Pulmonary interstitial emphysema
Pulmonary interstitial emphysema (PIE) is a collection of air outside of the normal air space of the pulmonary alveoli, found instead inside the connective tissue of the peribronchovascular sheaths, interlobular septa, and visceral pleura. (This supportive tissue is called the pulmonary interstitium.) This collection of air develops as a result of alveolar and terminal bronchiolar rupture. Pulmonary interstitial emphysema is more frequent in premature infants who require mechanical ventilation for severe lung disease. Infants with pulmonary interstitial emphysema are typically recommended for admission to a neonatal intensive care unit.
| Pulmonary interstitial emphysema | |
|---|---|
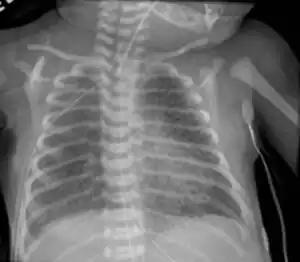 | |
| Chest radiography showing severe pulmonary interstitial emphysema | |
| Specialty | Pediatrics |
Cause
Pulmonary interstitial emphysema is a concern in any of the following:
Pathophysiology
Pulmonary interstitial emphysema is created when air bursts or ruptures through tissue from the alveoli and bronchioles into the perivascular tissue of the lung.
Diagnosis
A chest X ray may show a "salt and pepper" appearance due to the linear lucencies that are present.
Treatment
Different treatments have been used to manage pulmonary interstitial emphysema with variable success. Admission/transfer to a neonatal intensive care unit (NICU) is common and expected for patients with PIE. Treatments include:
- Lateral decubitus position with the affected side down
- High-frequency ventilation
- Lobectomy
- Selective Main Bronchial Intubation and Occlusion[1]
Prognosis
Pulmonary interstitial emphysema often resolves gradually and may take 2–3 weeks.[2] For longer durations of PIE the length of time of mechanical ventilation needed may increase and the incidence of bronchopulmonary dysplasia becomes higher. Some infants may develop chronic lobar emphysema, which may require surgical lobectomies.[3]
Epidemiology
United States
The prevalence of pulmonary interstitial emphysema widely varies with the population studied. In a 1987 study 3% of infants admitted to the neonatal intensive care unit (NICU) developed pulmonary interstitial emphysema.[2]
International
Studies reflecting international frequency demonstrated that 2-3% of all infants in NICUs develop pulmonary interstitial emphysema.[4][5] When limiting the population studied to premature infants, this frequency increases to 20-30%, with the highest frequencies occurring in infants weighing fewer than 1000 g.[6]
See also
References
- Chalak LF, Kaiser JR, Arrington RW (2007). "Resolution of pulmonary interstitial emphysema following selective left main stem intubation in a premature newborn: an old procedure revisited". Paediatr Anaesth. 17 (2): 183–6. doi:10.1111/j.1460-9592.2006.02044.x. PMID 17238893. S2CID 21128728.
- Heneghan MA, Sosulski R, Alarcon MB (1987). "Early pulmonary interstitial emphysema in the newborn: a grave prognostic sign". Clin Pediatr (Phila). 26 (7): 361–5. doi:10.1177/000992288702600707. PMID 3595042. S2CID 26285767.
- Morisot C, Kacet N, Bouchez MC, Rouland V, Dubos JP, Gremillet C, et al. (1990). "Risk factors for fatal pulmonary interstitial emphysema in neonates". Eur J Pediatr. 149 (7): 493–5. doi:10.1007/bf01959402. PMID 2347343. S2CID 23256278.
- Hart SM, McNair M, Gamsu HR, Price JF (1983). "Pulmonary interstitial emphysema in very low birthweight infants". Arch Dis Child. 58 (8): 612–5. doi:10.1136/adc.58.8.612. PMC 1628320. PMID 6351760.
- Yu VY, Wong PY, Bajuk B, Szymonowicz W (1986). "Pulmonary interstitial emphysema in infants less than 1000 g at birth". Aust Paediatr J. 22 (3): 189–92. doi:10.1111/j.1440-1754.1986.tb00221.x. PMID 3767787. S2CID 22291777.
- Gaylord MS, Thieme RE, Woodall DL, Quissell BJ (1985). "Predicting mortality in low-birth-weight infants with pulmonary interstitial emphysema". Pediatrics. 76 (2): 219–24. doi:10.1542/peds.76.2.219. PMID 4022695. S2CID 38763776.