Piperaquine
Piperaquine is an antiparasitic drug used in combination with dihydroartemisinin to treat malaria. Piperaquine was developed under the Chinese National Malaria Elimination Programme in the 1960s and was adopted throughout China as a replacement for the structurally similar antimalarial drug chloroquine. Due to widespread parasite resistance to piperaquine, the drug fell out of use as a monotherapy, and is instead used as a partner drug for artemisinin combination therapy. Piperaquine kills parasites by disrupting the detoxification of host heme.
 | |
| Clinical data | |
|---|---|
| ATC code | |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| ChEBI | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| Chemical and physical data | |
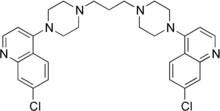
| Formula | C29H32Cl2N6 |
| Molar mass | 535.52 g·mol−1 |
| 3D model (JSmol) | |
| Melting point | 199 to 204 °C (390 to 399 °F) (dec.V |
| |
| |
| | |
Medical uses
Piperaquine is used in combination with dihydroartemisinin for the treatment of malaria.[1] This combination is one of several artemisinin combination therapies recommended by the World Health Organization for treatment of uncomplicated malaria.[1] This combination is also recommended by the World Health Organization for treatment of severe malaria after administration of artesunate.[1]
Piperaquine is also registered for use in some countries in combination with arterolane.[1] However, this combination is not recommended by the World Health Organization due to insufficient data.[1]
Contraindications
Like chloroquine, piperaquine can prolong the QT interval. Although large randomized clinical trials have not revealed evidence of cardiotoxicity, the World Health Organization recommends not using piperaquine in patients with congenital QT prolongation or who are on other drugs that prolong the QT interval.[1]
Pharmacology
Mechanism of action
Like chloroquine, piperaquine is thought to function by accumulating in the parasite digestive vacuole and interfering with the detoxification of heme into hemozoin.[2]
Resistance
Parasites that survive piperaquine treatment have been increasingly reported since 2010, particularly in Southeast Asia. The epicenter of piperaquine resistance appears to be western Cambodia where in 2014 over 40% of dihydroartemisinin-piperaquine treatments failed to eliminate parasites from the patient's blood.[3] Characterizing piperaquine-resistant parasites has been technically challenging, as parasites that survive piperaquine treatment in patients appear to remain sensitive to piperaquine in vitro; i.e. piperaquine appears to have the same IC50 in sensitive parasites and resistant parasites.[3]
The mechanism by which parasites become resistant to piperaquine remains unclear. Amplification of the parasite proteases plasmepsin 2 and plasmepsin 3, both involved in degrading host hemoglobin, is associated with resistance to piperaquine.[4] Similarly, mutations in a gene related to chloroquine resistance, PfCRT, have been associated with piperaquine resistance; however, parasites that are resistant to chloroquine remain sensitive to piperaquine.[4][3] In contrast, amplification of the gene for the parasite transporter PfMDR1, a mechanism of parasite resistance to mefloquine, is inversely correlated with piperaquine resistance.[3]
Pharmacokinetics
Piperaquine is a lipophilic drug and therefore is rapidly absorbed and distributed across much of the body.[2] The drug reaches its maximal concentrations approximately 2 hours after administration.[2]
Chemistry
Piperaquine is available as a base, and as a water-soluble tetraphosphate salt.[5]
History
Piperaquine was discovered in the 1960s by two separate groups working independently of one another: the Shanghai Pharmaceutical Industry Research Institute in China and the Rhone Poulenc in France.[5] In the 1970s and 1980s piperaquine became the primary antimalarial drug of the Chinese National Malaria Control Programme due to increased parasite resistance to chloroquine.[2] By the late 1980s, the use of piperaquine as an antimalarial monotherapy diminished as increasing parasite resistance to piperaquine was observed.[5] Beginning in the 1990s, piperaquine was tested and adopted as a partner drug for artemisinin combination therapy.[5]
References
- Guidelines for the Treatment of Malaria (PDF) (3 ed.). WHO. 2015. p. 33-34. Retrieved 22 May 2018.
- Eastman RT, Fidock DA (2009). "Artemisinin-based combination therapies: a vital tool in efforts to eliminate malaria". Nature Reviews Microbiology. 7 (12): 864–874. doi:10.1038/nrmicro2239. PMC 2901398. PMID 19881520.
- Duru V, Witkowski B, Menard D (2016). "Plasmodium falciparum resistance to artemisinin derivatives and piperaquine: a major challenge for malaria elimination in Cambodia". The American Journal of Tropical Medicine and Hygiene. 95 (6): 1228–1238. doi:10.4269/ajtmh.16-0234. PMC 5154433. PMID 27928074.
- Haldar K, Bhattacharjee S, Safeukui I (2018). "Drug resistance in Plasmodium". Nature Reviews Microbiology. 16 (3): 156–170. doi:10.1038/nrmicro.2017.161. PMC 6371404. PMID 29355852.
- Davis TM, Hung TY, Sim IK, Karunajeewa HA, Ilett KF (2005). "Piperaquine: a resurgent antimalarial drug". Drugs. 65 (1): 75–87. doi:10.2165/00003495-200565010-00004. PMID 15610051.