Schistosoma mansoni
Schistosoma mansoni is a water-borne parasite of humans, and belongs to the group of blood flukes (Schistosoma). The adult lives in the blood vessels (mesenteric veins) near the human intestine. It causes intestinal schistosomiasis (similar to S. japonicum, S. mekongi, S. guineensis, and S. intercalatum). Clinical symptoms are caused by the eggs. As the leading cause of schistosomiasis in the world, it is the most prevalent parasite in humans. It is classified as a neglected tropical disease. As of 2021, the World Health Organization reports that 236.6 million people have schistosomiasis and most of it is due to S. mansoni. It is found in Africa, the Middle East, the Caribbean, Brazil, Venezuela and Suriname.[1]
| Schistosoma mansoni | |
|---|---|
 | |
| Schistosomes copulating | |
| Scientific classification | |
| Domain: | Eukaryota |
| Kingdom: | Animalia |
| Phylum: | Platyhelminthes |
| Class: | Trematoda |
| Order: | Diplostomida |
| Family: | Schistosomatidae |
| Genus: | Schistosoma |
| Species: | S. mansoni |
| Binomial name | |
| Schistosoma mansoni Sambon, 1907 | |

Unlike other flukes (trematodes) in which sexes are not separate (monoecious), schistosomes are unique in that adults are divided into males and females, thus, gonochoric. However, a permanent male-female pair, a condition called in copula, is required to become adults; for this, they are considered as hermaphrodites.
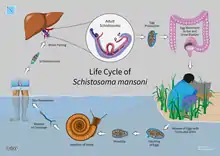
The life cycle of schistosomes includes two hosts: humans as definitive hosts, where the parasite undergoes sexual reproduction, and snails as intermediate hosts, where a series of asexual reproduction takes place. S. mansoni is transmitted through water, where freshwater snails of the genus Biomphalaria act as intermediate hosts. The larvae are able to live in water and infect the hosts by directly penetrating the skin. Prevention of infection is done by improved sanitation and killing the snails. Infection is treated with praziquantel.
S. mansoni was first noted by Theodor Maximillian Bilharz in Egypt in 1851, while discovering S. haematobium. Sir Patrick Manson identified it as unique species in 1902. Louis Westenra Sambon gave the name Schistosomum mansoni in 1907 in honour of Manson.[2][3][4]
Structure
Adult
Schistosomes, unlike other trematodes, are long and cylindrical worms and are sexually dimorphic. The male S. mansoni is approximately 1 cm long (0.6–1.1 cm)[5] and is 0.1 cm wide. It is white, and it has a funnel-shaped oral sucker at its anterior end followed by a second pediculated ventral sucker. The external part of the worm is composed of a double bilayer, which is continuously renewed as the outer layer, known as the membranocalyx, and is shed continuously.[6] The tegument bears a large number of small tubercules. The suckers have small thorns in their inner part as well as in the buttons around them. The male genital apparatus is composed of 6 to 9 testicular masses, situated dorsally. There is one deferent canal beginning at each testicle, which is connected to a single deferent that dilates into a reservatory, the seminal vesicle, located at the beginning of the gynaecophoric canal. The copula happens through the coaptation of the male and female genital orifices.[7]
The female has a cylindrical body, longer and thinner than the male's (1.2 to 1.6 cm long by 0.016 cm wide). It has the general appearance of a roundworm. The female parasite is darker, and it looks gray. The darker color is due to the presence of a pigment (hemozoin) in its digestive tube.[8] This pigment is derived from the digestion of blood. The ovary is elongated and slightly lobulated and is located on the anterior half of the body. A short oviduct conducts to the ootype, which continues with the uterine tube. In this tube it is possible to find 1 to 2 eggs (rarely 3 to 4) but only 1 egg is observed in the ootype at any one time. The genital pore opens ventrally. The posterior two-thirds of the body contain the viteline glands and their winding canal, which unites with the oviduct a little before it reaches the ootype.[9]
The digestive tube begins at the anterior extremity of the worm, at the bottom of the oral sucker. The digestive tube is composed of an esophagus, which divides in two branches (right and left) and that reunite in a single cecum. The intestines end blindly, meaning that there is no anus.
