Stages of death
The stages of death of a human being have medical, biochemical and legal aspects. The term taphonomy from palaeontology applies to the fate of all kinds of remains of organisms. Forensic taphonomy is concerned with remains of the human body.[1]
| Stages of death |
|---|
History
The academic study of death is called thanatology, a field pioneered by Élie Metchnikoff in the early 20th century. Thanatology focuses on describing postmortem bodily modifications, as well as perspectives concerning psychosocial, medical, ethical, and spiritual aspects of death.
Definition of death
Prior to the 1980s, the legal standard defined death as the absence of cardiopulmonary function including the loss of all vital signs.[2] However, as medical technology advanced, there were situations where one might lose brain function and maintain cardiopulmonary function.[3] This led the American Medical Association, the American Bar Association in collaboration with the National Conference of Commissioners on Uniform State Laws to come together in the 1980s to expand the definition of death through the Uniform Determination of Death Act (UDDA).[3] Under this law, death can be defined as the loss of cardiopulmonary function or the loss of brain function including the brainstem and cortex.
Clinical signs and stages of death
Signs of death or strong indications that a warm-blooded animal is no longer alive are:
- Respiratory arrest (no breathing)
- Cardiac arrest (no pulse)
- Brain death (no neuronal activity)
The heart and lungs are vital organs for human life due to their ability to properly oxygenate human blood (lungs) and distribute this blood to all vital organs (heart). Hence failure of the heart to pump blood or the lungs to obtain oxygen can lead to a cardiopulmonary death where the heart stops pumping and there is no pulse. In the brain, this can be manifested by a hypoxic state which leads to cerebral edema and thus an increase in intracranial pressure. The rise in intracranial pressure can lead to further disruption in cerebral blood flow, leading to necrosis or tissue death.[4] The aforementioned mechanism is the most common cause of brain death, however this increase in intracranial pressure does not always occur due to an arrest in cardiopulmonary function.[5] Traumatic brain injuries and subarachnoid hemorrhages can also increase the intracranial pressure in the brain leading to a cessation of brain function and hence death.[6] While cardiopulmonary death can be easily assessed by looking for the presence of a pulse, or identifying electrical activity through EKG tracings, assessment of brain death is slightly more nuanced. Per the United Kingdom Medical Royal Colleges, a diagnosis of brain death is a two-fold process including 1) identifying the cause of irreversible brain damage and excluding reversible causes of brain damage and 2) conducting a series of clinical and laboratory tests to assess brain stem function.[7][8]
The definition of legal death, and its formal documentation in a death certificate, vary according to the jurisdiction. The certification applies to somatic death, corresponding to death of the person, which has varying definitions but most commonly describes a lack of vital signs and brain function.[9] Death at the level of cells, called molecular death or cell death, follows a matter of hours later.[10] These distinctions, and the independence of physicians certifying legal death, are significant in organ procurement.[11]
Post-mortem changes
.png.webp)
Post-mortem changes refer to the series of changes that occur to a body after death. These changes can generally be divided between early post-mortem changes and late post-mortem changes (also known as decomposition).[12] These changes occur along a continuum and can be helpful in determining the post-mortem interval, which is the time between death and examination.
The stages that follow shortly after death are:
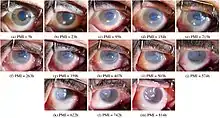
- Corneal opacity or "clouding"
- Pallor mortis, paleness which happens in the first 15–120 minutes after death
- Algor mortis, the reduction in body temperature following death. This is generally a steady decline until matching ambient temperature
- Rigor mortis, the limbs of the corpse become stiff (Latin rigor) and difficult to move or manipulate
- Livor mortis, or dependent lividity, a settling of the blood in the lower (dependent) portion of the body
- Putrefaction, the beginning signs of decomposition
Of these, with obvious mortal damage to the body, the textbook conclusive signs of death clear to a lay person are: algor mortis, rigor mortis, livor mortis, and putrefaction.[13]
The cardinal signs of death may refer to the ending of breathing, heartbeat and circulation, or to algor mortis, livor mortis and rigor mortis; the adoption of brain death as a definition has lessened the centrality of these signs.[14][12] In a clearer contemporary terminology, algor mortis, livor mortis and rigor mortis are called "early postmortem" changes, in distinction from the "immediate postmortem" changes associated with the cessation of bodily functions, as indicated by vital signs.[15] With an ophthalmoscope, changes to the blood in the retina are quickly visible.[16]
Those stages are followed, in taphonomy, by
- Decomposition, the reduction into simpler forms of matter, accompanied by a strong, unpleasant odor.
- Skeletonization, the end of decomposition, where all soft tissues have decomposed, leaving only the skeleton.
- Fossilization, the natural preservation of the skeletal remains formed over a very long period. This stage may not occur, depending on the circumstances and the conditions of the surrounding environment.
Decomposition stages
Descriptions of decomposition have had varying numbers of discrete stages. A 5-stage process developed by Galloway and colleagues that is commonly used in forensic pathology is detailed below:[17][18]
- Stage 1: Fresh – about half of bodies show signs of lividity and no signs of insects.
