Fibrous joint
In anatomy, fibrous joints are joints connected by fibrous tissue, consisting mainly of collagen. These are fixed joints where bones are united by a layer of white fibrous tissue of varying thickness. In the skull the joints between the bones are called sutures. Such immovable joints are also referred to as synarthroses.
| Fibrous joint | |
|---|---|
 Fibrous joints | |
| Details | |
| Identifiers | |
| Latin | articulatio fibrosa, junctura fibrosa |
| TA98 | A03.0.00.004 |
| TA2 | 1517 |
| FMA | 7492 |
| Anatomical terminology | |
Types
Most fibrous joints are also called "fixed" or "immovable". These joints have no joint cavity and are connected via fibrous connective tissue.
- Sutures: The skull bones are connected by fibrous joints called sutures.[1] In fetal skulls the sutures are wide to allow slight movement during birth. They later become rigid (synarthrodial).
- Syndesmosis: Some of the long bones in the body such as the radius and ulna in the forearm are joined by a syndesmosis (along the interosseous membrane). Syndemoses are slightly moveable (amphiarthrodial). The distal tibiofibular joint is another example.
Sutures
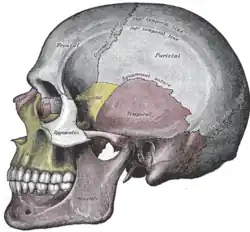
A suture is a type of fibrous joint that is only found in the skull (cranial suture). The bones are bound together by Sharpey's fibres. A tiny amount of movement is permitted at sutures, which contributes to the compliance and elasticity of the skull. These joints are synarthroses.[1] It is normal for many of the bones of the skull to remain unfused at birth. The fusion of the skull's bones before birth is known as craniosynostosis. The term "fontanelle" is used to describe the resulting "soft spots". The relative positions of the bones continue to change during the life of the adult (though less rapidly), which can provide useful information in forensics and archaeology. In old age, cranial sutures may ossify (turn to bone) completely.[3] The joints between the teeth and jaws (gomphoses) and the joint between the mandible and the cranium, the temporomandibular joint, form the only non-sutured joints in the skull.
Types of sutures
- Serrate sutures – similar to a denticulate suture but the interlocking regions are serrated rather than square. Eg: Coronal suture, sagittal Sutures.
- Plane sutures – edges of the bones are flush with each other as in a normal butt joint. Eg: Internasal suture.
- Limbous sutures – edges are bevelled so the plane of the suture is sloping as in a mitre joint. Eg: Temporo-parietal suture.
- Schindylesis – formed by two bones fitting into each other similar to a bridle joint. Eg: Palatomaxillary suture.
- Denticulate sutures – the edges slot into each other as in a finger joint. Eg: Lambdoid suture.
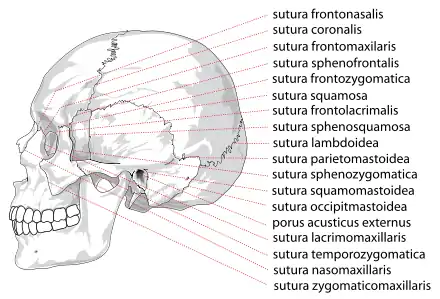
List of sutures
Most sutures are named for the bones they articulate, but some have special names of their own.
Visible from the side
- Coronal suture – between the frontal and parietal bones
- Lambdoid suture – between the parietal and occipital bones and continuous with the occipitomastoid suture
- Occipitomastoid suture – between the occipital and temporal bones and continuous with the lambdoid suture
- Sphenofrontal suture
- Sphenoparietal suture
- Sphenosquamosal suture
- Sphenozygomatic suture
- Squamosal suture – between the parietal and the temporal bone
- Zygomaticotemporal suture
- Zygomaticofrontal suture
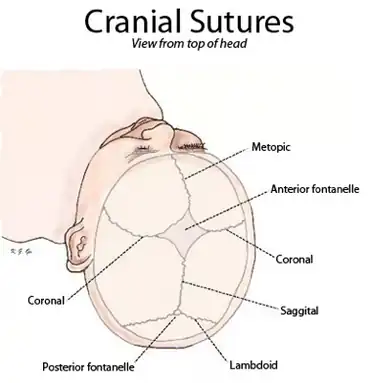
Visible from the front or above
- Frontal suture / Metopic suture – between the two frontal bones, prior to the fusion of the two into a single bone
- Sagittal suture – along the midline, between parietal bones
Visible from below or inside
Gallery
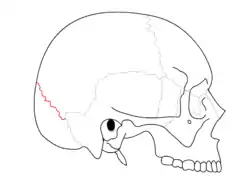 Lambdoid suture
Lambdoid suture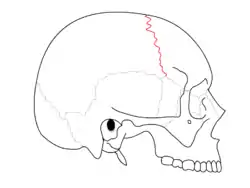 Coronal suture
Coronal suture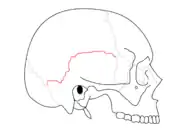 Squamosal suture
Squamosal suture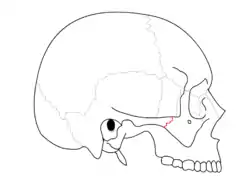 Zygomaticotemporal suture
Zygomaticotemporal suture Sagittal suture.
Sagittal suture. Sagittal suture.
Sagittal suture. Sagittal suture.
Sagittal suture. Top view of cranial suture.
Top view of cranial suture.
