Stroke Belt
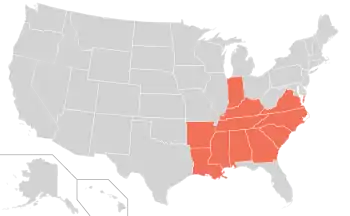
The Stroke Belt or Stroke Alley is a region in the southeastern United States that has been recognized by public health authorities for having an unusually high incidence of stroke and other forms of cardiovascular disease. It is usually defined as a 11-state region consisting of Alabama, Arkansas, Georgia, Indiana, Kentucky, Louisiana, Mississippi, North Carolina, South Carolina, Tennessee, and Virginia. It is often disputed if Texas belongs in the Stroke Belt. [1]
Although many possible causes for the high stroke incidence have been investigated, the reasons for the phenomenon have not been determined.
Geographic scope
The stroke belt is typically defined to include the states of Alabama, Arkansas, Georgia, Kentucky, Louisiana, Mississippi, North Carolina, South Carolina, Tennessee, and Virginia.[2] In 1980 these 11 states had age-adjusted stroke mortality rates more than 10% above the national average.[3]
Some investigators also consider North Florida to be a part of the stroke belt, based on a stroke mortality rate higher than several states included in the region.[4] East Texas also is characterized as a stroke belt.[5]
History of observations

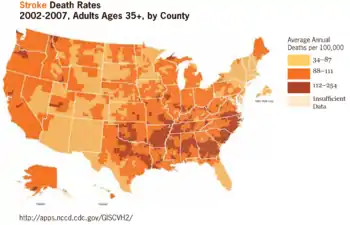
The stroke belt was first identified in 1962 by Centers for Disease Control (CDC) researchers who noted a concentration of high stroke death rates in the Atlantic coastal plain counties of North Carolina, South Carolina and Georgia.[6] Similar high stroke rates were later observed in the Mississippi Delta region as well.[6][7]
Analysis by the CDC of U.S. mortality statistics from the period 1991 to 1998 found that for both blacks and whites the counties with the highest stroke death rates were in the southeastern states and the Mississippi Delta region. Stroke death rates for states ranged from a high of 169 per 100,000 in South Carolina to a low of 89 per 100,000 in New York.[8] While most observational studies have focused primarily on stroke incidence in adults, in 2004 researchers reported that children in the eleven stroke belt states also have an increased risk of death from ischemic and hemorrhagic stroke compared with children in other states.[9]
Glymour et al. (2007) reported that adults who had resided in the stroke belt during childhood and had moved outside the region had higher stroke risk at ages 50 and older than adults who grew up in areas with lower stroke incidence.[10] A study reported in 2011 found that people over age 45 living in the eight "stroke belt" states of Alabama, Arkansas, Georgia, Louisiana, Mississippi, North Carolina, South Carolina and Tennessee had an 18 percent higher incidence of cognitive decline than people in other U.S. regions. Another researcher noted that, "Stroke by itself is a major contributor to cognitive impairment and dementia."[11] Other researchers have made similar observations.[12][13]
In 2011, CDC researchers mapped the occurrence of diabetes in the U.S. by county, finding that highest prevalence of diabetes is in a "diabetes belt" that has extensive overlap with the stroke belt.[14][15]
Hypotheses on causation
The causes of the elevated incidence of stroke in the stroke belt region have not been determined.[7][10][16][17] Numerous possible contributing factors have been identified, including hypertension, low socioeconomic status, diet, cultural lifestyle, quality of healthcare facilities, smoking, and infections.[18] Among the specific factors that have been proposed or studied are the following:
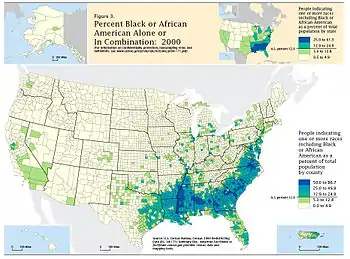
- It has been suggested that the higher stroke death rates in the stroke belt are due to the region's high African American population, because African Americans' stroke death rates are higher than the national average.[19] However, because White people also have higher rates of stroke death in the stroke belt than in other parts of the country, the higher death rates in the stroke belt cannot be attributed solely to the region's higher proportion of African Americans.[3]
- In the early 1990s it was hypothesized that selenium deficiency in the soils of the coastal plain might be a causative factor.[20] The subsequent recognition of high stroke incidence in areas with different soil characteristics led researchers to reject this hypothesis.[21]