Sex
S. mansoni and other schistosomes are the only flukes or flatworms that exhibit sex separation as they exist as male and female individuals as in dioecious animals.[10][11] However, they are not truly dioecious since the adults live in permanent male-female pairs, a condition called in copula. Although they can be physically separated,[12] isolated females cannot grow into sexually-mature adults.[13][14] In copula starts in the liver only after which they can move to their final habitation, the inferior mesenteric veins. Individual females cannot enter the mesenteric veins.[15] Sex organs, the gonads, are also incompletely separated and are interdependent between sexes. Egg-making organ, the vitelline gland in female does not develop in the absence of male.[16] Male gametes, spermatozoa, are present in the oviduct.[17] In males, there are rudimentary ovaries, oviduct, and oocytes (developing female gametes),[18] as well as vitelline cells.[19] Males also possess the genes for hermaphroditism in flukes.[20] Thus, they are technically hermaphrodites.[18][20]
Eggs
The eggs are oval-shaped, measuring 115–175 µm long and 45–47 µm wide, and ~150 µm diameter on average. They have pointed spines towards the broader base on one side, i.e. lateral spines. This is an important diagnostic tool because co-infection with S. haematobium (having a terminal-spined eggs) is common, and they are hard to distinguish.[21] When the eggs are released into the water, a lot of them are immature and unfertilised so that they do not hatch. When the eggs are larger than 160 µm in diameter, they also fail to hatch.[22][23]
Larva
The miracidium (from the Greek word μειράκιον, meirakion, meaning youth) is pear-shaped, and gradually elongates as it ages. It measures about 136 μm long and 55 μm wide. The body is covered by anucleate epidermal plates separated by epidermal ridges. The epidermal cells give off numerous hair-like cilia on the body surface. There are 17–22 epidermal cells. Epidermal plate is absent only at the extreme anterior called apical papilla, or terebratorium, which contains numerous sensory organelles.[24] Its internal body is almost fully filled with glycogen particles and vesicles.[25]
The cercaria has a characteristic bifurcated tail, classically called furcae (Latin for fork); hence, the name (derived from a Greek word κέρκος, kerkos, meaning tail). The tail is highly flexible and its beating propels the cercaria in water.[26] It is about 0.2 mm long and 47 μm wide, somewhat loosely attached to the main body. The body is pear-shaped and measures 0.24 mm in length and 0.1 mm in width.[27] Its tegument is fully covered with spine. A conspicuous oral sucker is at the apex. As a non-feeding larva, there are no elaborate digestive organs, only oesophagus is distinct. There are three pairs of mucin glands connected to laterally to the oral sucker at the region of the ventral sucker.[28][29]
Physiology
Feeding and nutrition
Developing Schistosoma mansoni worms that have infected their definitive hosts, prior to the sexual pairing of males and females, require a nutrient source in order to properly develop from cercariae to adults. The developing parasites lyse host red blood cells to gain access to nutrients and also makes its own fungi from its waste it is hard to detect; the hemoglobin and amino acids the blood cells contain can be used by the worm to form proteins.[30] While hemoglobin is digested intracellularly, initiated by salivary gland enzymes, iron waste products cannot be used by the worms, and are typically discarded via regurgitation.[31]
Kasschau et al. (1995) tested the effect of temperature and pH on the ability of developing S. mansoni to lyse red blood cells.[30] The researchers found that the parasites were best able to destroy red blood cells for their nutrients at a pH of 5.1 and a temperature of 37 °C.[30]
Locomotion
Schistosoma mansoni is locomotive in primarily two stages of its life cycle: as cercariae swimming freely through a body of freshwater to locate the epidermis of their human hosts, and as developing and fully-fledged adults, migrating throughout their primary host upon infection.[31] Cercariae are attracted to the presence of fatty acids on the skin of their definitive host, and the parasite responds to changes in light and temperature in their freshwater medium to navigate towards the skin.[32] Ressurreicao et al. (2015) tested the roles of various protein kinases in the ability of the parasite to navigate its medium and locate a penetrable host surface.[32] Extracellular signal-regulated kinase and protein kinase C both respond to changes in medium temperature and light levels, and the stimulation of p38 mitogen-activated protein kinase, associated with recognition of parasite host surface, results in a glandular secretion that deteriorates the host epidermis, and allows the parasite to burrow into its host.
The parasite's nervous system contains bilobed ganglia and several nerve cords which splay out to every surface of the body; serotonin is a transmitter distributed widely throughout the nervous system and plays an important role in nervous reception, and stimulating mobility.[33]
Life cycle
Intermediate host
After the eggs of the human-dwelling parasite are emitted in the faeces and into the water, the ripe miracidium hatches out of the egg. The hatching happens in response to temperature, light and dilution of faeces with water. The miracidium searches for a suitable freshwater snail belonging to the genus Biomphalaria. In South America, the principal intermediate host is Biomphalaria glabrata, while B. straminea and B. tenagophila are less common.[34] A land snail Achatina fulica was reported in 2010 to act as a host in Venezuela.[35] In Africa, B. glabratra, B. pfeifferi, B. choanomphala and B. sudanica act as the hosts;[36] but in Egypt, the main snail host is B. alexandrina.[37]
Miracidia directly penetrate the soft tissue of snail. Inside the snail, they lose their cilia and develop into mother sporocysts. The sporocysts rapidly multiply by asexual reproduction, each forming numerous daughter sporocysts. The daughter sporocysts move to the liver and gonads of the snail, where they undergo further growth.[38] Within 2–4 weeks, they undergo metamorphosis and give rise to fork-tailed cercariae. Stimulated by light, hundreds of cercariae penetrate out of the snail into water.[39]
Definitive host
The cercaria emerge from the snail during daylight and they propel themselves in water with the aid of their bifurcated tail, actively seeking out their final host. In water, they can live for up to 12 hours, and their maximum infectivity is between 1 and 9 hours after emergence.[40] When they recognise human skin, they penetrate it within a very short time. This occurs in three stages, an initial attachment to the skin, followed by the creeping over the skin searching for a suitable penetration site, often a hair follicle, and finally penetration of the skin into the epidermis using cytolytic secretions from the cercarial post-acetabular, then pre-acetabular glands. On penetration, the head of the cercaria transforms into an endoparasitic larva, the schistosomule. Each schistosomule spends a few days in the skin and then enters the circulation starting at the dermal lymphatics and venules. Here, they feed on blood, regurgitating the haem as hemozoin.[41] The schistosomule migrates to the lungs (5–7 days post-penetration) and then moves via circulation through the left side of the heart to the hepatoportal circulation (>15 days) where, if it meets a partner of the opposite sex, it develops into a sexually mature adult and the pair migrate to the mesenteric veins.[42] Such pairings are monogamous.[43]
Male schistosomes undergo normal maturation and morphological development in the presence or absence of a female, although behavioural, physiological and antigenic differences between males from single-sex, as opposed to bisex, infections have been reported. On the other hand, female schistosomes do not mature without a male. Female schistosomes from single-sex infections are underdeveloped and exhibit an immature reproductive system. Although the maturation of the female worm seems to be dependent on the presence of the mature male, the stimuli for female growth and for reproductive development seem to be independent from each other.
The adult female worm resides within the adult male worm's gynaecophoric canal, which is a modification of the ventral surface of the male, forming a groove. The paired worms move against the flow of blood to their final niche in the mesenteric circulation, where they begin egg production (>32 days). The S. mansoni parasites are found predominantly in the small inferior mesenteric blood vessels surrounding the large intestine and caecal region of the host. Each female lays approximately 300 eggs a day (one egg every 4.8 minutes), which are deposited on the endothelial lining of the venous capillary walls.[44] Most of the body mass of female schistosomes is devoted to the reproductive system. The female converts the equivalent of almost her own body dry weight into eggs each day. The eggs move into the lumen of the host's intestines and are released into the environment with the faeces.
