Wrist osteoarthritis
Wrist osteoarthritis is gradual loss of articular cartilage and hypertrophic bone changes (osteophytes). While in many joints this is part of normal aging (senescence), in the wrist osteoarthritis usually occurs over years to decades after scapholunate interosseous ligament rupture or an unhealed fracture of the scaphoid. Characteristic symptoms including pain, deformity and stiffness. Pain intensity and incapability (limited function) are notably variable and do not correspond with arthritis severity on radiographs.
| Wrist osteoarthritis | |
|---|---|
| Other names | Osteoarthritis of the wrist |
 | |
| Specialty | Orthopedic |
Osteoarthritis of the wrist can be idiopathic, but it is mostly seen as a post-traumatic condition.[1][2] There are different types of post-traumatic osteoarthritis. Scapholunate advanced collapse (SLAC) is the most common form, followed by scaphoid non-union advanced collapse (SNAC).[3] Other post-traumatic causes such as intra-articular fractures of the distal radius or ulna can also lead to wrist osteoarthritis, but are less common.
Types
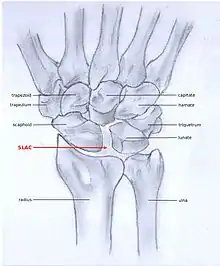
SLAC and SNAC are two patterns of wrist osteoarthritis, following predictable patterns depending on the type of underlying injury. SLAC is caused by scapholunate ligament rupture, and SNAC is caused by a scaphoid fracture which does not heal non-union.
SLAC is more common than SNAC; 55% of the patients with wrist osteoarthritis have a SLAC wrist.[3]
SLAC
Scapholunate advanced collapse (SLAC) is a predictable pattern of wrist osteoarthritis that results from untreated long-standing scapholunate ligament rupture and the associated carpal malalignment.[4] The misalignment is described as dorsal intercalated segment instability (DISI) which is where the lunate angulates towards the dorsal side of the hand.[2][5]
SNAC
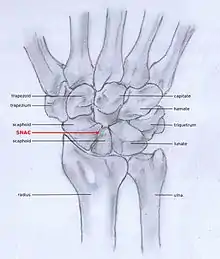
Scaphoid fracture non-union changes the shape of the scaphoid bone and results in DISI malalignment.[2][5] Scaphoid Non-union Advanced collapse (SNAC) is the pattern of osteoarthritis that develops in relation to the malalignment.
Stages
Post-traumatic osteoarthritis can be classified into four stages.[1][6] These stages are similar between SLAC and SNAC wrists. Each stage has a different treatment.
- Stage I: the osteoarthritis is only localized in the distal scaphoid and radial styloid.
- Stage II: the osteoarthritis is localized in the entire radioscaphoid joint.
- Stage III: the osteoarthritis is localized in the entire radioscaphoid joint with involvement of the capitolunate joint.
- Stage IV: the osteoarthritis is located in the entire radiocarpal joint and in the intercarpal joints. It also may involve the distal radio-ulnar joint (DRUJ).
 Stage I
Stage I Stage II
Stage II Stage III
Stage III Stage IV
Stage IV
Signs and symptoms
The most common initial presenting symptom of wrist osteoarthritis is joint pain.[7][8] Other signs and symptoms, as with any joint affected by osteoarthritis, include:
- Loss of motion stiffness, which can be worse after a period of rest, such as when one awakes in the morning.
- Deformity of the wrist. There is a characteristic dorsal radial fullness related to osteophytes and joint effusion.
- Crepitus (crackling), which is felt when the wrist is moved passively.[8]
These symptoms can lead to loss of function and less daily activity.[7]
Mechanism
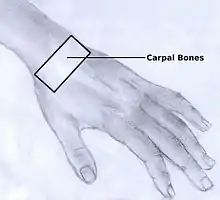
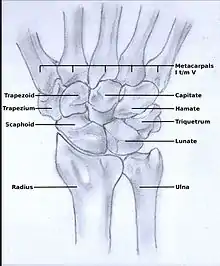
In order to understand the cause of post-traumatic wrist osteoarthritis it is important to know and understand the anatomy of the wrist. The hand is subdivided into three parts:
The wrist consists of eight small carpal bones. Each of these carpal bones has a different size and shape. They contribute towards the stability of the wrist and are ranked in two rows, each consisting of four bones.
Diagnosis
Osteoarthritis of the wrist is predominantly a clinical diagnosis, and thus is primarily based on the patients medical history, physical examination and wrist X-rays.[2]
Medical history
The person may or may not recall an old wrist injury. [7]
Physical examination
Examination may identify limited passive wrist motion, pain at the extremes of wrist motion, tenderness at the radioscaphoid joint, and dorsal radial prominence.[2] Activities that use forceful wrist extension such as rising from a chair or push-ups may be painful.
In the absence of gout, chondrocalcinosis, rheumatoid arthritis, or prior distal radius fracture, a person with gradual onset limited motion and pain in the wrist likely has wrist osteoarthritis.