- Some observers have assumed that more stroke belt residents suffer from untreated hypertension. However, researchers have found that residents of the southern United States are as likely to be aware of hypertension and receiving treatment as residents of other U.S. regions.[18] Additionally, researchers who documented the region's elevated incidence of pediatric stroke noted that "If the stroke belt is solely caused by regional differences in atherosclerotic stroke risk factors, it should not apply to children."[9]
- It has been suggested that one cause of higher mortality may be the predominantly rural character of the region, which increases the distances that patients must travel to obtain emergency medical treatment.[17] Regional differences in standards of medical care have also been suggested as a contributing factor. In one study, researchers found that patients discharged from hospitals in the stroke belt after suffering acute myocardial infarction were less likely to be treated with warfarin than patients in most other U.S. regions.[22]
- Glymour et al. (2007) suggested that the higher stroke incidence in the stroke belt is related to experiences or exposures in childhood.[10]
- It has been proposed that poverty and malnutrition in previous generations, which resulted in poor maternal prenatal nutrition and low birth weights, led to a predisposition to cardiovascular disease in adult life.[23]
- Diets high in fried and high-fat foods (such as fried chicken or fried fish[24]), which are prevalent in the region, are thought to contribute to higher risk.[6]
- The same geographical area also has a higher than national average incidence of lung cancer, as it is where much of the tobacco in the United States is grown. Smoking is reputed to be the strongest contributing factor of developing both diseases.[25]
Public health initiatives to reduce stroke incidence in the region
The U.S. federal government has conducted public health programs specifically aimed at reducing stroke incidence and mortality in the stroke belt. In the 1990s the Stroke Belt Initiative operated in eleven stroke belt states, providing nutrition education, blood pressure screening, smoking cessation programs, weight loss programs, and other health promotion and public education initiatives targeted at stroke risk factors.[3]
In 2004, the Stroke Belt Elimination Initiative of the U.S. Department of Health and Human Services awarded grants aimed at reducing the high incidence of stroke and high rates of stroke death and disability in the seven states with the highest rates of stroke (Alabama, Arkansas, Georgia, Mississippi, North Carolina, South Carolina, and Tennessee).[16]
Origins
The term "stroke belt" is modeled after similar terms used for U.S. regions such as "snowbelt" and "Sun Belt",[26] which extend the analogy to the belt as an article of clothing. The coastal plain counties of the Carolinas and Georgia — where the stroke belt phenomenon was first described, and where stroke incidence is highest — are sometimes called the "buckle of the stroke belt" or the "stroke buckle".[27][28]
See also
References
- Emily Ramshaw, East Texans’ Bad Health and Bad Habits Promote a ‘Stroke Belt’, The New York Times, January 14, 2011
- "What is the Stroke Belt?". Live Science. 27 March 2013.
- Stroke Belt Initiative: Project Accomplishments and Lessons Learned Archived 2008-10-01 at the Wayback Machine, National Heart, Lung, and Blood Institute, National Institutes of Health; reports on a conference that occurred in 1996
- Siegel PZ, Wolfe LE, Wilcox D, Deeb LC (1992). "North Florida is part of the stroke belt". Public Health Rep. 107 (5): 540–3. PMC 1403695. PMID 1410234.
- Emily Ramshaw, East Texans’ Bad Health and Bad Habits Promote a ‘Stroke Belt’, The New York Times, January 14, 2011
- Combating Southern Fried Fat, CBS News, February 14, 2005
- Casper ML, Wing S, Anda RF, Knowles M, Pollard RA (May 1995). "The shifting stroke belt. Changes in the geographic pattern of stroke mortality in the United States, 1962 to 1988". Stroke. 26 (5): 755–60. doi:10.1161/01.str.26.5.755. PMID 7740562.
