Patellofemoral pain syndrome
Patellofemoral pain syndrome (PFPS; not to be confused with jumper's knee) is knee pain as a result of problems between the kneecap and the femur.[4] The pain is generally in the front of the knee and comes on gradually.[2][4] Pain may worsen with sitting, excessive use, or climbing and descending stairs.[1]
| Patellofemoral pain syndrome | |
|---|---|
| Other names | Patellar overload syndrome, runner's knee,[1] retropatellar pain syndrome[1] |
 | |
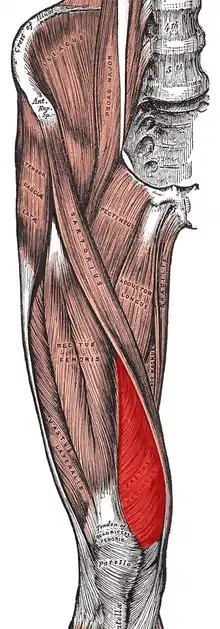
| Diagram of the bones of the lower extremity. Rough distribution of areas affected by PFPS highlighted in red: patella and distal femur. | |
| Specialty | Orthopedics, sports medicine |
| Symptoms | Pain in the front of the knee[1] |
| Usual onset | Gradual[2] |
| Causes | Unclear[1] |
| Risk factors | Trauma, increased training, weak quadriceps muscle[1] |
| Diagnostic method | Based on symptoms and examination[3] |
| Differential diagnosis | Patellar tendinopathy, infrapatellar bursitis, infrapatellar fat pad syndrome, chondromalacia patellae[2] |
| Treatment | Rest, physical therapy[3] |
| Prognosis | May last for years[3] |
| Frequency | Relatively common[2] |
While the exact cause is unclear, it is believed to be due to overuse.[1][2] Risk factors include trauma, increased training, and a weak quadriceps muscle.[1] It is particularly common among runners.[3] The diagnosis is generally based on the symptoms and examination.[3] If pushing the kneecap into the femur increases the pain, the diagnosis is more likely.[1][3]
Treatment typically involves rest and rehabilitation with a Physical Therapist.[5] Runners may need to switch to activities such as cycling or swimming.[3] Insoles may help some people.[3] Symptoms may last for years despite treatment.[3] Patellofemoral pain syndrome is the most common cause of knee pain, affecting more than 20% of young adults.[1][2] It occurs about 2.5 times more often in females than males.[2]
Signs and symptoms
The onset of the condition is usually gradual,[4] although some cases may appear suddenly following trauma.[3] The most common symptom is diffuse vague pain around the kneecap (peripatellar) and localized pain focused behind the kneecap (retropatellar). Affected individuals typically have difficulty describing the location of the pain. They may place their hands over the anterior patella or describe a circle around the patella. This is often called the "circle sign".[3] Pain is usually initiated when weight is put on the knee extensor mechanism, such as when ascending or descending stairs or slopes, squatting, kneeling, cycling, or running.[6][7][8] Pain during prolonged sitting is sometimes termed the "movie sign" or "theatre sign" because individuals might experience pain while sitting to watch a film or similar activity.[6] The pain is typically aching and occasionally sharp. Pain may be exacerbated by activities.[3][9] The knee joint may exhibit noises such as clicking.[6] However, this has no relation to pain and function.[10][11] Giving-way of the knee may be reported.[6] Reduced knee flexion may be experienced during activities.[12]
Causes
In most patients with PFPS an examination of their history will highlight a precipitating event that caused the injury. Changes in activity patterns such as excessive increases in running mileage, repetitions such as running up steps and the addition of strength exercises that affect the patellofemoral joint are commonly associated with symptom onset. Excessively worn or poorly fitted footwear may be a contributing factor. To prevent recurrence the causal behaviour should be identified and managed correctly.[3]
The medical cause of PFPS is thought to be increased pressure on the patellofemoral joint.[6] There are several theorized mechanisms relating to how this increased pressure occurs:
- Increased levels of physical activity[6]
- Malalignment of the patella as it moves through the femoral groove[6]
- Quadriceps muscle imbalance[6][13][14]
- Tight anatomical structures, e.g. retinaculum or iliotibial band.[6]
Causes can also be a result of excessive genu valgum and the above-mentioned repetitive motions leading to abnormal lateral patellar tracking. Individuals with genu valgum have larger than normal Q-angles causing the weight-bearing line to fall lateral to the centre of the knee causing overstretching of the MCL and stressing the lateral meniscus and cartilages.
