Pregnancy test
A pregnancy test is used to determine whether a female is pregnant or not. The two primary methods are testing for the female pregnancy hormone (human chorionic gonadotropin (hCG)) in blood or urine using a pregnancy test kit, and scanning with ultrasonography.[1] Testing blood for hCG results in the earliest detection of pregnancy.[2] Almost all pregnant women will have a positive urine pregnancy test one week after the first day of a missed menstrual period.[3]
Types
Human chorionic gonadotropin (hCG)

Identified in the early 20th century, human chorionic gonadotropin (hCG) is a glycoprotein hormone that rises quickly in the first few weeks of pregnancy, typically reaching a peak at 8- to 10-weeks gestational age.[4][5] hCG is produced by what will become the placenta.[6] hCG testing can be performed with a blood (serum) sample (typically done in a medical facility) or with urine (which can be performed in a medical facility or at home). The assays used to detect the presence of hCG in blood or urine are generally reliable and inexpensive. Secretion of hCG can occur as soon as 6 days following ovulation and on average 8–10 days following ovulation; this is the earliest hCG can be detected in a blood sample.[7][5][8] The hCG concentration in blood is higher than in urine. Therefore, a blood test can be positive while the urine test is still negative.[9][10]
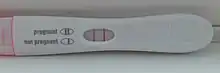
Qualitative tests (yes/no or positive/negative results) look for the presence of the beta subunit of human chorionic gonadotropin (hCG) in blood or urine. For a qualitative test the thresholds for a positive test are generally determined by an hCG cut-off where at least 95% of pregnant women would get a positive result on the day of their first missed period.[11] Qualitative urine pregnancy tests vary in sensitivity. High-sensitivity tests are more common and typically detect hCG levels between 20 and 50 milli-international units/mL (mIU/mL). Low-sensitivity tests detect hCG levels between 1500 and 2000 mIU/mL and have unique clinical applications, including confirmation of medication abortion success.[12] Qualitative urine tests available for home use are typically designed as lateral flow tests.
Quantitative tests measure the exact amount of hCG in the sample. Blood tests can detect hCG levels as low as 1 mIU/mL, and typically clinicians will diagnose a positive pregnancy test at 5mIU/mL.[11]
| Urine pregnancy test | Blood pregnancy test | |
|---|---|---|
| Detection thresholds | High-sensitivity:
Qualitative test: 20 to 50 mIU/mL, depending on test Low-sensitivity: Qualitative test: 1500-2000 mIU/mL, depending on test |
Qualitative test:
5 to 10 mIU/mL, depending on test Quantitative test: 1 to 2 mIU/mL for an ultrasensitive test |
There is a multilevel urine pregnancy test (MLPT) that measures hCG levels semiquantitatively. The hCG levels are measured at <25, 25 to 99, 100 to 499, 500 to 1999, 2000 to 9999, and >10,000 mIU/mL. This test has utility for determining the success of medication abortion.[13][14]
Ultrasound
Obstetric ultrasonography may also be used to detect and diagnose pregnancy. It is very common to have a positive at-home urine pregnancy test before an ultrasound. Both abdominal and vaginal ultrasound may be used, but vaginal ultrasound allows for earlier visualization of the pregnancy. With obstetric ultrasonography the gestational sac (intrauterine fluid collection) can be visualized at 4.5 to 5 weeks gestation, the yolk sac at 5 to 6 weeks gestation, and fetal pole at 5.5 to 6 weeks gestation. Ultrasound is used to diagnose multiple gestation.[3][15]
Accuracy

A systematic review published in 1998 showed that home pregnancy test kits, when used by experienced technicians, are almost as accurate as professional laboratory testing (97.4%). When used by consumers, however, the accuracy fell to 75%: the review authors noted that many users misunderstood or failed to follow the instructions included in the kits.[16]
False positive
False positive pregnancy test results are rare and may occur for several reasons, including:
- user error in performing and interpreting the test,
- biochemical pregnancy (loss of pregnancy before signs of pregnancy are apparent on ultrasound, likely very soon after implantation),
- and non-pregnant production of the hCG molecule (i.e. secretion due to a tumor or the pituitary gland, some diseases of the liver, cancers, including choriocarcinoma and other germ cell tumors, IgA deficiencies, heterophile antibodies, enterocystoplasties, gestational trophoblastic diseases (GTD), and gestational trophoblastic neoplasms).[17][3]