- CDC Releases Atlas of Stroke Mortality Archived 2008-10-11 at the Wayback Machine, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention & Health Promotion, February 20, 2003
- Fullerton HJ, Elkins JS, Johnston SC (Jul 2004). "Pediatric Stroke Belt: geographic variation in stroke mortality in US children". Stroke. 35 (7): 1570–3. doi:10.1161/01.STR.0000130514.21773.95. PMID 15178830.
- Glymour MM, Avendaño M, Berkman LF (Sep 2007). "Is the 'stroke belt' worn from childhood?: risk of first stroke and state of residence in childhood and adulthood". Stroke. 38 (9): 2415–21. doi:10.1161/STROKEAHA.107.482059. PMID 17673716.
- Mary Elizabeth Dallas, U.S. Southeast 'Stroke Belt' Also Shows Higher Rates of Cognitive Decline, Health Day (MedLine Plus), May 26, 2011
- El-Saed A, Kuller LH (Sep 2007). "Is the stroke belt worn from childhood?: current knowledge and future directions". Stroke. 38 (9): 2403–4. doi:10.1161/STROKEAHA.107.487405. PMID 17673801.
- Kuźma, Elżbieta; Lourida, Ilianna; Moore, Sarah F.; Levine, Deborah A.; Ukoumunne, Obioha C.; Llewellyn, David J. (August 2018). "Stroke and dementia risk: A systematic review and meta-analysis". Alzheimer's & Dementia. 14 (11): 1416–1426. doi:10.1016/j.jalz.2018.06.3061. hdl:2027.42/152961. ISSN 1552-5260. PMC 6231970. PMID 30177276.
- Nathan Seppa (March 8, 2011). "'Diabetes Belt' Outlined; Region of high prevalence stretches across Deep South and Appalachia". U.S. News & World Report.
- "Researchers find U.S. "diabetes belt"". Reuters. March 8, 2011. Archived from the original on March 9, 2015. Retrieved July 2, 2017.
- "HHS Announces Initiative to Reduce the Incidence of Stroke in Stroke Belt States" (press release). Department of Health and Human Services. August 5, 2004. Archived from the original on October 31, 2004.
- Stroke Mystery, Newsweek, November 8, 2005
- Lisa Nainggolan, Hypertension may not be the whole story in the Stroke Belt, Medscape Medical News, February 9, 2005
- African American males age 45 to 54 have a threefold greater risk of ischemic stroke than white males in the same age range.
- Felicity Barringer, Toward Solving the Mystery Of the American 'Stroke Belt' , The New York Times, July 29, 1992
- Introduction Archived 2009-11-24 at the Wayback Machine, Atlas of Stroke Mortality: Racial, Ethnic, and Geographic Disparities in the United States (Casper ML, Barnett E, Williams GI Jr., Halverson JA, Braham VE, Greenlund KJ). Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, 2003
- Stroke Belt — A Standard of Care Phenomenon?, Family Practice News, June 1, 2000
- Risk may be associated with mother's health Archived 2008-10-11 at the Wayback Machine, Health & Medicine Week, July 14, 2003
- Bakalar, Nicholas (3 January 2011). "Diet: Fried Fish Is Seen as a 'Stroke Belt' Culprit". The New York Times. Retrieved 3 January 2012.
- Peto, R; Lopez AD; Boreham J; et al. (2006). Mortality from smoking in developed countries 1950–2000: Indirect estimates from National Vital Statistics. Oxford University Press. ISBN 978-0-19-262535-9.
- WordSpy website, posted on March 25, 2003
- Howard G, Anderson R, Johnson NJ, Sorlie P, Russell G, Howard VJ (May 1997). "Evaluation of social status as a contributing factor to the stroke belt region of the United States". Stroke. 28 (5): 936–40. doi:10.1161/01.str.28.5.936. PMID 9158628. Archived from the original on July 20, 2012.
- I, Shrira; N, Christenfeld; G, Howard (2008). "Exposure to the US Stroke Buckle as a Risk Factor for Cerebrovascular Mortality". Neuroepidemiology. 30 (4): 229–233. doi:10.1159/000128102. PMC 2821430. PMID 18437029.
External links
- Atlas of Stroke Mortality: Racial, Ethnic and Geographic Disparities in the United States, Centers for Disease Control and Prevention
- Stroke Belt Consortium
- Stroke Statistics, Internet Stroke Center at Washington University