The cause of pain and dysfunction often results from either abnormal forces (e.g. increased pull of the lateral quadriceps retinaculum with acute or chronic lateral PF subluxation/dislocation) or prolonged repetitive compressive or shearing forces (running or jumping) on the PF joint. The result is synovial irritation and inflammation and subchondral bony changes in the distal femur or patella known as "bone bruises". Secondary causes of PF Syndrome are fractures, internal knee derangement, osteoarthritis of the knee and bony tumors in or around the knee.[15]
Diagnosis
Examination
People can be observed standing and walking to determine patellar alignment.[16] The Q-angle, lateral hypermobility, and J-sign are commonly used determined to determine patellar maltracking.[17] The patellofemoral glide, tilt, and grind tests (Clarke's sign), when performed, can provide strong evidence for PFPS.[3][18] Lastly, lateral instability can be assessed via the patellar apprehension test, which is deemed positive when there is pain or discomfort associated with lateral translation of the patella.[3][16] Various clinical tests have been investigated for diagnostic accuracy. The Active Instability Test, knee pain during stair climbing, Clarke's test, pain with prolonged sitting, patellar inferior pole tilt, and pain during squatting have demonstrated the best accuracy.[19] However, careful consideration is still needed when using these tests to make a differential diagnosis of PFPS.[19] Individuals with PFP may be exhibit higher pain level and lower function.[20]
Magnetic resonance imaging rarely can give useful information for managing patellofemoral pain syndrome and treatment should focus on an appropriate rehabilitation program including correcting strength and flexibility concerns.[21] In the uncommon cases where a patient has mechanical symptoms like a locked knee, knee effusion, or failure to improve following physical therapy, then an MRI may give more insight into diagnosis and treatment.[21]
Classification
PFPS is one of a handful of conditions sometimes referred to as runner's knee;[3] the other conditions being chondromalacia patellae, iliotibial band syndrome, and plica syndrome.
Chondromalacia patellae is a term sometimes used synonymously with PFPS.[6] However, there is general consensus that PFPS applies only to individuals without cartilage damage,[6] thereby distinguishing it from chondromalacia patellae, a condition with softening of the patellar articular cartilage.[3] Despite this distinction, the diagnosis of PFPS is typically made based only on the history and physical examination rather than on the results of any medical imaging. Therefore, it is unknown whether most persons with a diagnosis of PFPS have cartilage damage or not, making the difference between PFPS and chondromalacia theoretical rather than practical.[6] It is thought that only some individuals with anterior knee pain will have true chondromalacia patellae.[3]
Differential diagnosis
The diagnosis of patellofemoral pain syndrome is made by ruling out patellar tendinitis, prepatellar bursitis, plica syndrome, Sinding-Larsen and Johansson syndrome, and Osgood–Schlatter disease.[22] Currently, there is not a gold standard assessment to diagnose PFPS.[19]
Treatment
A variety of treatments for patellofemoral pain syndrome are available.[23] Most people respond well to conservative therapy.[23][24][13]
Exercises
Patellofemoral pain syndrome may also result from overuse or overload of the PF joint. For this reason, knee activity should be reduced until the pain is resolved.[25][26]
There is consistent but low quality evidence that exercise therapy for PFPS reduces pain, improves function and aids long-term recovery.[27] However, there is insufficient evidence to compare the effectiveness of different types of exercises with each other, and exercises with other forms of treatment.[27]
Exercise therapy is the recommended first line treatment of PFPS.[3] Various exercises have been studied and recommended.[28] Exercises are described according to 3 parameters:[7]
- Type of muscle activity (concentric, eccentric or isometric)
- Type of joint movement (dynamic, isometric or static)
- Reaction forces (closed or open kinetic chain)
The majority of exercise programs intended to treat PFPS are designed to strengthen the quadriceps muscles,[7] because their weakness and quadriceps muscle imbalance may contribute to abnormal patellar tracking. [23] If the strength of the vastus medialis muscle is inadequate, the usually larger and stronger vastus lateralis muscle will pull sideways (laterally) on the kneecap. Strengthening the vastus medialis to prevent or counter the lateral force of the vastus lateralis is one way of relieving PFPS, however it is hard to isolate and strengthen only one muscle of quadriceps.