- bacterial contamination and blood in urine[18]
Spurious evaporation lines may appear on many home pregnancy tests if read after the suggested 3–5 minute window or reaction time, independent of an actual pregnancy. False positives may also appear on tests used past their expiration date.[19]
False positive pregnancy test can happen due to 'phantom hCG' which is due to people having human antianimal or heterophilic antibodies.[20]
False positives can also be caused by (in order of incidence) quiescent pregnancy, pituitary sulfated hCG, heterophilic antibody, familial hCG syndrome and cancer.[21]
Due to use of medication
Urine tests can be falsely positive in those that are taking the medications: chlorpromazine, promethazine, phenothiazines, methadone,[18] aspirin, carbamazepine and drugs that cause high urinary pH.[22]
False negative
False negative readings can occur when testing is done too early. hCG levels rise rapidly in early pregnancy and the chances of false negative test results diminish with time (increasing gestational age).[23] Less sensitive urine tests and qualitative blood tests may not detect pregnancy until three or four days after implantation.[24] Menstruation occurs on average 14 days after ovulation, so the likelihood of a false negative is low once a menstrual period is late. Ovulation may not occur at a predictable time in the menstrual cycle. A number of factors may cause an unexpectedly early or late ovulation, even for people with a history of regular menstrual cycles.[25]
More rare, false negative results can also occur due to a "hook effect", where a sample with a very high level of hCG is tested without dilution, causing an invalid result.[26]
Other uses
Pregnancy tests may be used to predict if a pregnancy is likely to continue or is abnormal. Miscarriage, or spontaneous abortion or pregnancy loss, is common in early pregnancy.[27] Serial quantitative blood tests may be done, usually 48 hours apart, and interpreted based on the knowledge that hCG in a viable normal pregnancy rises rapidly in early pregnancy. For example, for a starting hCG level of 1,500 mIU/ml or less, the hCG of continuing, normal pregnancy will increase at least 49% in 48 hours. However, for pregnancies with a higher starting hCG, between 1,500 and 3,000 mIU/ml, the hCG should rise at least 40%; for a starting hCG greater than 3,000 mIU/ml, the hCG should increase at least 33%.[28] Failure to rise by these minimums may indicate that the pregnancy is not normal, either as a failed intrauterine pregnancy or a possible ectopic pregnancy.[28]
Ultrasound is also a common tool for determining viability and location of a pregnancy. Serial ultrasound may be used to identify non-viable pregnancies, as pregnancies that do not grow in size or develop expected structural findings on repeated ultrasounds over a 1-2 week interval may be identified as abnormal.[29] Occasionally, a single ultrasound may be used to identify a pregnancy as non-viable; for example, an embryo that is greater than a certain size but that lacks a visible heart beat may be confidently determined to be not viable without the need for follow up ultrasound for confirmation.[29]
Research
Research has identified at least one other possible marker that may appear earlier and exclusively during pregnancy. For example, early pregnancy factor (EPF) can be detected in blood within 48 hours of fertilization, rather than after implantation.[30] However, its reliable use as a pregnancy test remains unclear as studies have shown its presence in physiological situations besides pregnancy, and its application to humans remains limited.[31]
History
.jpg.webp)
Records of attempts at pregnancy testing have been found as far back as the ancient Greek and ancient Egyptian cultures. The ancient Egyptians watered bags of wheat and barley with the urine of a possibly pregnant woman. Germination indicated pregnancy. The type of grain that sprouted was taken as an indicator of the fetus's sex.[33] Hippocrates suggested that a woman who had missed her period should drink a solution of honey in water at bedtime: resulting abdominal distention and cramps would indicate the presence of a pregnancy. Avicenna and many physicians after him in the Middle Ages performed uroscopy, a nonscientific method to evaluate urine.
