Radical perineal prostatectomy
Radical perineal prostatectomy is a surgical procedure wherein the entire prostate gland is removed through an incision in the area between the anus and the scrotum (perineum).[1][2]
| Radical perineal prostatectomy | |
|---|---|
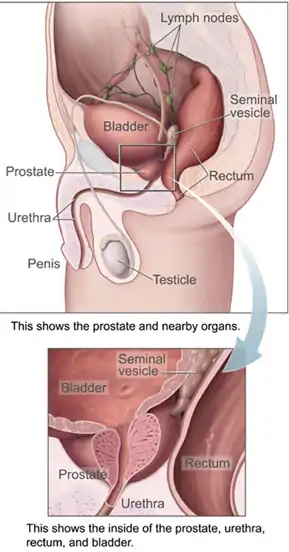 Location of prostate gland | |
| Specialty | Urology |
It is used to remove early prostate cancer, in select people who have a small well defined cancer in the prostate. It is less commonly used than the alternative methods of the retropubic route, or the robot assisted laparoscopic approach.[3][4]
When the cancer is small and confined to the prostate, radical perineal prostatectomy achieves the same rate of cure as the retropubic approach but less blood is lost and recovery is faster. One downside to the perineal approach is an increased risk of fecal incontinence.[2][5]
The procedure was first performed in 1904 by Hugh H. Young and assisted by William S. Halstead, as a way of removing the prostate in cancer treatment.
Uses
Radical perineal prostatectomy is used to remove early prostate cancer, in select people who have a small well defined cancer in the prostate.[3] It is less commonly used than the alternative methods of the retropubic route, or the robot assisted laparoscopic approach.[1][4]
It is more suited to younger men, age under 70 years, who have at least a ten-year life expectancy, few if any other medical problems, a Gleason score of less than 8 (4+4) and PSA of less than 10.[3] It may be indicated where the man with prostate cancer is obese, has had several abdominal operations before, previous pelvic arterial bypass grafts or has a delayed recurrence of prostate cancer after salvage prostatectomy and radiotherapy.[3]
Technique

Before surgery
Before the operation, an assessment of life expectancy is made. Physical examination including a digital rectal examination and routine blood tests are carried out. At least six transrectal ultrasound guided biopsies taken from different zones of the prostate are usually obtained. Other considerations include bowel preparation the day before surgery and taking antibiotics.[3]
Procedure
A radical perineal prostatectomy uses an incision in the area between the anus and the scrotum (perineum).[2][6] There is more than one way of performing the procedure.[7] In men with normal erections, a small cancer which can not be felt and Gleason scores of 6 or less, it may be possible to preserve the nerves for erection.[7] The procedure usually takes around one hour.[4]
After surgery
Over the course of the first day or two after the procedure, many men require a gradual transfer from oral fluids to soft foods. Additionally, men are encouraged to maintain mobility and painkillers may be necessary initially but tapered off over time. The hospital stay is usually short and the Foley catheter can be removed usually at three weeks after surgery. Longer term followup with PSA monitoring is required.[3]
Complications and outcomes
Lymph nodes can be sampled through the same incision, although this procedure is not common place in the U.S. at this time. When the cancer is small and confined to the prostate, radical perineal prostatectomy achieves the same rate of cure as the retropubic approach but less blood is lost and recovery is faster. One downside to the perineal approach is an increased risk of fecal incontinence.[2][5]
History
The procedure was first performed on a 70-year old married preacher on 7 April 1904 by American surgeon Hugh H. Young and assisted by William S. Halstead, as a way of removing the prostate in cancer treatment, after prostatic massage and an early type of transurethral resection of the prostate had failed to relieve him of pain in his urethra.[8] By 1937, Young reported a five-year survival rate of 50%. However, by the time the diagnosis of prostate cancer was made, it was usually too late to perform the procedure.[2][9]
Removing the prostate via the perineal route went out of favour in the 1970s. However, with the introduction the PSA test, better public awareness of options for treating localised disease, the ability to perform nerve-sparing surgery, and the advantage of there being potentially less post-operative complications using the perineal route, rekindled interest in the procedure.[3]
References
- Kirby, R. S.; Patel, M. I.; Poon, D. M. C. (2020). "Management of clinically localised disease". Fast Facts: Prostate Cancer: If, when and how to intervene. Karger Medical and Scientific Publishers. p. 69. ISBN 978-3-318-06587-9.
- Korman, Howard J. (3 November 2020). "Radical Perineal Prostatectomy for Prostate Cancer: Practice Essentials, Technical Considerations, Outcomes". www.medscape.com. Medscape. Archived from the original on 7 February 2021. Retrieved 19 February 2021.
- Sullivan L.D. (2003) Radical Perineal Prostatectomy. In: Bruskewitz R.C. (eds) Atlas of the Prostate. Current Medicine Group, London. https://doi.org/10.1007/978-1-4615-6505-5_10
- Zippe C.D. (2006) Radical Perineal Prostatectomy. In: Novick A.C. et al. (eds) Operative Urology at the Cleveland Clinic. Humana Press. https://doi.org/10.1007/978-1-59745-016-4_37
- Eden, Christopher; Hutton, Anthony (2013). "56. Laparoscopic radical prostatectomy". In Tewari, Ashutosh (ed.). Prostate Cancer: A Comprehensive Perspective. Springer. p. 679. ISBN 978-1-4471-2863-2.
- "radical perineal prostatectomy". www.cancer.gov. 2 February 2011. Retrieved 19 February 2021.
- Korman, Howard (8 July 2020). "Radical Perineal Prostatectomy for Prostate Cancer Technique: Approach Considerations, Perineal Approach to Radical Prostatectomy, Postoperative Care". emedicine.medscape.com. Medscape. Archived from the original on 19 February 2021. Retrieved 19 February 2021.
- "Radical Prostatectomy | The British Association of Urological Surgeons Limited". www.baus.org.uk. Retrieved 19 February 2021.
- Shimkin, Michael B. (1977). Contrary to Nature: Being an Illustrated Commentary on Some Persons and Events of Historical Importance in the Development of Knowledge Concerning ... Cancer. U.S. Department of Health, Education, and Welfare, Public Health Service, National Institutes of Health. p. 265. ISBN 9780719400124.
Further reading
- Young, Hugh Hampton (December 1909). "XV. Cancer of the Prostate". Annals of Surgery. 50 (6): 1144–1233. doi:10.1097/00000658-190912000-00015. ISSN 0003-4932. PMC 1407492. PMID 17862456.