Also, there is growing evidence that shows proximal factors play a much larger role than vastus medialis (VMO) strength deficits or quadriceps imbalance.[29] Hip abductor, extensor, and external rotator strengthening may help.[30] Emphasis during exercise may be placed on coordinated contraction of the medial and lateral parts of the quadriceps as well as of the hip adductor, hip abductor and gluteal muscles.[7] Many exercise programs include stretches designed to improve lower limb flexibility.[7]
Electromyographic biofeedback allows visualization of specific muscle contractions and may help individuals performing the exercises to target the intended muscles during the exercise.[7] Neuromuscular electrical stimulation to strengthen quadracep muscles is sometimes suggested, however the effectiveness of this treatment is not certain.[31]
Inflexibility has often been cited as a source of patellofemoral pain syndrome. Stretching of the lateral knee has been suggested to help.[32]
Knee and lumbar joint mobilization are not recommended as primary interventions for PFPS. It can be used as combination intervention, but as we continue to promote use of active and physical interventions for PFPS, passive interventions such as joint mobilizations are not recommended.[33]
Manual therapy
Manual therapy in addition to exercises helps in reducing pain, improving function, and knee range of motion in patients with PFPS. Manual therapy such as patellar joint mobilization, manipulation and soft tissue mobilization along with Physical therapy exercises is found to be effective in treating PFPS. However, there is not enough evidence that supports lumbopelvic spine manipulation has any effect on the quadriceps muscle activation to improve function & reduce pain.[34]
Medication
Non-steroidal anti-inflammatory drugs (NSAIDs) are widely used to treat PFPS; however, there is only very limited evidence that they are effective.[6] NSAIDs may reduce pain in the short term; overall, however, after three months pain is not improved.[35] There is no evidence that one type of NSAID is superior to another in PFPS, and therefore some authors have recommended that the NSAID with fewest side effects and which is cheapest should be used.[6]
Glycosaminoglycan polysulfate (GAGPS) inhibits proteolytic enzymes and increases synthesis and degree of polymerization of hyaluronic acid in synovial fluid.[6] There is contradictory evidence that it is effective in PFPS.[6]
Braces and taping
There is no difference in pain symptoms between taping and non-taping in individuals with PFPS.[35] Although taping alone is not shown to reduce pain, studies show that taping in conjunction with therapeutic exercise can have a significant effect on pain reduction.[36]
Knee braces are ineffective in treating PFPS.[35] The technique of McConnell taping involves pulling the patella medially with tape (medial glide). Findings from some studies suggest that there is limited benefit with patella taping or bracing when compared to quadriceps exercises alone.[23] There is a lack of evidence to show that knee braces, sleeves, or straps are effective.[37]
Insoles
Low arches can cause overpronation or the feet to roll inward too much increasing load on the patellofemoral joint. Poor lower extremity biomechanics may cause stress on the knees and can be related to the development of patellofemoral pain syndrome, although the exact mechanism linking joint loading to the development of the condition is not clear. Foot orthoses can help to improve lower extremity biomechanics and may be used as a component of overall treatment.[38][39] Foot orthoses may be useful for reducing knee pain in the short term,[40] and may be combined with exercise programs or physical therapy. However, there is no evidence supporting use of combined exercise with foot orthoses as intervention beyond 12 months for adults. Evidence for long term use of foot orthoses for adolescents is uncertain. No evidence supports use of custom made foot orthoses.[33]