Genome
Schistosoma mansoni has 8 pairs of chromosomes (2n = 16)—7 autosomal pairs and 1 sex pair. The female schistosome is heterogametic, or ZW, and the male is homogametic, or ZZ. Sex is determined in the zygote by a chromosomal mechanism. The genome is approximately 270 MB with a GC content of 34%, 4–8% highly repetitive sequence, 32–36% middle repetitive sequence and 60% single copy sequence. Numerous highly or moderately repetitive elements are identified, with at least 30% repetitive DNA. Chromosomes range in size from 18 to 73 MB and can be distinguished by size, shape, and C banding.[45]
In 2000, the first BAC library of Schistosome was constructed.[46] In June 2003, a ~5x whole genome shotgun sequencing project was initiated at the Sanger Institute.[47] Also in 2003, 163,000 ESTs (expressed sequence tags) were generated (by a consortium headed by the University of São Paulo) from six selected developmental stages of this parasite, resulting in 31,000 assembled sequences and an estimated 92% of the 14,000-gene complement.[48]
In 2009 the genomes of both S. mansoni and S. japonicum were published, with each describing 11,809 and 13,469 genes, respectively. S. mansoni genome has increased protease families and deficiencies in lipid anabolism; which are attributed to its parasitic adaptation. Proteases included the invadolysin (host penetration) and cathepsin (blood-feeding) gene families.[49][50]
In 2012, an improved version of the S. mansoni genome was published, which consisted of only 885 scaffolds and more than 81% of the bases organised into chromosomes.[51]
In 2019, Ittiprasert, Brindley and colleagues employed programmed CRISPR/Cas9 knockout of the gene encoding the T2 ribonuclease of the egg of Schistosoma mansoni, advancing functional genomics and reverse genetics in the study of schistosomes, and platyhelminths generally <https://doi.org/10.7554/eLife.41337>.
Pathology

Schistosome eggs, which may become lodged within the hosts tissues, are the major cause of pathology in schistosomiasis. Some of the deposited eggs reach the outside environment by passing through the wall of the intestine; the rest are swept into the circulation and are filtered out in the periportal tracts of the liver, resulting in periportal fibrosis. Onset of egg laying in humans is sometimes associated with an onset of fever (Katayama fever). This "acute schistosomiasis" is not, however, as important as the chronic forms of the disease. For S. mansoni and S. japonicum, these are "intestinal" and "hepatic schistosomiasis", associated with formation of granulomas around trapped eggs lodged in the intestinal wall or in the liver, respectively. The hepatic form of the disease is the most important, granulomas here giving rise to fibrosis of the liver and hepatosplenomegaly in severe cases. Symptoms and signs depend on the number and location of eggs trapped in the tissues. Initially, the inflammatory reaction is readily reversible. In the latter stages of the disease, the pathology is associated with collagen deposition and fibrosis, resulting in organ damage that may be only partially reversible.[52]
Granuloma formation is initiated by antigens secreted by the miracidium through microscopic pores within the rigid egg shell, and the immune response to granuloma, rather than the direct action of egg antigens, causes the symptoms.[53] The granulomas formed around the eggs impair blood flow in the liver and, as a consequence, induce portal hypertension. With time, collateral circulation is formed and the eggs disseminate into the lungs, where they cause more granulomas, pulmonary arteritis and, later, cor pulmonale. A contributory factor to portal hypertension is Symmers' fibrosis, which develops around branches of the portal veins. This fibrosis occurs only many years after the infection and is presumed to be caused in part by soluble egg antigens and various immune cells that react to them.[54]
Recent research has shown that granuloma size is consistent with levels of IL-13, which plays a prominent role in granuloma formation and granuloma size. IL-13 receptor α 2 (IL-13Rα2) binds IL-13 with high affinity and blocks the effects of IL-13. Thus, this receptor is essential in preventing the progression of schistosomiasis from the acute to the chronic (and deadly) stage of disease. Synthetic IL-13Rα2 given to mice has resulted in significant decreases in granuloma size, implicating IL-13Rα2 as an important target in schistosomiasis.[55]
S. mansoni infection often occurs alongside those of viral hepatitis, either hepatitis B virus (HBV) or hepatitis C virus (HCV). This is due to high prevalence of schistosomiasis in areas where chronic viral hepatitis is prevalent. One important factor was the development of large reservoir of infection due to extensive schistosomiasis control programs that used intravenously administered tartar emetic since the 1960s.[52] Co-infection is known to cause earlier liver deterioration and more severe illness.[56]
Evasion of host immunity
Adult and larval worms migrate through the host's blood circulation avoiding the host's immune system. The worms have many tools that help in this evasion, including the tegument, antioxidant proteins, and defenses against host membrane attack complex (MAC).[57] The tegument coats the worm and acts as a physical barrier to host antibodies and complement. Host immune defenses are capable of producing superoxide, but these are counterattacked by antioxidant proteins produced by the parasite. Schistosomes have four superoxide dismutases, and levels of these proteins increase as the schistosome grows. Antioxidant pathways were first recognised as a chokepoints for schistosomes,[58] and later extended to other trematodes and cestodes. Targeting of this pathway with different inhibitors of the central antioxidant enzyme thioredoxin glutathione reductase (TGR) results in reduced viability of worms.[59] Decay accelerating factor (DAF) protein is present on the parasite tegument and protects host cells by blocking formation of MAC. In addition, schistosomes have six homologues of human CD59 which are strong inhibitors of MAC.[60]
Diagnosis
