, ISBN 0323013228
- Reference list for image is located at Commons:Template:Accessory bones of the wrist – references.
-
- Location and structure: Erica Chu, Donald Resnick. "MRI Web Clinic — June 2014: Sesamoid Bones: Normal and Abnormal". Retrieved 2017-11-04.
- Prevalences: Chen W; Cheng J; Sun R; Zhang Z; Zhu Y; Ipaktchi K; et al. (2015). "Prevalence and variation of sesamoid bones in the hand: a multi-center radiographic study". Int J Clin Exp Med. 8 (7): 11721–6. PMC 4565393. PMID 26380010. - "Poster Abstracts" (PDF). Association for Sports Medicine of Serbia (Udruženje za medicinu sporta Srbije). 2006. Retrieved 2017-11-03., citing: Natsis K.; Beletsiotis A.; Terzidis I.; Gigis P. "A study of the accessory bones of the foot. Incidence in the Greek population-clinical significance" (PDF).
- R. O'Rahilly. A survey of carpal and tarsal anomalies. J Bone Joint Surg Am. 1953; 35: 626–642
- T.E. Keats, M.W. Anderson. Atlas of normal roentgen variants that may simulate disease. 7th edition, Mosby Inc. 2001 ISBN 0323013228
- A. Köhler. Röntgenology. The borderlands of the normal and early pathological in the skiagram. Translated by Arthur Turnbull. Ed. 2. Baillière, Tindall & Cox, Londen, 1935
- Schultz, Adolph H. (1936-12-01). "Characters Common to Higher Primates and Characters Specific for Man (Continued)". The Quarterly Review of Biology. 11 (4): 425–455. doi:10.1086/394517. ISSN 0033-5770.
- A.H. Schultz. Characters common to higher primates and characters specific for man. Quart Rev Biol. 1936; 11: 259–283; 425–455
- Richmond, Brian G.; Begun, David R.; Strait, David S. (2001). "Origin of human bipedalism: The knuckle-walking hypothesis revisited". American Journal of Physical Anthropology. 116 (S33): 70–105. doi:10.1002/ajpa.10019. ISSN 0002-9483. PMID 11786992.
- Püschel, Thomas A.; Marcé-Nogué, Jordi; Chamberlain, Andrew T.; Yoxall, Alaster; Sellers, William I. (2020-02-26). "The biomechanical importance of the scaphoid-centrale fusion during simulated knuckle-walking and its implications for human locomotor evolution". Scientific Reports. 10 (1): 3526. doi:10.1038/s41598-020-60590-6. ISSN 2045-2322. PMC 7044280. PMID 32103129.
- Reference list for shapes and locations for included bones is located at: Commons:Template:Accessory bones of the ankle – references.
- Frank Gaillard; Mohammad Taghi Niknejad; et al. "Os subtibiale". Radiopaedia. Retrieved 2017-11-05.
- Champagne, IM; Cook, DL; Kestner, SC; Pontisso, JA; Siesel, KJ (1999). "Os subfibulare. Investigation of an accessory bone". Journal of the American Podiatric Medical Association. 89 (10): 520–524. doi:10.7547/87507315-89-10-520. ISSN 8750-7315. PMID 10546424.
- A reference list for shapes, locations and prevalences for included bones is located at Commons:Template:Accessory and sesamoid bones of the foot – references.
- Nwawka, O. Kenechi; Hayashi, Daichi; Diaz, Luis E.; Goud, Ajay R.; Arndt, William F.; Roemer, Frank W.; Malguria, Nagina; Guermazi, Ali (2013). "Sesamoids and accessory ossicles of the foot: anatomical variability and related pathology". Insights into Imaging. 4 (5): 581–593. doi:10.1007/s13244-013-0277-1. ISSN 1869-4101. PMC 3781258. PMID 24006205.
- "Accessory Navicular". Wheeless' Textbook of Orthopaedics.
- "Macrorad Teleradyoloji Olgu Sunumları – SYMPTOMATIC ACCESSORY NAVICULAR BONE".
- Miller TT, Staron RB, Feldman F, Parisien M, Glucksman WJ, Gandolfo LH (June 1995). "The symptomatic accessory tarsal navicular bone: assessment with MR imaging". Radiology. 195 (3): 849–853. doi:10.1148/radiology.195.3.7754020. PMID 7754020.
- Wilson, Chloe (3 November 2021). "Os Trigonum Syndrome: Causes, Symptoms & Treatment". Foot Pain Explored.
- SCAPINELLI R (1963). "Sesamoid Bones in the Ligamentum Nuchae of Man". J Anat. 97: 417–22. PMC 1244202. PMID 14047360.
- Warner, Jon J.P.; Beim, Gloria M.; Higgins, Laurence (September 1998). "The Treatment of Symptomatic Os Acromiale". The Journal of Bone and Joint Surgery. 80 (9): 1320–6. doi:10.2106/00004623-199809000-00011. PMID 9759817.
- Sammarco, VJ (March 2000). "Os acromiale: frequency, anatomy, and clinical implications". J Bone Joint Surg Am. 82 (3): 394–400. doi:10.2106/00004623-200003000-00010. PMID 10724231.
- Dr Henry Knipe; et al. "Oppenheimer ossicle". Radiopaedia. Retrieved 2017-11-05.