Surgery
The scientific consensus is that surgery should be avoided except in very severe cases in which conservative treatments fail.[6] The majority of individuals with PFPS receive nonsurgical treatment.[7]
Alternative medicine
The use of electrophysical agents and therapeutic modalities are not recommended as passive treatments should not be the focus of the plan of care.[41] There is no evidence to support the use of acupuncture or low-level laser therapy.[42] Most studies claiming benefits of alternative therapies for PFPS were conducted with flawed experimental design, and therefore did not produce reliable results.[43]
Prognosis
Patellarfemoral pain syndrome can become a chronic injury, with an estimated 50% of people reporting persistent patellar-femoral pain after a year.[31] Risk factors for a prolonged recovery (or persistent condition) include age (older athletes), females, increased body weight, a reduction in muscle strength, time to seek care, and in those who experience symptoms for more than two months.[31]
Epidemiology
Patellofemoral pain syndrome is the most common cause of anterior knee pain in the outpatient.[3][44] Specific populations at high risk of primary PFPS include runners, bicyclists, basketball players, young athletes and females.[45]
BMI did not significantly increase risk of developing PFPS in adolescents. However, adults with PFPS have higher BMI than those without. It is suggested that higher BMI is associated with limited physical activity in people with PFPS as physical activity levels decrease as a result of pain associated with the condition. However, no longitudinal studies are able to show that BMI can be a predictor of development or progression of the condition.[46]
References
- Ferri, Fred F. (2016). Ferri's Clinical Advisor 2017 E-Book: 5 Books in 1. Elsevier Health Sciences. p. 936.e6. ISBN 9780323448383.
- Dutton, RA; Khadavi, MJ; Fredericson, M (February 2016). "Patellofemoral Pain". Physical Medicine and Rehabilitation Clinics of North America. 27 (1): 31–52. doi:10.1016/j.pmr.2015.08.002. PMID 26616176.
- Dixit S, DiFiori JP, Burton M, Mines B (January 2007). "Management of patellofemoral pain syndrome". American Family Physician. 75 (2): 194–202. PMID 17263214.
- Callaghan MJ, Selfe J (April 2012). "Patellar taping for patellofemoral pain syndrome in adults". The Cochrane Database of Systematic Reviews. 4 (4): CD006717. doi:10.1002/14651858.CD006717.pub2. PMID 22513943.
- "Patellofemoral pain syndrome - Diagnosis and treatment - Mayo Clinic". Mayo Clinic. Retrieved 17 May 2022.
- Heintjes E, Berger MY, Bierma-Zeinstra SM, Bernsen RM, Verhaar JA, Koes BW (2004). "Pharmacotherapy for patellofemoral pain syndrome". The Cochrane Database of Systematic Reviews. 2008 (3): CD003470. doi:10.1002/14651858.CD003470.pub2. PMC 8276350. PMID 15266488.
- van der Heijden RA, Lankhorst NE, van Linschoten R, Bierma-Zeinstra SM, van Middelkoop M (2013). "Exercise for treating patellofemoral pain syndrome (Protocol)". Cochrane Database of Systematic Reviews. 2: CD010387. doi:10.1002/14651858.CD010387.
- Smith TO, Drew BT, Meek TH, Clark AB (2013). "Knee orthoses for treating patellofemoral pain syndrome (Protocol)". Cochrane Database of Systematic Reviews. 5: CD010513. doi:10.1002/14651858.CD010513.
- Pazzinatto MF, de Oliveira Silva D, Barton C, Rathleff MS, Briani RV, de Azevedo FM (October 2016). "Female Adults with Patellofemoral Pain Are Characterized by Widespread Hyperalgesia, Which Is Not Affected Immediately by Patellofemoral Joint Loading". Pain Medicine. 17 (10): 1953–1961. doi:10.1093/pm/pnw068. PMID 27113220.