Selmar Aschheim and Bernhard Zondek introduced testing based on the presence of human chorionic gonadotropin (hCG) in 1928.[34] Early studies of hCG had concluded that it was produced by the pituitary gland. In the 1930s, Doctor Georgeanna Jones discovered that hCG was produced not by the pituitary gland, but by the placenta. This discovery was important in relying on hCG as an early marker of pregnancy.[35] In the Aschheim and Zondek test, an infantile female mouse was injected subcutaneously with urine of the woman to be tested, and the mouse later was killed and dissected. Presence of ovulation indicated that the urine contained hCG and meant that the subject was pregnant. A similar test was developed using immature rabbits. Here, too, killing the animal to check her ovaries was necessary.
At the beginning of the 1930s, Hillel Shapiro and Harry Zwarenstein, who were researchers at the University of Cape Town, discovered that if urine from a pregnant woman was injected into the South African Xenopus frog and the frog ovulated, this indicated that the subject was pregnant. This test, known as the frog test, was used throughout the world from the 1930s to 1960s, with Xenopus frogs being exported in great numbers.[36][37] Shapiro's advisor, Lancelot Hogben, claimed to have developed the pregnancy test himself, but refuted by both Shapiro and Zwarenstein in a letter to the British Medical Journal. A later article, independently authored, granted Hogben credit for the principle of using Xenopus to determine gonadotropin levels in a pregnant woman's urine, but not for its usage as a functional pregnancy test.[38]
Hormonal pregnancy tests such as Primodos and Duogynon were used in the 1960s and 1970s in the UK and Germany. These tests involved taking a dosed amount of hormones, and observing the response a few days later. A pregnant woman does not react, as she is producing the hormones in pregnancy; a subject who is not pregnant responds to the absence of the hormone by beginning a new menstrual cycle. While the test was (is) generally considered accurate, research advancements have replaced it with simpler techniques.[39]
Immunologic pregnancy tests were introduced in 1960 when Wide and Gemzell presented a test based on in-vitro hemagglutination inhibition. This was a first step away from in-vivo pregnancy testing[40][41] and initiated a series of improvements in pregnancy testing leading to the contemporary at-home testing.[41] Direct measurement of antigens, such as hCG, was made possible after the invention of the radioimmunoassay in 1959.[42] Radioimmunoassays require sophisticated apparatus and special radiation precautions and are expensive.
Organon International obtained the first patent on a home pregnancy test in 1969, two years after product designer Margaret Crane noticed that the laboratory testing procedure was relatively simple and made a prototype. The product became available in Canada in 1971, and the United States in 1977, after delays caused by concerns over sexual morality and the ability of potentially pregnant women to perform the test and cope with the results without a doctor.[43]
Another home pregnancy testing kit was based on the work of Judith Vaitukaitis and Glenn Braunstein, who developed a sensitive hCG assay at the National Institutes of Health.[44][45] That test went onto the market in 1978.[46] In the 1970s, the discovery of monoclonal antibodies led to the development of the relatively simple and cheap immunoassays, such as agglutination-inhibition-based assays and sandwich ELISA, used in modern home pregnancy tests. Tests are now so cheap that they can be mass-produced in a general publication and used for advertising.[47]
See also
References
- Chard, T. (1992). "REVIEW: Pregnancy tests: a review". Human Reproduction. 7 (5): 701–710. doi:10.1093/oxfordjournals.humrep.a137722. ISSN 1460-2350. PMID 1639991.
- Casanova, Robert; Weiss, Patrice M. (April 2018). Beckmann and Ling's obstetrics and gynecology. Casanova, Robert,, Chuang, Alice,, Goepfert, Alice R.,, Hueppchen, Nancy A.,, Weiss, Patrice M.,, American College of Obstetricians and Gynecologists (8th ed.). Philadelphia. ISBN 978-1-4963-5309-2. OCLC 949870151.
{{cite book}}: CS1 maint: location missing publisher (link) - Bastian, Lori A; Brown, Haywood L (November 2019). "Clinical manifestations and diagnosis of early pregnancy". UpToDate.