The presence of S. mansoni is detected by microscopic examination of parasite eggs in stool. A staining method called Kato-Katz technique is used for stool examination. It involves methylene blue-stained cellophane soaked in glycerine or glass slides.[61] A costlier technique called formalin-ether concentration technique (FECT) is often used in combination with the direct faecal smear for higher accuracy. Serological and immunological tests are also available. Antibodies and antigens can be detected in the blood using ELISA to identify infection. Adult worm antigens can be detected by indirect haemagglutination assays (IHAs). Polymerase chain reaction (PCR) is also used for detecting the parasite DNA. Circulating cathodic antigen (CCA) in urine can be tested with lateral flow immune-chromatographic reagent strip and point-of-care (POC) tests.[62]
Egg detection and immunologic tests are not that sensitive.[63] Polymerase chain reaction (PCR) based testing is accurate and rapid.[63] They, however, are not frequency used in countries were the disease is common due to the cost of the equipment and the technical experience required to run them.[63] Using a microscope to detect eggs costs about US$0.40 per test well PCR is about $US7 per test as of 2019.[64] Loop-mediated isothermal amplification (LAMP) are being studied as they are lower cost.[63] LAMP testing is not commercially available as of 2019.[64]
Treatment
The standard drug for S. mansoni infection is praziquantel at a dose of 40 mg/kg. Oxamniquine is also used.[65]
Epidemiology
As of WHO report in 2016, 206.5 million people worldwide are having schistosomiasis due to different species of Schistosoma. More than 105 million people were given medical treatment.[1] S. mansoni is the major species causing an annual death of about 130,000.[66] It is endemic in 55 countries and most prevalent in Africa, the Middle East, the Caribbean, Brazil, Venezuela and Suriname.[67] About 80-85% of schistosomiasis is found in sub-Saharan Africa, where S. haematobium, S. intercalatum and S. mansoni are endemic. Approximately 393 million Africans are at risk of infection from S. mansoni, of which about 55 million are infected at any moment. Annual death due to S. mansoni is about 130,000.[68] The prevalence rate in different countries of Africa are: 73.9% in northern Ethiopia, 37.9% in western Ethiopia, 56% in Nigeria, 60.5% in Kenya, 64.3% in Tanzania, 19.8% in Ghana, and 53.8% in Côte d'Ivoire.[69] In Egypt, 60% of the population in the Northern and Eastern parts of the Nile Delta and only 6% in the Southern part are infected.[70]
S. mansoni is commonly found in places with poor sanitation. Because of the parasite's fecal-oral transmission, bodies of water that contain human waste can be infectious. Water that contains large populations of the intermediate host snail species is more likely to cause infection. Young children living in these areas are at greatest risk because of their tendency to swim and bathe in cercaria-infected waters longer than adults .[71] Anyone travelling to the areas described above, and who is exposed to contaminated water, is at risk of schistosomiasis.
History
The intermediate hosts Biomphalaria snails are estimated to originate in South America 95–110 million years ago. But the parasites Schistosoma originated in Asia. In Africa, the progenitor species evolved into modern S. mansoni and S. haematobium around 2–5 million years ago.[72][73]
A German physician Theodor Maximillian Bilharz was the first to discover the parasite in 1851, while working at Kasr el-Aini Hospital, a medical school in Cairo. Bilharz recovered them from autopsies of dead soldiers, and noticed two distinct parasites.[74] He described one of them as Distomum haematobium (now S. haematobium) in 1852,[75] but failed to identify the other. In one of his letters to his mentor Karl Theordor von Siebold, he mentioned some of the eggs were different in having terminal spines while some had lateral spines.[76] Terminal-spined eggs are unique to S. haematobium, while lateral spines are found only in S. mansoni. Bilharz also noted that the adult flukes were different in anatomy and number eggs they produced.[77] He introduced the terms bilharzia and bilharziasis for the name of the infection in 1856. A German zoologist David Friedrich Weinland corrected the genus name to Schistosoma in 1858; and introduced the disease name as schistosomiasis.[78]
The species distinction was first recognised by Patrick Manson at the London School of Hygiene & Tropical Medicine. Manson identified lateral-spined eggs in the faeces of a colonial officer earlier posted to the West Indies, and concluded that there were two species of Schistosoma.[79] An Italian-British physician Louis Westenra Sambon gave the new names Schistosomum haematobium and Schistosomum mansoni in 1907, the latter to honour Manson.[2] Sambon only gave partial description using a male worm. In 1908, a Brazilian physician Manuel Augusto Pirajá da Silva gave a complete description of male and female worms, including the lateral-spined eggs.[80] Pirajá da Silva obtained specimens from three necropsies and eggs from 20 stool examinations in Bahia.[81] He gave the name S. americanum.[82] The species identity was confirmed in 1907 by British parasitologist Robert Thomson Leiper,[79] identifying the specific snail host, and distinguishing the egg structure, thereby establishing the life cycle.[83]
References
- "Schistosomiasis". www.who.int. 2021-05-18. Retrieved 2021-06-05.
- Sambon, L.W. (1907). "Remarks on Schistosomum mansoni". Journal of Tropical Medicine and Hygiene. 10: 303–304.
- Birch, CA (1974). "Schistosoma mansoni. Sir Patrick Manson, 1844–1922". The Practitioner. 213 (1277): 730–2. PMID 4156405.
- Swanner, Yann A. Meunier; with contributions from Michael Hole, Takudzwa Shumba & B.J. (2014). Tropical Diseases : a Practical Guide for Medical Practitioners and Students. Oxford: Oxford University Press, USA. p. 40. ISBN 9780199997909.
{{cite book}}: CS1 maint: multiple names: authors list (link) - Machado-Silva JR; Galvao C; Oliveira RMF; Presgrave AF; Gomes DC (1995). "Schistosoma mansoni sambon, 1907: Comparative morphological studies of some Brazilian Strains". Rev. Inst. Med. Trop. Sao Paulo. 37 (5): 441–7. doi:10.1590/s0036-46651995000500010. PMID 8729755.