- de Oliveira Silva D, Pazzinatto MF, Priore LB, Ferreira AS, Briani RV, Ferrari D, Bazett-Jones D, Azevedo FM (September 2018). "Knee crepitus is prevalent in women with patellofemoral pain, but is not related with function, physical activity and pain". Physical Therapy in Sport. 33: 7–11. doi:10.1016/j.ptsp.2018.06.002. hdl:11449/179928. PMID 29890402. S2CID 48352699.
- de Oliveira Silva D, Barton C, Crossley K, Waiteman M, Taborda B, Ferreira AS, Azevedo FM (September 2018). "Implications of knee crepitus to the overall clinical presentation of women with and without patellofemoral pain". Physical Therapy in Sport. 33: 89–95. doi:10.1016/j.ptsp.2018.07.007. hdl:11449/180174. PMID 30059950. S2CID 51894366.
- Silva D, Briani RV, Pazzinatto MF, Ferrari D, Aragão FA, Azevedo FM (November 2015). "Reduced knee flexion is a possible cause of increased loading rates in individuals with patellofemoral pain". Clinical Biomechanics. 30 (9): 971–5. doi:10.1016/j.clinbiomech.2015.06.021. PMID 26169602.
- Briani RV, De Oliveira Silva D, Flóride CS, Aragão FA, de Albuquerque CE, Magalhães FH, de Azevedo FM (2018). "Quadriceps neuromuscular function in women with patellofemoral pain: Influences of the type of the task and the level of pain". PLOS ONE. 13 (10): e0205553. Bibcode:2018PLoSO..1305553B. doi:10.1371/journal.pone.0205553. PMC 6179260. PMID 30304030.
- Willy RW, et al. (2019). "Patellofemoral Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Academy of Orthopaedic Physical Therapy of the American Physical Therapy Association". Journal of Orthopaedic & Sports Physical Therapy. 49 (9): CPG1–CPG95. doi:10.2519/jospt.2019.0302. PMID 31475628.
- Plamondon, Tom (12 Aug 2009). "Special tests in the clinical examination of patellofemoral syndrome". Doctors Lounge. 09 (8): 287. Retrieved 2012-08-20.
- Sarwark JF (2010). Essentials of musculoskeletal care. Rosemont, Ill.: American Academy of Orthopaedic Surgeons. ISBN 9780892035793. OCLC 706805938.
- Sheehan FT, Derasari A, Fine KM, Brindle TJ, Alter KE (January 2010). "Q-angle and J-sign: indicative of maltracking subgroups in patellofemoral pain". Clinical Orthopaedics and Related Research. 468 (1): 266–75. doi:10.1007/s11999-009-0880-0. PMC 2795830. PMID 19430854.
- Malanga G, Nadler S (2006). Musculoskeletal physical examination : an evidence-based approach. Philadelphia, Penns.: Elsevier Mosby. pp. 302–304. ISBN 9781560535911.
- Cook C, Mabry L, Reiman MP, Hegedus EJ (June 2012). "Best tests/clinical findings for screening and diagnosis of patellofemoral pain syndrome: a systematic review". Physiotherapy. 98 (2): 93–100. doi:10.1016/j.physio.2011.09.001. PMID 22507358.
- Ferreira AS, Silva DO, Priore LB, Garcia CL, Ducatti MH, Botta AF, Waiteman MC, Azevedo FM (2018). "Differences in pain and function between adolescent athletes and physically active non-athletes with patellofemoral pain". Physical Therapy in Sport. 33: 70–75. doi:10.1016/j.ptsp.2018.07.005. hdl:11449/171444. PMID 30025378. S2CID 51701050.
- American Medical Society for Sports Medicine (24 April 2014), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American Medical Society for Sports Medicine, retrieved 29 July 2014, which cites
- Prins MR, van der Wurff P (2009). "Females with patellofemoral pain syndrome have weak hip muscles: a systematic review". The Australian Journal of Physiotherapy. 55 (1): 9–15. doi:10.1016/S0004-9514(09)70055-8. PMID 19226237.
- Bolgla LA, Boling MC (June 2011). "An update for the conservative management of patellofemoral pain syndrome: a systematic review of the literature from 2000 to 2010". International Journal of Sports Physical Therapy. 6 (2): 112–25. PMC 3109895. PMID 21713229.