X-rays
Radiographs can confirm the diagnosis of wrist osteoarthritis. The earliest sign is narrowing of the joint space between the radius and the scaphoid and an osteophyte off the tip of the radial styloid. [9]
SLAC
Because SLAC results from scapholunate ligament rupture, there is a larger space between the two bones, also known as the Terry Thomas sign.[10] Scaphoid instability due to the ligament rupture can be stactic or dynamic.[11] When the X-ray is diagnostic and there is a convincing Terry Thomas sign it is a static scaphoid instability. When the scaphoid is made unstable by either the patient or by manipulation by the examining physician it is a dynamic instability.[11]
SNAC
In order to diagnose a SNAC wrist you need a PA view X-ray and a lateral view X-ray. As in SLAC, the lateral view X-ray is performed to see if there is a DISI.[12] Computed tomography (CT) or Magnetic Resonance Imaging (MRI) are rarely used to diagnose SNAC or SLAC wrist osteoarthritis because there is no additional value.[7] Also, these techniques are much more expensive than a standard X-ray. CT or MRI may be used if there is a strong suspicion for another underlying pathology or disease.[7]
Treatment
Post-traumatic wrist osteoarthritis can be accommodated. A wrist splint, ice, acetaminophen, and NSAIDs may alleviate symptoms. Surgery to change the wrist anatomy to attempt to alleviate pain is an option.[1][13][2][6]
Stage I
For stage I, normally, nonsurgical treatment is sufficient. Injections of corticosteroid may be considered. Keep in mind that corticosteroids provide, at best, temporary alleviation of discomfort. And corticosteroid injection harms cartilage. Since people with Stage 1 arthritis have good cartilage, one might be cautious with corticosteroid injection.
Surgical options for mild arthritis may include neurectomy of the anterior and posterior interosseous nerves, or radial styloidectomy, in which the radial styloid is surgically removed from the distal radius.
Stage II
The surgical options for stage II and III wrist osteoarthritis are excision of some of the bones with or without fusion (arthrodesis) of the others. The idea is to try to alleviate pain while maintaining some wrist motion.
One technique is to remove one row of carpal bones. The bones closer to the forearm (proximal) are removed: scaphoid, lunate, and triquetrum.[14] It is important that the radioscaphocapitate ligament is left intact, because if the ligament is not preserved the capitate bone will translate to the ulnar side of the wrist and move away from the distal radius.[1][15]
The new articulation of the capitate with the lunate fossa of the distal radius is not as congruent as the former scaphoid-lunate-radius joint.[16][17] This and other issues contribute to potential to develop arthritis over the years. In part based on these concerns, some surgeon prefer to maintain the lunate in patients younger than 40 years proximal row carpectomy. [6][18]
A surgery called four-corner arthrodesis is an option.[6] The capitate, lunate, hamate and triquetrum are fused together in this procedure and the scaphoid is excised.[1][14] Before the arthrodesis is executed, the lunate must be reduced out of DISI position.[14] Because the radiolunate joint is typically preserved in stage II SLAC and SNAC wrists, this joint can be the only remaining joint of the proximal wrist. Both procedures are often combined with wrist denervation, as described in the text of treatment stage I.
Stage III
In Stage III wrist osteoarthritis, some surgeons offer patients proximal row carpectomy and interpose some of the wrist capsule to account for the arthritis in the capitate. Four-corner arthrodesis, as described above in stage II, is also an option.
Stage IV
In this stage there are two surgical treatment options; total wrist arthroplasty and total wrist arthrodesis. Total wrist arthrodesis has become the standard surgical treatment for patients with stage IV wrist osteoarthritis. During this procedure the carpal bones are all fused together and are then fastened to the distal radius.[14] Patients who still want to undertake heavy labor benefit the most of this surgical approach,[19] because after surgery and recovery this is still possible. However, the arc of motion is extremely diminished by this type of surgery.
The best option for those who wish for a motion-sparing procedure is total wrist arthroplasty. However, impact loading should be avoided, an object heavier than 4.5 kg should not be lifted.[20] So, this surgical approach has postoperative activity restrictions. Nevertheless, patients with a total wrist arthrodesis on one side and a total wrist arthroplasty on the other, prefer the total wrist arthroplasty.[21] The procedure exists of a couple of elements. First, the proximal row is removed and the distal row is fastened to the metacarpals. Then, one side of the arthroplasty is placed upon the distal row and the other side on the distal radius. Additionally, the head of the ulna is removed.[14]
References
- Weiss, KE; Rodner, CM (May–June 2007). "Osteoarthritis of the Wrist, Review article". The Journal of Hand Surgery. 32A (5): 725–46. doi:10.1016/j.jhsa.2007.02.003. PMID 17482013. S2CID 5821652.