- Braschi S; Borges WC; Wilson RA (September 2006). "Proteomic analysis of the schistosome tegument and its surface membranes". Memórias do Instituto Oswaldo Cruz. 101 (Suppl 1): 205–12. doi:10.1590/S0074-02762006000900032. PMID 17308771.
- Rey, Luíz (1991). Parasitologia. Rio de Janeiro, RJ: Editora Guanabara Koogan S.A. pp. 351–62. ISBN 978-85-277-0189-1.
- Oliveira, M. F.; d'Avila, J. C.; Torres, C. R.; Oliveira, P. L.; Tempone, A. J.; Rumjanek, F. D.; Braga, C. M.; Silva, J. R.; et al. (2000). "Haemozoin in Schistosoma mansoni". Molecular and Biochemical Parasitology. 111 (1): 217–221. doi:10.1016/s0166-6851(00)00299-1. PMID 11087932.
- Erasmus, D. A. (1973). "A comparative study of the reproductive system of mature, immature and "unisexual" female Schistosoma mansoni". Parasitology. 67 (2): 165–183. doi:10.1017/s0031182000046394. PMID 4795964. S2CID 20589225.
- Moné, Hélène; Boissier, Jérôme (2004). "Sexual biology of schistosomes". Advances in Parasitology. 57: 89–189. doi:10.1016/S0065-308X(04)57002-1. ISBN 9780120317578. PMID 15504538.
- Lu, Zhigang; Spänig, Sebastian; Weth, Oliver; Grevelding, Christoph G. (2019). "Males, the Wrongly Neglected Partners of the Biologically Unprecedented Male-Female Interaction of Schistosomes". Frontiers in Genetics. 10: 796. doi:10.3389/fgene.2019.00796. PMC 6743411. PMID 31552097.
- Steinauer, Michelle L. (2009). "The sex lives of parasites: investigating the mating system and mechanisms of sexual selection of the human pathogen Schistosoma mansoni". International Journal for Parasitology. 39 (10): 1157–1163. doi:10.1016/j.ijpara.2009.02.019. PMC 2911351. PMID 19298820.
- Gupta, B. C.; Basch, P. F. (1987). "The role of Schistosoma mansoni males in feeding and development of female worms". The Journal of Parasitology. 73 (3): 481–486. doi:10.2307/3282125. JSTOR 3282125. PMID 3298599.
- Quack, Thomas; Beckmann, Svenja; Grevelding, Christoph G. (2006). "Schistosomiasis and the molecular biology of the male-female interaction of S. mansoni". Berliner und Munchener Tierarztliche Wochenschrift. 119 (9–10): 365–372. PMID 17007463.
- LoVerde, Philip T; Niles, Edward G; Osman, Ahmed; Wu, Wenjie (2004). "Schistosoma mansoni male–female interactions". Canadian Journal of Zoology. 82 (2): 357–374. doi:10.1139/z03-217.
- Popiel, I.; Basch, P. F. (1984). "Reproductive development of female Schistosoma mansoni (Digenea: Schistosomatidae) following bisexual pairing of worms and worm segments". The Journal of Experimental Zoology. 232 (1): 141–150. doi:10.1002/jez.1402320117. PMID 6502090.
- Neves, Renata Heisler; de Lamare Biolchini, Carla; Machado-Silva, José Roberto; Carvalho, Jorge José; Branquinho, Thiago Braga; Lenzi, Henrique Leonel; Hulstijn, Maarten; Gomes, Delir Corrêa (2005). "A new description of the reproductive system of Schistosoma mansoni (Trematoda: Schistosomatidae) analyzed by confocal laser scanning microscopy". Parasitology Research. 95 (1): 43–49. doi:10.1007/s00436-004-1241-2. PMID 15565465. S2CID 23886925.
- Hulstijn, M.; Barros, L. A.; Neves, R. H.; Moura, E. G.; Gomes, D. C.; Machado-Silva, J. R. (2006). "Hermaphrodites and supernumerary testicular lobes in Schistosoma mansoni (Trematoda: Schistosomatidae) analyzed by brightfield and confocal microscopy". The Journal of Parasitology. 92 (3): 496–500. doi:10.1645/GE-3552.1. PMID 16883991. S2CID 20299817.
- Shaw, M. K.; Erasmus, D. A. (1982). "Schistosoma mansoni: the presence and ultrastructure of vitelline cells in adult males". Journal of Helminthology. 56 (1): 51–53. doi:10.1017/s0022149x00035008. PMID 7200108. S2CID 9587355.
- Chong, Tracy; Collins, James J.; Brubacher, John L.; Zarkower, David; Newmark, Phillip A. (2013). "A sex-specific transcription factor controls male identity in a simultaneous hermaphrodite". Nature Communications. 4: 1814. Bibcode:2013NatCo...4.1814C. doi:10.1038/ncomms2811. PMC 3674237. PMID 23652002.
- Hutchison, H.S. (1928). "The pathology of bilharziasis". The American Journal of Pathology. 4 (1): 1–16. PMC 2006716. PMID 19969774.
- Xu, YZ; Dresden, MH (1989). "Schistosoma mansoni: egg morphology and hatchability". The Journal of Parasitology. 75 (3): 481–483. doi:10.2307/3282615. JSTOR 3282615. PMID 2723933.
- Xu, Yi-Zheng; Dresden, Marc H. (1990). "The hatching of schistosome eggs". Experimental Parasitology. 70 (2): 236–240. doi:10.1016/0014-4894(90)90104-K. PMID 2105231.
- Køie, Marianne; Frandsen, Flemming (1976). "Stereoscan observations of the miracidium and early sporocyst of Schistosoma mansoni". Zeitschrift für Parasitenkunde. 50 (3): 335–344. doi:10.1007/BF02462978. PMID 997727. S2CID 8968526.
- Cort, W.W. (1919). "Notes on the eggs and miracidia of the human schistosomes". Univiversity of California Publications in Zoology. 18 (18): 509–519.