- Earl JE, Vetter CS (August 2007). "Patellofemoral pain". Physical Medicine and Rehabilitation Clinics of North America. 18 (3): 439–58, viii. doi:10.1016/j.pmr.2007.05.004. PMID 17678761.
- Thomeé R, Renström P, Karlsson J, Grimby G (August 1995). "Patellofemoral pain syndrome in young women. I. A clinical analysis of alignment, pain parameters, common symptoms and functional activity level". Scandinavian Journal of Medicine & Science in Sports. 5 (4): 237–44. doi:10.1111/j.1600-0838.1995.tb00040.x. PMID 7552769. S2CID 46457854.
- Tria AJ, Palumbo RC, Alicea JA (October 1992). "Conservative care for patellofemoral pain". The Orthopedic Clinics of North America. 23 (4): 545–54. doi:10.1016/S0030-5898(20)31770-3. PMID 1408039.
- van der Heijden RA, Lankhorst NE, van Linschoten R, Bierma-Zeinstra SM, van Middelkoop M (January 2015). "Exercise for treating patellofemoral pain syndrome". The Cochrane Database of Systematic Reviews. 1: CD010387. doi:10.1002/14651858.CD010387.pub2. PMID 25603546.
- van der Heijden, Rianne A; Lankhorst, Nienke E; van Linschoten, Robbart; Bierma-Zeinstra, Sita MA; van Middelkoop, Marienke; van Middelkoop, Marienke (2013). Van Middelkoop, Marienke (ed.). "Exercise for treating patellofemoral pain syndrome". Reviews. doi:10.1002/14651858.CD010387.
- de Oliveira Silva D, Barton CJ, Pazzinatto MF, Briani RV, de Azevedo FM (June 2016). "Proximal mechanics during stair ascent are more discriminate of females with patellofemoral pain than distal mechanics". Clinical Biomechanics. 35: 56–61. doi:10.1016/j.clinbiomech.2016.04.009. PMID 27128766.
- Powers, CM (February 2010). "The influence of abnormal hip mechanics on knee injury: a biomechanical perspective". The Journal of Orthopaedic and Sports Physical Therapy. 40 (2): 42–51. doi:10.2519/jospt.2010.3337. PMID 20118526.
- Martimbianco, Ana Luiza C.; Torloni, Maria Regina; Andriolo, Brenda Ng; Porfírio, Gustavo Jm; Riera, Rachel (2017-12-12). "Neuromuscular electrical stimulation (NMES) for patellofemoral pain syndrome". The Cochrane Database of Systematic Reviews. 12 (12): CD011289. doi:10.1002/14651858.CD011289.pub2. ISSN 1469-493X. PMC 6486051. PMID 29231243.
- Zaffagnini S, Dejour D, Arendt EA (2010). Patellofemoral pain, instability, and arthritis clinical presentation, imaging, and treatment. Berlin: Springer. p. 134. ISBN 9783642054242.
- Collins NJ, Barton CJ, van Middelkoop M, Callaghan MJ, Rathleff MS, Vicenzino BT, Davis IS, Powers CM, Macri EM, Hart HF, de Oliveira Silva D, Crossley KM (September 2018). "2018 Consensus statement on exercise therapy and physical interventions (orthoses, taping and manual therapy) to treat patellofemoral pain: recommendations from the 5th International Patellofemoral Pain Research Retreat, Gold Coast, Australia, 2017". British Journal of Sports Medicine. 52 (18): 1170–1178. doi:10.1136/bjsports-2018-099397. PMID 29925502.
- Espí-López, Gemma Victoria; Arnal-Gómez, Anna; Balasch-Bernat, Mercè; Inglés, Marta (June 2017). "Effectiveness of Manual Therapy Combined With Physical Therapy in Treatment of Patellofemoral Pain Syndrome: Systematic Review". Journal of Chiropractic Medicine. 16 (2): 139–146. doi:10.1016/j.jcm.2016.10.003. ISSN 1556-3707. PMC 5440631. PMID 28559754.