- Cole, Laurence A (2010). "Biological functions of hCG and hCG-related molecules". Reproductive Biology and Endocrinology. 8 (1): 102. doi:10.1186/1477-7827-8-102. ISSN 1477-7827. PMC 2936313. PMID 20735820.
- Braunstein, G. D.; Rasor, J.; Danzer, H.; Adler, D.; Wade, M. E. (15 November 1976). "Serum human chorionic gonadotropin levels throughout normal pregnancy". American Journal of Obstetrics and Gynecology. 126 (6): 678–681. doi:10.1016/0002-9378(76)90518-4. ISSN 0002-9378. PMID 984142.
- Rhoades, Rodney; Bell, David R., eds. (2009). Medical physiology: principles for clinical medicine (3rd ed.). Philadelphia: Lippincott Williams & Wilkins. ISBN 978-0-7817-6852-8. OCLC 144771424.
- Wilcox, A. J.; Baird, D. D.; Weinberg, C. R. (10 June 1999). "Time of implantation of the conceptus and loss of pregnancy". The New England Journal of Medicine. 340 (23): 1796–1799. doi:10.1056/NEJM199906103402304. ISSN 0028-4793. PMID 10362823.
- Lenton, E. A.; Neal, L. M.; Sulaiman, R. (June 1982). "Plasma concentrations of human chorionic gonadotropin from the time of implantation until the second week of pregnancy". Fertility and Sterility. 37 (6): 773–778. doi:10.1016/s0015-0282(16)46337-5. ISSN 0015-0282. PMID 7115557.
- O'Connor, R. E.; Bibro, C. M.; Pegg, P. J.; Bouzoukis, J. K. (July 1993). "The comparative sensitivity and specificity of serum and urine HCG determinations in the ED". The American Journal of Emergency Medicine. 11 (4): 434–436. doi:10.1016/0735-6757(93)90186-f. ISSN 0735-6757. PMID 8216535.
- Davies, Suzy; Byrn, Francis; Cole, Laurence A. (June 2003). "Human chorionic gonadotropin testing for early pregnancy viability and complications". Clinics in Laboratory Medicine. 23 (2): 257–264, vii. doi:10.1016/s0272-2712(03)00026-x. ISSN 0272-2712. PMID 12848444.
- Gronowski, Ann M., ed. (2004). Handbook of clinical laboratory testing during pregnancy. Totowa, N.J.: Humana Press. ISBN 1-58829-270-3. OCLC 53325293.
- Raymond, Elizabeth G.; Shochet, Tara; Bracken, Hillary (July 2018). "Low-sensitivity urine pregnancy testing to assess medical abortion outcome: A systematic review". Contraception. 98 (1): 30–35. doi:10.1016/j.contraception.2018.03.013. ISSN 0010-7824. PMID 29534996. S2CID 206967147.
- Raymond, Elizabeth G.; Shochet, Tara; Blum, Jennifer; Sheldon, Wendy R.; Platais, Ingrida; Bracken, Hillary; Dabash, Rasha; Weaver, Mark A.; Ngoc, Nguyen Thi Nhu; Blumenthal, Paul D.; Winikoff, Beverly (May 2017). "Serial multilevel urine pregnancy testing to assess medical abortion outcome: a meta-analysis". Contraception. 95 (5): 442–448. doi:10.1016/j.contraception.2016.12.004. ISSN 0010-7824. PMID 28041991.
- Lynd, Kelsey; Blum, Jennifer; Ngoc, Nguyen Thi Nhu; Shochet, Tara; Blumenthal, Paul D.; Winikoff, Beverly (2013). "Simplified medical abortion using a semi-quantitative pregnancy test for home-based follow-up". International Journal of Gynecology & Obstetrics. 121 (2): 144–148. doi:10.1016/j.ijgo.2012.11.022. ISSN 1879-3479. PMID 23477704.
- Woo, Joseph (2006). "Why and when is Ultrasound used in Pregnancy?". Obstetric Ultrasound: A Comprehensive Guide. Retrieved 27 May 2007.