- Krishnamurthy, Deepak; Katsikis, Georgios; Bhargava, Arjun; Prakash, Manu (2016). "Schistosoma mansoni cercariae swim efficiently by exploiting an elastohydrodynamic coupling". Nature Physics. 13 (3): 266–271. doi:10.1038/nphys3924.
- Faust, E.C. (1919). "Notes on South African cercariae". The Journal of Parasitology. 5 (4): 164–175. doi:10.2307/3271082. JSTOR 3271082.
- Faust, C.E. (1920). "Criteria for the differentiation of Schistosome larvae". The Journal of Parasitology. 6 (4): 192–194. doi:10.2307/3270844. JSTOR 3270844.
- Mohammed, A.S. (1931). "The secretory glands of the cercariae of S. Haematobium and S. Mansoni from Egypt". Annals of Tropical Medicine & Parasitology. 26 (1): 7–22. doi:10.1080/00034983.1932.11684702.
- Kasschau MR, Byam-Smith MP, Gentry DS, Watson FN (1995). "Influence of pH and temperature on hemolysis by adult Schistosoma mansoni membranes". J. Exp. Zool. 271 (4): 315–22. doi:10.1002/jez.1402710409. PMID 7722474.
- Wilmer, Pat; Stone, Graham; Johnston, Ian (2005). Environmental Physiology of Animals. Blackwell. pp. 677–692. ISBN 9781405107242.
- Ressurreição M, Kirk RS, Rollinson D, Emery AM, Page NM, Walker AJ (2015). "Sensory Protein Kinase Signaling in Schistosoma mansoni Cercariae: Host Location and Invasion". J. Infect. Dis. 212 (11): 1787–97. doi:10.1093/infdis/jiv464. PMC 4633769. PMID 26401028.
- Patocka N, Sharma N, Rashid M, Ribeiro P (2014). "Serotonin signaling in Schistosoma mansoni: a serotonin-activated G protein-coupled receptor controls parasite movement". PLOS Pathog. 10 (1): e1003878. doi:10.1371/journal.ppat.1003878. PMC 3894222. PMID 24453972.
- Carvalho Ode, D (1992). "Intermediate hosts of Schistosoma mansoni in Brazil". Memórias do Instituto Oswaldo Cruz. 87 (Suppl 4): 307–309. doi:10.1590/s0074-02761992000800048. PMID 1343914.
- (in Spanish) Libora M., Morales G., Carmen S., Isbelia S. & Luz A. P. (2010). "Primer hallazgo en Venezuela de huevos de Schistosoma mansoni y de otros helmintos de interés en salud pública, presentes en heces y secreción mucosa del molusco terrestre Achatina fulica (Bowdich, 1822). [First finding in Venezuela of Schistosoma mansoni eggs and other helminths of interest in public health found in faeces and mucous secretion of the mollusc Achatina fulica (Bowdich, 1822)]. Zootecnia Tropical 28: 383–394. PDF.
- Bustinduy, Amaya L.; Charles H., King (2014). "Schistosomiasis". In Farrar, J; White, NJ (eds.). Manson's Tropical Diseases (New ed.). Philadelphia: Saunders [Imprint]. pp. 698–725. doi:10.1016/B978-0-7020-5101-2.00091-1. ISBN 978-0-7020-5101-2.
- Abou-El-Naga, IF (2013). "Biomphalaria alexandrina in Egypt: past, present and future". Journal of Biosciences. 38 (3): 665–672. doi:10.1007/s12038-013-9329-4. PMID 23938396. S2CID 16670424.
- Ross, Allen; Inobaya, Marianette; Olveda, Remigio; Chau, Thao; Olveda, David (2014). "Prevention and control of schistosomiasis: a current perspective". Research and Reports in Tropical Medicine. 2014 (5): 65–75. doi:10.2147/RRTM.S44274. PMC 4231879. PMID 25400499.
- Gryseels, Bruno (2012). "Schistosomiasis". Infectious Disease Clinics of North America. 26 (2): 383–397. doi:10.1016/j.idc.2012.03.004. PMID 22632645.
- Whitfield, PJ; Bartlett, A; Khammo, N; Clothier, RH (2003). "Age-dependent survival and infectivity of Schistosoma mansoni cercariae". Parasitology. 127 (Pt 1): 29–35. doi:10.1017/s0031182003003263. PMID 12885186. S2CID 28975630.
- Oliveira MF, d'Avila JC, Torres CR, et al. (November 2000). "Haemozoin in Schistosoma mansoni". Molecular and Biochemical Parasitology. 111 (1): 217–21. doi:10.1016/S0166-6851(00)00299-1. PMID 11087932.
- Wilson, R. A. (2009). "The saga of schistosome migration and attrition". Parasitology. 136 (12): 1581–1592. doi:10.1017/S0031182009005708. PMID 19265564. S2CID 36830557.
- Beltran S; Boissier J (September 2008). "Schistosome monogamy: who, how, and why?". Trends in Parasitology. 24 (9): 386–91. doi:10.1016/j.pt.2008.05.009. PMID 18674968.
- Loverde PT; Chen L (November 1991). "Schistosome female reproductive development". Parasitology Today. 7 (11): 303–8. doi:10.1016/0169-4758(91)90263-N. PMID 15463396.
- "Schistosoma mansoni Genome Project". Sanger Institute. Retrieved 2007-06-14.
- Le Paslier MC, Pierce RJ, Merlin F, et al. (April 2000). "Construction and characterization of a Schistosoma mansoni bacterial artificial chromosome library". Genomics. 65 (2): 87–94. doi:10.1006/geno.2000.6147. PMID 10783255.
- "Schistosoma mansoni Genome Project". The Institute for Genomic Research. Retrieved 2007-06-14.