- Rodriguez-Merchan EC (March 2014). "Evidence Based Conservative Management of Patello-femoral Syndrome". The Archives of Bone and Joint Surgery. 2 (1): 4–6. PMC 4151435. PMID 25207305.
- Logan CA, Bhashyam AR, Tisosky AJ, Haber DB, Jorgensen A, Roy A, Provencher MT (September 2017). "Systematic Review of the Effect of Taping Techniques on Patellofemoral Pain Syndrome". Sports Health. 9 (5): 456–461. doi:10.1177/1941738117710938. PMC 5582697. PMID 28617653.
- Smith TO, Drew BT, Meek TH, Clark AB (December 2015). "Knee orthoses for treating patellofemoral pain syndrome" (PDF). The Cochrane Database of Systematic Reviews. 2015 (12): CD010513. doi:10.1002/14651858.CD010513.pub2. PMC 8763348. PMID 26645724.
- Gross ML, Davlin LB, Evanski PM (1991). "Effectiveness of orthotic shoe inserts in the long-distance runner". The American Journal of Sports Medicine. 19 (4): 409–12. doi:10.1177/036354659101900416. PMID 1897659. S2CID 23550947.
- Eng JJ, Pierrynowski MR (February 1993). "Evaluation of soft foot orthotics in the treatment of patellofemoral pain syndrome". Physical Therapy. 73 (2): 62–8, discussion 68–70. doi:10.1093/ptj/73.2.62. PMID 8421719. S2CID 24645828.
- Hossain M, Alexander P, Burls A, Jobanputra P (January 2011). "Foot orthoses for patellofemoral pain in adults". The Cochrane Database of Systematic Reviews (1): CD008402. doi:10.1002/14651858.CD008402.pub2. PMID 21249707.
- Collins NJ, Barton CJ, van Middelkoop M, Callaghan MJ, Rathleff MS, Vicenzino BT, Davis IS, Powers CM, Macri EM, Hart HF, de Oliveira Silva D, Crossley KM (September 2018). "2018 Consensus statement on exercise therapy and physical interventions (orthoses, taping and manual therapy) to treat patellofemoral pain: recommendations from the 5th International Patellofemoral Pain Research Retreat, Gold Coast, Australia, 2017". British Journal of Sports Medicine. 52 (18): 1170–1178. doi:10.1136/bjsports-2018-099397. PMID 29925502.
- Crossley K, Bennell K, Green S, McConnell J (April 2001). "A systematic review of physical interventions for patellofemoral pain syndrome". Clinical Journal of Sport Medicine. 11 (2): 103–10. doi:10.1097/00042752-200104000-00007. PMID 11403109. S2CID 22097250.
- Bizzini M, Childs JD, Piva SR, Delitto A (January 2003). "Systematic review of the quality of randomized controlled trials for patellofemoral pain syndrome". The Journal of Orthopaedic and Sports Physical Therapy. 33 (1): 4–20. doi:10.2519/jospt.2003.33.7.F4. PMID 12570282.
- Lack S, Neal B, De Oliveira Silva D, Barton C (July 2018). "How to manage patellofemoral pain - Understanding the multifactorial nature and treatment options". Physical Therapy in Sport. 32: 155–166. doi:10.1016/j.ptsp.2018.04.010. hdl:11449/171014. PMID 29793124. S2CID 46921956.
- Atanda A, Reddy D, Rice JA, Terry MA (November 2009). "Injuries and chronic conditions of the knee in young athletes". Pediatrics in Review. 30 (11): 419–28, quiz 429–30. doi:10.1542/pir.30-11-419. PMID 19884282. S2CID 23042353.
- Hart HF, Barton CJ, Khan KM, Riel H, Crossley KM (May 2017). "Is body mass index associated with patellofemoral pain and patellofemoral osteoarthritis? A systematic review and meta-regression and analysis". British Journal of Sports Medicine. 51 (10): 781–790. doi:10.1136/bjsports-2016-096768. PMID 27927675. S2CID 40935953.