- Stage 2: Early Decomposition – Bacteria grow throughout the body, releasing gases, including cadaverine, which in turn bloat the body and cause an unpleasant odor.
- Stage 3: Advanced Decomposition – This stage brings further discoloration to the body. The gases from bacterial decay begin to escape, causing a strong odor.
- Stage 4: Skeletonization – The internal organs liquefy and the body begins to dry out.
- Stage 5: Extreme Decomposition – Advancing of the skeletonization with bleaching, exfoliation, and loss of wide portions of long bone.
References
- Sorg, Marcella H.; Haglund, William D. (13 December 1996). Forensic Taphonomy: The Postmortem Fate of Human Remains. CRC Press. p. 13. ISBN 978-1-4398-2192-3.
- Sarbey, Ben (1 December 2016). "Definitions of death: brain death and what matters in a person". Journal of Law and the Biosciences. 3 (3): 743–752. doi:10.1093/jlb/lsw054. ISSN 2053-9711. PMC 5570697. PMID 28852554.
- Smit, Hans (1962). "The Uniform Interstate and International Procedure Act Approved by the National Conference of Commissioners on Uniform State Laws: A New Era Commences". The American Journal of Comparative Law. 11 (3): 415–417. doi:10.2307/838593. ISSN 0002-919X. JSTOR 838593.
- Machado, Calixto (25 February 2010). "Diagnosis of brain death". Neurology International. 2 (1): 2. doi:10.4081/ni.2010.e2. ISSN 2035-8377. PMC 3093212. PMID 21577338.
- Spinello, Irene M. (September 2015). "Brain Death Determination". Journal of Intensive Care Medicine. 30 (6): 326–337. doi:10.1177/0885066613511053. ISSN 0885-0666. PMID 24227449. S2CID 39103031.
- Wijdicks, Eelco F.M. (May 1995). "Determining brain death in adults [RETIRED]". Neurology. 45 (5): 1003–1011. doi:10.1212/wnl.45.5.1003. ISSN 0028-3878. PMID 7746373.
- "Diagnosis of death. Memorandum issued by the honorary secretary of the Conference of Medical Royal Colleges and their Faculties in the United Kingdom on 15 January 1979". BMJ. 1 (6159): 332. 3 February 1979. doi:10.1136/bmj.1.6159.332. ISSN 0959-8138. PMC 1597667. PMID 421104.
- "Diagnosis of brain death. Statement issued by the honorary secretary of the Conference of Medical Royal Colleges and their Faculties in the United Kingdom on 11 October 1976". BMJ. 2 (6045): 1187–1188. 13 November 1976. doi:10.1136/bmj.2.6045.1187. ISSN 0959-8138. PMC 1689565. PMID 990836.
- Shedge, Rutwik; Krishan, Kewal; Warrier, Varsha; Kanchan, Tanuj (2021), "Postmortem Changes", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30969563, retrieved 13 September 2021
- Bardale, Rajesh (October 2011). Principles of Forensic Medicine & Toxicology. Wife Goes On. p. 133. ISBN 978-93-5025-493-6.
- Peitzman, Andrew B.; Rhodes, Michael; Schwab, C. William (2008). The Trauma Manual: Trauma and Acute Care Surgery. Lippincott Williams & Wilkins. p. 415. ISBN 978-0-7817-6275-5.
- Prahlow, Joseph A. (10 March 2010). Forensic Pathology for Police, Death Investigators, Attorneys, and Forensic Scientists. Springer Science & Business Media. p. 163. ISBN 978-1-59745-404-9.
- Pollak, Andrew N.; Browner, Bruce D.; Surgeons, American Academy of Orthopaedic (2002). Emergency Care and Transportation of the Sick and Injured. Jones & Bartlett Learning. p. 19. ISBN 978-0-7637-2046-9.
- Fox, Renée C. (1981). "The Sting of Death in American Society". Social Service Review. 55 (1): 47–48. doi:10.1086/643890. ISSN 0037-7961. JSTOR 30011444. PMID 10250829. S2CID 33834100.
- Almulhim, Abdulaziz M.; Menezes, Ritesh G. (2020). "Evaluation of Postmortem Changes". StatPearls. StatPearls Publishing. PMID 32119351.
- Saukko, Pekka; Knight, Bernard (4 November 2015). Knight's Forensic Pathology. CRC Press. p. 57. ISBN 978-1-4441-6508-1.
- Wescott, Daniel J. (13 August 2018). "Recent advances in forensic anthropology: decomposition research". Forensic Sciences Research. 3 (4): 327–342. doi:10.1080/20961790.2018.1488571. ISSN 2096-1790. PMC 6374978. PMID 30788450.
- Forensic taphonomy : the postmortem fate of human remains. William D. Haglund, Marcella H. Sorg. Boca Raton: CRC Press. 1997. ISBN 0-8493-9434-1. OCLC 35236386.
{{cite book}}: CS1 maint: others (link)