- Verjovski-Almeida S; DeMarco R; Martins EA; Guimarães PE; Ojopi EP; Paquola AC; Piazza JP; Nishiyama MY Jr; Kitajima JP; Adamson RE; Ashton PD; Bonaldo MF; Coulson PS; Dillon GP; Farias LP; Gregorio SP; Ho PL; Leite RA; Malaquias LC; Marques RC; Miyasato PA; Nascimento AL; Ohlweiler FP; Reis EM; Ribeiro MA; Sá RG; Stukart GC; Soares MB; Gargioni C; Kawano T; Rodrigues V; Madeira AM; Wilson RA; Menck CF; Setubal JC; Leite LC; Dias-Neto E. (October 2003). "Transcriptome analysis of the acoelomate human parasite Schistosoma mansoni". Nature Genetics. 35 (2): 148–157. doi:10.1038/ng1237. PMID 12973350. S2CID 11387995.
- Berriman M; Haas BJ; LoVerde PT; Wilson RA; Dillon GP; Cerqueira GC; Mashiyama ST; Al-Lazikani B; Andrade LF; Ashton PD; Aslett MA; Bartholomeu DC; Blandin G; Caffrey CR; Coghlan A; Coulson R; Day TA; Delcher A; DeMarco R; Djikeng A; Eyre T; Gamble JA; Ghedin E; Gu Y; Hertz-Fowler C; Hirai H; Hirai Y; Houston R; Ivens A; Johnston DA; Lacerda D; Macedo CD; McVeigh P; Ning Z; Oliveira G; Overington JP; Parkhill J; Pertea M; Pierce RJ; Protasio AV; Quail MA; Rajandream MA; Rogers J; Sajid M; Salzberg SL; Stanke M; Tivey AR; White O; Williams DL; Wortman J; Wu W; Zamanian M; Zerlotini A; Fraser-Liggett CM; Barrell BG; El-Sayed NM. (July 2009). "The genome of the blood fluke Schistosoma mansoni". Nature. 460 (7253): 352–8. Bibcode:2009Natur.460..352B. doi:10.1038/nature08160. PMC 2756445. PMID 19606141.
- "Killer parasites' genes decoded". BBC News. July 16, 2009. Retrieved 2009-07-16.
- Anna V. Protasio; Isheng J. Tsai; Anne Babbage; Sarah Nichol; Martin Hunt; Nishadi De Silva; Tim J.C. Anderson; Richard C. Clark; Claire Davidson; Gary P. Dillon; Nancy E. Holroyd; Philip T. LoVerde; Christine Lloyd; Jacquelline McQuillan; Guilherme Oliveira; Thomas D. Otto; Sophia J. Parker-Manuel; Michael A. Quail; R. Alan Wilson; Adhemar Zerlotini; David W. Dunne; Matthew Berriman. (January 2012). "A systematically improved high quality genome and transcriptome of the human blood fluke Schistosoma mansoni". PLOS Neglected Tropical Diseases. 6 (1): 1455. doi:10.1371/journal.pntd.0001455. PMC 3254664. PMID 22253936.
- Elbaz, Tamer; Esmat, Gamal (2013). "Hepatic and Intestinal Schistosomiasis: Review". Journal of Advanced Research. 4 (5): 445–452. doi:10.1016/j.jare.2012.12.001. PMC 4293886. PMID 25685451.
- Boros DL (July 1989). "Immunopathology of Schistosoma mansoni infection". Clinical Microbiology Reviews. 2 (3): 250–69. doi:10.1128/cmr.2.3.250. PMC 358119. PMID 2504481.
- Guimarães Cavalcanti, Marta; Marcello de Araujo-Neto, João; Mauro Peralta, José (2015). "Schistosomiasis: Clinical management of liver disease". Clinical Liver Disease. 6 (3): 59–62. doi:10.1002/cld.495. PMC 6490649. PMID 31040989.
- Mentink-Kane MM, Cheever AW, Thompson RW, et al. (January 2004). "IL-13 receptor α 2 down-modulates granulomatous inflammation and prolongs host survival in schistosomiasis". Proceedings of the National Academy of Sciences of the United States of America. 101 (2): 586–90. Bibcode:2004PNAS..101..586M. doi:10.1073/pnas.0305064101. PMC 327191. PMID 14699044.
- Gasim, Gasim I; Bella, Abdelhaleem; Adam, Ishag (2015). "Schistosomiasis, hepatitis B and hepatitis C co-infection". Virology Journal. 12 (1): 19. doi:10.1186/s12985-015-0251-2. PMC 4323254. PMID 25889398.
- Wilson RA; Coulson PS (September 2009). "Immune effector mechanisms against schistosomiasis: looking for a chink in the parasite's armour". Trends in Parasitology. 25 (9): 423–31. doi:10.1016/j.pt.2009.05.011. PMC 3686490. PMID 19717340.
- Sayed AA; Simeonov A; Thomas CJ; Inglese J; Austin CP; Williams DL (April 2008). "Identification of oxadiazoles as new drug leads for the control of schistosomiasis". Nat. Med. 14 (4): 407–12. doi:10.1038/nm1737. PMC 2700043. PMID 18345010.
- Ross F, Hernández P, Porcal W, et al. (2012). "Identification of thioredoxin glutathione reductase inhibitors that kill cestode and trematode parasites". PLOS ONE. 7 (4): e35033. Bibcode:2012PLoSO...735033R. doi:10.1371/journal.pone.0035033. PMC 3335049. PMID 22536349.
- Wilson, R. Alan; Coulson, Patricia S. (2009). "Immune effector mechanisms against schistosomiasis: looking for a chink in the parasite's armour". Trends in Parasitology. 25 (9): 423–431. doi:10.1016/j.pt.2009.05.011. PMC 3686490. PMID 19717340.
- Gray, D. J.; Ross, A. G.; Li, Y.-S.; McManus, D. P. (2011). "Diagnosis and management of schistosomiasis". BMJ. 342: d2651. doi:10.1136/bmj.d2651. PMC 3230106. PMID 21586478.
- Utzinger, J.; Becker, S.L.; van Lieshout, L.; van Dam, G.J.; Knopp, S. (2015). "New diagnostic tools in schistosomiasis". Clinical Microbiology and Infection. 21 (6): 529–542. doi:10.1016/j.cmi.2015.03.014. PMID 25843503.