- Bastian LA, Nanda K, Hasselblad V, Simel DL (1998). "Diagnostic efficiency of home pregnancy test kits. A meta-analysis". Arch Fam Med. 7 (5): 465–9. doi:10.1001/archfami.7.5.465. PMID 9755740. Archived from the original on 6 December 2008. Retrieved 12 May 2008.
- Stenman, Ulf-Håkan; Alfthan, Henrik; Hotakainen, Kristina (July 2004). "Human chorionic gonadotropin in cancer". Clinical Biochemistry. 37 (7): 549–561. doi:10.1016/j.clinbiochem.2004.05.008. PMID 15234236.
- Wallach, Jacques (2007). Interpretation of diagnostic tests (8th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 866. ISBN 978-0-7817-3055-6.
- "First Response early result pregnancy test" (PDF). FirstResponse.com.
- Wallach, Jacques (2014). Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (10th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 978-1-4511-9176-9.
- Laurence A. Cole; Stephen A. Butler (2020). 100 Years of Human Chorionic Gonadotropin: Reviews and New Perspectives. Elsevier. p. 87. ISBN 978-0-12-820050-6.
- Betz D, Fane K (2020). "Human Chorionic Gonadotropin". Statpearls. PMID 30422545.
 Text was copied from this source, which is available under a Creative Commons Attribution 4.0 International License.
Text was copied from this source, which is available under a Creative Commons Attribution 4.0 International License. - Wilcox AJ, Baird DD, Weinberg CR (1999). "Time of implantation of the conceptus and loss of pregnancy". New England Journal of Medicine. 340 (23): 1796–1799. doi:10.1056/NEJM199906103402304. PMID 10362823.
- Wilcox AJ, Baird DD, Weinberg CR (June 1999). "Time of implantation of the conceptus and loss of pregnancy". New England Journal of Medicine. 340 (23): 1796–9. doi:10.1056/NEJM199906103402304. PMID 10362823.
- Chard, T. (May 1992). "Pregnancy tests: a review". Human Reproduction (Oxford, England). 7 (5): 701–710. doi:10.1093/oxfordjournals.humrep.a137722. ISSN 0268-1161. PMID 1639991.
- Griffey, Richard T.; Trent, Caleb J.; Bavolek, Rebecca A.; Keeperman, Jacob B.; Sampson, Christopher; Poirier, Robert F. (January 2013). ""Hook-like effect" causes false-negative point-of-care urine pregnancy testing in emergency patients". The Journal of Emergency Medicine. 44 (1): 155–160. doi:10.1016/j.jemermed.2011.05.032. ISSN 0736-4679. PMID 21835572.
- "Clinical presentation of ectopic pregnancy", Ectopic Pregnancy, Cambridge University Press, 26 January 1996, pp. 14–20, doi:10.1017/cbo9780511663475.002, ISBN 978-0-521-49612-4
- American College of Obstetricians Gynecologists' Committee on Practice Bulletins—Gynecology (March 2018). "ACOG Practice Bulletin No. 193: Tubal Ectopic Pregnancy". Obstetrics & Gynecology. 131 (3): e91–e103. doi:10.1097/AOG.0000000000002560. ISSN 0029-7844. PMID 29470343. S2CID 3466601.
- Doubilet, Peter M.; Benson, Carol B.; Bourne, Tom; Blaivas, Michael (10 October 2013). Campion, Edward W. (ed.). "Diagnostic Criteria for Nonviable Pregnancy Early in the First Trimester". New England Journal of Medicine. 369 (15): 1443–1451. doi:10.1056/NEJMra1302417. ISSN 0028-4793. PMID 24106937.
- Fan XG, Zheng ZQ (1997). "A study of early pregnancy factor activity in preimplantation". Am. J. Reprod. Immunol. 37 (5): 359–64. doi:10.1111/j.1600-0897.1997.tb00244.x. PMID 9196793. S2CID 71525444.
- Clarke FM. Controversies in assisted reproduction and genetics. Does "EPF" have an identity?. J Assist Reprod Genet. 1997;14(9):489–491. doi:10.1023/a:1021110906666
- Clark, Stephanie Brown. (2005).Jan Steen: The Doctor's Visit.Literature, Arts, and Medicine Database. Retrieved 27 May 2007.