- Shah, CM; Stern PJ (2013). "Scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) wrist arthritis". Curr Rev Musculoskelet Med. 6 (1): 9–17. doi:10.1007/s12178-012-9149-4. PMC 3702758. PMID 23325545.
- Bisneto EN, Freitas MC, Paula EJ, Mattar R, Zumiotti AV (2011). "Comparison between proximal row carpectomy and four-corner fusion for treating osteoarthrosis following carpal trauma: a prospective randomized study". Clinics (Sao Paulo). 66 (1): 51–5. doi:10.1590/s1807-59322011000100010. PMC 3044580. PMID 21437436.
- Tischler, Brian T.; Diaz, Luis E.; Murakami, Akira M.; Roemer, Frank W.; Goud, Ajay R.; Arndt, William F.; Guermazi, Ali (2014). "Scapholunate advanced collapse: a pictorial review". Insights into Imaging. 5 (4): 407–417. doi:10.1007/s13244-014-0337-1. ISSN 1869-4101. PMC 4141341. PMID 24891066.
- Omori, S; Moritomo, H; Omokawa, S; Murase, T; Sugamoto, K; Yoshikawa, H (July 2013). "In vivo 3-dimensional analysis of dorsal intercalated segment instability deformity secondary to scapholunate dissociation: a preliminary report". The Journal of Hand Surgery. 38 (7): 1346–55. doi:10.1016/j.jhsa.2013.04.004. PMID 23790423.
- Strauch, RJ (Apr 2011). "Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis--update on evaluation and treatment". The Journal of Hand Surgery. 36 (4): 729–735. doi:10.1016/j.jhsa.2011.01.018. PMID 21463735.
- Sinusas, K (2012). "Osteoarthritis: diagnosis and treatment". Am Fam Physician. 85 (1): 49–56. PMID 22230308.
- Manek, NJ; Lane NE (2000). "Osteoarthritis: current concepts in diagnosis and management". Am Fam Physician. 61 (6): 1795–804. PMID 10750883.
- "Radiocarpal joint space". radref.org. Retrieved 2017-01-18.
- Wolfe, SW; Hotchkiss, RN (2011). Green's Operative Hand Surgery, 6th Edition (6th ed.). Churchill Livingstone. ISBN 978-1-4160-5279-1.
- Jupiter, JB; Edwards, JE (1991). Flynn's hand surgery, fourth edition; chapter 10 dislocations and fracture dislocations of the carpus (4th ed.). Baltimore: Williams&Wilkins. pp. 198–199. ISBN 978-0-683-04490-4.
- Novelline, RA (2004). Squire's fundamentals of radiology, 6th Edition (6th ed.). United States of America: President and fellows of Harvard college. ISBN 978-0-674-01279-0.
- Talwalkar, SC; Hayton MC; Stanley JK (2008). "Wrist osteoarthritis". Scand J Surg. 97 (4): 305–9. doi:10.1177/145749690809700406. PMID 19211384. S2CID 43701956.
- Berger, RA; Weiss, APC (2004). Hand surgery, first edition; Principles of Limited Wrist Arthrodesis (1st ed.). Philadelphia: Lippincott Williams & Wilkins. pp. 1290–1295, 1320–1329, 1352–1373. ISBN 978-0-7817-2874-4.
- Berger, RA; Landsmeer, JM (1990). "The palmar radiocarpal ligaments: a study of adult and fetal hunman wrist joints". The Journal of Hand Surgery. 15 (6): 847–854. doi:10.1016/0363-5023(90)90002-9. PMC 2328843. PMID 2269772.
- Inglis, AE; Jones, EC (1977). "Proximal row carpectomy for diseases of the proximal row". The Journal of Hand Surgery. 59A (4): 460–463. PMID 863938.
- Imrbiglia, JE; Broudy, AS; Hagberg, WC (1990). "Proximal row carpectomy: clinical evaluation". The Journal of Hand Surgery. 15 (3): 426–430. doi:10.1016/0363-5023(90)90054-U. PMID 2348060.
- Wall, LB; DiDonna, ML (Aug 2013). "Proximal row carpectomy: minimum 20-year follow-up". The Journal of Hand Surgery. 38 (8): 1498–1504. doi:10.1016/j.jhsa.2013.04.028. PMID 23809467.
- Weiss, APC; Hastings, H (Jan 1995). "Wrist arthrodesis for traumatic conditions: a study of plate and local bone graft application". The Journal of Hand Surgery. 20A (5): 50–56. doi:10.1016/S0363-5023(05)80058-9. PMID 7722266.
- Anderson, MC; Adams, BD (2005). "Total wrist arthroplasty". Hand Clinics. 21 (4): 621–630. doi:10.1016/j.hcl.2005.08.014. PMID 16274871.
- Vicar, AJ; Burton, RI (1988). "Surgical management of the rheumatoid wrist-fusion or arthroplasty". The Journal of Hand Surgery. 11A (6): 790–797. doi:10.1016/s0363-5023(86)80224-6. PMID 3794231.