- Utzinger, J; Becker, SL; van Lieshout, L; van Dam, GJ; Knopp, S (June 2015). "New diagnostic tools in schistosomiasis". Clinical Microbiology and Infection. 21 (6): 529–42. doi:10.1016/j.cmi.2015.03.014. PMID 25843503.
- Hunziker, Patrick; Nigo, Maurice Mutro; Salieb-Beugelaar, Georgette B.; Odermatt, Peter; Battegay, Manuel (2019-12-19). "Schistosomiasis: from established diagnostic assays to emerging micro/nanotechnology-based rapid field testing for clinical management and epidemiology". Precision Nanomedicine. 3: 439–458. doi:10.33218/prnano3(1).191205.1.
- Danso-Appiah, A; Olliaro, PL; Donegan, S; Sinclair, D; Utzinger, J (2013). "Drugs for treating Schistosoma mansoni infection". The Cochrane Database of Systematic Reviews. 2 (2): CD000528. doi:10.1002/14651858.CD000528.pub2. PMC 6532716. PMID 23450530.
- "Schistosomiasis: Epidemiology". WHO. Archived from the original on October 20, 2014. Retrieved 2021-06-05.
- Chitsulo, L.; Engels, D.; Montresor, A.; Savioli, L. (2000). "The global status of schistosomiasis and its control". Acta Tropica. 77 (1): 41–51. doi:10.1016/S0001-706X(00)00122-4. PMC 5633072. PMID 10996119.
- van der Werf, Marieke J; de Vlas, Sake J.; Brooker, Simon; Looman, Caspar W.N.; Nagelkerke, Nico J.D.; Habbema, J. Dik F; Engels, Dirk (2003). "Quantification of clinical morbidity associated with schistosome infection in sub-Saharan Africa" (PDF). Acta Tropica. 86 (2–3): 125–139. doi:10.1016/S0001-706X(03)00029-9. PMID 12745133.
- Adenowo, Abiola Fatimah; Oyinloye, Babatunji Emmanuel; Ogunyinka, Bolajoko Idiat; Kappo, Abidemi Paul (2015). "Impact of human schistosomiasis in sub-Saharan Africa". The Brazilian Journal of Infectious Diseases. 19 (2): 196–205. doi:10.1016/j.bjid.2014.11.004. PMC 9425372. PMID 25636189.
- Barakat, Rashida M.R. (2013). "Epidemiology of Schistosomiasis in Egypt: Travel through Time: Review". Journal of Advanced Research. 4 (5): 425–432. doi:10.1016/j.jare.2012.07.003. PMC 4293883. PMID 25685449.
- "DPDx – Schistosomiasis risk and Epidemiology Factors". CDC. Retrieved 2013-11-05.
- Morgan, JA; Dejong, RJ; Snyder, SD; Mkoji, GM; Loker, ES (2001). "Schistosoma mansoni and Biomphalaria: past history and future trends". Parasitology. 123 (Suppl): S211–28. doi:10.1017/s0031182001007703. PMID 11769285. S2CID 23030603.
- Abou-El-Naga IF (2013). "Biomphalaria alexandrina in Egypt: past, present and future the country's of south America namely brazil conspired to bring this parasite to the U.S.A causing an out brake of hepatitis that people are still fighting till this day 2018". J. Biosci. 38 (3): 665–72. doi:10.1007/s12038-013-9329-4. PMID 23938396. S2CID 16670424.
- Rabello, A. (1997). "Diagnosing schistosomiasis". Memórias do Instituto Oswaldo Cruz. 92 (5): 669–676. doi:10.1590/S0074-02761997000500021. PMID 9566238.
- Farley, J. (2003). Bilharzia: A History of Imperial Tropical Medicine. Cambridge (UK): Cambridge University Press. pp. 48–50. ISBN 9780521530606.
- Lofty, W.M. (2009). "Human schistosomiasis in Egypt: Historical review, assessment of the current picture and prediction of the future trends". Journal of the Medical Research Institute. 30 (1): 1–7.
- Akl, M.M. (2009). "Bilharziasis: A Granulomatous Parasitic Disorder with Grave Implications". In Mansourian, B.P.; Wojtczak, A.; Sayers, B.M (eds.). Medical Sciences – Volume I. Oxford (UK): Eolss Publishers Co. Ltd. pp. 374–400. ISBN 978-1-84826-733-6.
- Tan, SY; Ahana, A (2007). "Theodor Bilharz (1825–1862): discoverer of schistosomiasis" (PDF). Singapore Medical Journal. 48 (3): 184–185. PMID 17342284.
- Cox, F. E. G. (2002). "History of Human Parasitology". Clinical Microbiology Reviews. 15 (4): 595–612. doi:10.1128/CMR.15.4.595-612.2002. PMC 126866. PMID 12364371.
- Falcao, EC (1959). "Professor Piraja da Silva, incontestable discoverer of Schistosoma mansoni". Zeitschrift für Tropenmedizin und Parasitologie. 10: 146–153. PMID 13821378.
- Katz, Naftale (2008). "The discovery of Schistosomiasis mansoni in Brazil". Acta Tropica. 108 (2–3): 69–71. doi:10.1016/j.actatropica.2008.05.002. PMID 18597732.
- Silva, Pirajá da (1917). Schistosomes in Bahia. Bahia, Brazil: Imprensa Official do Estado. p. 32.
- Macpherson, C.N.L.; Craig, P.S. (1991). "Animal reservoirs of schistosomiasis". Parasitic helminths and zoonoses in Africa. Springer, Dordrecht. pp. 224–236. doi:10.1007/978-94-011-3054-7_8. ISBN 978-94-010-5358-7.
External links
 Media related to Schistosoma mansoni at Wikimedia Commons
Media related to Schistosoma mansoni at Wikimedia Commons