Syndesmosis
A syndesmosis is a slightly mobile[4] fibrous joint in which bones such as the tibia and fibula are joined together by connective tissue. An example is the distal tibiofibular joint. Injuries to the ankle syndesmosis are commonly known as a "high ankle sprain". Although the syndesmosis is a joint, in the literature the term syndesmotic injury is used to describe injury of the syndesmotic ligaments. It comes from the Greek σύν, syn (meaning "with") and δεσμός, desmos (meaning "a band").[5] Syndesmosis sprains have received increasing recognition during recent years because of a heightened awareness of the mechanism, symptoms, and signs of injury.[6]
Diagnosis of a syndesmotic injury
Diagnosis of syndesmosis injuries by physical examination is often straightforward. Physical examination findings that are often positive include the squeeze test and the external rotation test. Patients with high-grade syndesmosis injuries often cannot perform a single-leg heel raise. Patients report pain in varying degrees over the anterior and often posterior distal fibular joint.[7]
Syndesmotic tear
The severity of acute syndesmosis injury is rated from grade I to III by several authors. A grade I injury is a partial anteroinferior tibiofibular ligament tear, meaning the exorotation and squeeze tests are negative for this grade. Grade II injury is a complete anteroinferior tibiofibular ligament and inferior interosseous ligament tear, meaning that squeeze test and exorotation are positive. This results in the injury being stabilized with immobilization but not operatively stabilized. A grade III injury is a complete anteroinferior tibiofibular ligament tear including a (partial) interosseous ligament tear and deltoid ligament avulsion, meaning the joint is unstable and positive on the exorotation and squeeze tests. This grade requires operative stabilization.[8] If the syndesmosis is torn apart as result of bone fracture, surgeons will sometimes fix the relevant bones together with a syndesmotic screw, temporarily replacing the syndesmosis, or with a tightrope fixation, which is called Syndesmosis Procedure.[9][10] The screw inhibits normal movement of the bones and, thereby, the corresponding joint(s). When the natural articulation is healed, the screw may be removed. The tightrope fixation with elastic fiberwire suture on the other hand allows physiologic motion of the ankle and may be permanent.
Gomphosis
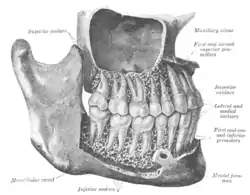
A gomphosis, also known as a dentoalveolar syndesmosis,[11] or 'peg and socket joint'[12] is a joint that binds the teeth to bony teeth sockets in the maxillary bone and mandible. The fibrous connection between a tooth and its socket is a periodontal ligament. Specifically, the connection is made between the maxilla or mandible to the cementum of the tooth.
The motion of a gomphosis is minimal, though considerable movement can be achieved over time—the basis of using braces to realign teeth. The joint can be considered a synarthrosis.[13]
The gomphosis is the only joint-type in which a bone does not join another bone, as teeth are not technically bone. In modern, more anatomical, joint classification, the gomphosis is simply considered a fibrous joint because the tissue linking the structures is ligamentous. It has been suggested that this permanent soft-tissue attachment was a critical requisite in the evolution of the mammalian (synapsid) tusk.[14]
A gomphosis is a specialized fibrous joint in which a conical process or peg of one bone fits into a hole or socket in another bone. (gomphos is a Greek word meaning bolt). Small quantity of fibrous tissue holds the bones together. No movement is possible at such peg-and-socket joints.
References
- "Module – Introduction to Joints". Archived from the original on 2007-12-17. Retrieved 2008-01-29.
- Tomco R. "Fibrous Joints". AnatomyOne. Amirsys, Inc. Archived from the original on 2013-01-16. Retrieved 2012-09-28.
- Harth S, Obert M, Ramsthaler F, Reuss C, Traupe H, Verhoff MA (April 2009). "Estimating age by assessing the ossification degree of cranial sutures with the aid of Flat-Panel-CT". Legal Medicine. 11 Suppl 1 (Supp.1): S186-9. doi:10.1016/j.legalmed.2009.01.091. PMID 19261532.
- Juneja, Pallavi; Munjal, Akul; Hubbard, John B. (2022), "Anatomy, Joints", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 29939670, retrieved 2022-04-26
- Arnold MA, Bryce D. "Arnold's Glossary of Anatomy". The University of Sydney.
- Jones MH, Amendola A (February 2007). "Syndesmosis sprains of the ankle: a systematic review". Clinical Orthopaedics and Related Research. 455: 173–5. doi:10.1097/BLO.0b013e31802eb471. PMID 17146360. S2CID 13598905.
- Metzler AV, Johnson DL (March 2013). "Dynamically unstable syndesmosis injuries". Orthopedics. 36 (3): 209–11. doi:10.3928/01477447-20130222-07. PMID 23464940.
- Valkering KP, Vergroesen DA, Nolte PA (December 2012). "Isolated syndesmosis ankle injury". Orthopedics. 35 (12): e1705–10. doi:10.3928/01477447-20121120-13. PMID 23218625.
- Porucznik MA (May 2008). "Screw vs. tightrope fixation for syndesmotic fractures". AAOS Now. American Academy of Orthopaedic Surgeons. Archived from the original on 14 June 2010.
- "Arthrex - TightRope®". www.arthrex.com.
- "Dentoalveolar syndesmosis". TheFreeDictionary.com.
- Betts, J. Gordon (2013). "9.2 Fibrous joints". Anatomy & physiology. Houston, Texas: OpenStax. ISBN 978-1-947172-04-3. Retrieved 16 April 2023.
- Billy A. "Articulations". Douglas College. Archived from the original on 2007-01-04. Retrieved 2008-01-29.
- Whitney, M.R.; Angielczyk, K.D.; Peecook, B.R.; Sidor, C.A. (2021). "The evolution of the synapsid tusk: insights from dicynodont therapsid tusk histology". Proceedings of the Royal Society B. 288 (1961): 20211670. doi:10.1098/rspb.2021.1670. PMC 8548784. PMID 34702071.