Lubsen-Brandsma, M.A. (1997). Jan Steen's fire pot; pregnancy test or gynecological therapeutic method in the 17th century?. Ned Tijdschr Geneeskd, 141(51), 2513–7. Retrieved 24 May 2006.
"The Doctor's Visit." (n.d.). The Web Gallery of Art. Retrieved 24 May 2006. - Ghalioungui, P.; Khalil, SH.; Ammar, A. R. (July 1963). "On an Ancient Egyptian Method of Diagnosing Pregnancy and Determining Foetal Sex". Medical History. 7 (3): 241–6. doi:10.1017/s0025727300028386. ISSN 0025-7273. PMC 1034829. PMID 13960613.
- Speert, Harold (1973). Iconographia Gyniatrica. Philadelphia: F. A. Davis. ISBN 978-0-8036-8070-8.
- Damewood MD, Rock JA (August 2005). "In memoriam: Georgeanna Seegar Jones, M.D.: her legacy lives on" (PDF). Fertility and Sterility. American Society for Reproductive Medicine. 84 (2): 541–2. doi:10.1016/j.fertnstert.2005.04.019. PMID 16363033. Archived from the original (PDF) on 9 December 2008. Retrieved 31 December 2007.
- Christophers, S. R. (16 November 1946). "The Government Lymph Establishment". Br Med J. 2 (4480): 752. doi:10.1136/bmj.2.4480.752. ISSN 0007-1447. PMC 2054716.
- Shapiro, H. A.; Zwarenstein, H. (19 May 1934). "A Rapid Test for Pregnancy on Xenopus lævis". Nature. 133 (3368): 762. Bibcode:1934Natur.133..762S. doi:10.1038/133762a0. ISSN 0028-0836. S2CID 4123060.
- Gurdon, J B; Hopwood, N (1 February 2003). "The introduction of Xenopus laevis into developmental biology: of empire, pregnancy testing and ribosomal genes". International Journal of Developmental Biology. 44 (1). ISSN 0214-6282
- Fiala, Creator, Autor: Christian (29 March 2018). "Titel: Museum für Verhütung und Schwangerschaftsabbruch - Museum of Contraception and Abortion". en.muvs.org. Retrieved 29 March 2018.
{{cite web}}: CS1 maint: multiple names: authors list (link) - Bleavins MR, Carini C, Malle JR, Rahbari R (2010). Biomarkers in Drug Development: A Handbook of Practice, Application, and Strategy, Chapter 1, Blood and Urine Chemistry. John Wiley and Sons. ISBN 978-0-470-16927-8.
- Wide L (2005). "Inventions leading to the development of the diagnostic test kit industry — from the modern pregnancy test to the sandwich assays". Upsala Journal of Medical Sciences. 110 (3): 193–216. doi:10.3109/2000-1967-066. PMID 16454158.
- Yalow RS, Berson SA (July 1960). "Immunoassay of endogenous plasma insulin in man". Journal of Clinical Investigation. 39 (7): 1157–75. doi:10.1172/JCI104130. PMC 441860. PMID 13846364.
- Kennedy, Pagan (29 July 2016). "Could Women Be Trusted With Their Own Pregnancy Tests?". The New York Times. ISSN 0362-4331. Retrieved 12 December 2016.
- Vaitukaitis, JL (December 2004). "Development of the home pregnancy test". Annals of the New York Academy of Sciences. 1038: 220–2. Bibcode:2004NYASA1038..220V. doi:10.1196/annals.1315.030. PMID 15838116. S2CID 29315420.
- "History of the Pregnancy Test Kit - Home Page". history.nih.gov. Retrieved 4 May 2020.
- A Thin Blue Line: The History of the Pregnancy Test Kit. "A Timeline of Pregnancy Testing". National Institutes of Health. Retrieved 15 March 2015.
- Nudd, Ti (9 January 2018). "Ikea Wants You to Pee on This Ad. If You're Pregnant, It Will Give You a Discount on a Crib". Adweek. Retrieved 13 January 2018.
External links
 Media related to Pregnancy test at Wikimedia Commons
Media related to Pregnancy test at Wikimedia Commons