Weight management
Weight management refers to behaviors, techniques, and physiological processes that contribute to a person's ability to attain and maintain a healthy weight.[1][2] Most weight management techniques encompass long-term lifestyle strategies that promote healthy eating and daily physical activity.[3] Moreover, weight management involves developing meaningful ways to track weight over time and to identify ideal body weights for different individuals.[4]
| Part of a series on |
| Human body weight |
|---|

Weight management strategies most often focus on achieving healthy weights through slow but steady weight loss, followed by maintenance of an ideal body weight.[5] However, weight neutral approaches to health have also been shown to result in positive health outcomes.[6][7]
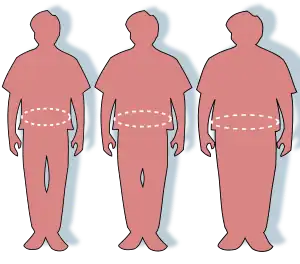
Understanding the basic science of weight management and strategies for attaining and maintaining a healthy weight is very important because obesity is a risk factor for development of many chronic diseases, like Type 2 diabetes, hypertension and cardiovascular disease.[1][5][8]
Key factors
There are many factors that contribute to a person's weight, including: diet, physical activity, genetics, environmental factors, health care support, medications, and illnesses.[5][9][10][11] Each of these factors affect weight in different ways and to varying degrees, but health professionals most often stress the importance of diet and physical activity because they can be affected by conscious behavior modification.[9][12] Attaining a healthy weight involves recognition of general techniques such as portion sizing, self-monitoring, and daily diet consistency.[13] Once this healthy weight has been attained, maintaining this stable weight additionally involves physical activity and control of an individual's environment and eating patterns.[14] Furthermore, healthcare support in the form of primary care medical supervision and following up over time has been shown to be helpful for long-term weight management.[15]
The following is a review of some of the key components of weight management in humans.
Energy balance
The science behind weight management is complex, but one of the key concepts that governs weight management is Energy Balance.[9] Energy Balance is the phrase used to describe the difference between the number of calories a person consumes and the number of calories that same person expends (a.k.a. burns) in a given time period.[9] There are three possible scenarios when it comes to the energy balance equation:
- Calories consumed (food, drink) = Calories expended (basal metabolic rate, physical activity, thermogenic effect of food, acute illness)
- Outcome: Weight remains unchanged
- Calories consumed > Calories expended
- Also known as Positive Energy Balance
- Outcome: Weight increases
- Calories consumed < Calories expended
- Also known as Negative Energy Balance
- Outcome: Weight decreases[9]
The calories a person consumes come from food and drink intake.[9] The calories a person expends comes from their basal metabolic rate and their daily physical activity.[5] The human body is very good at maintaining a neutral energy balance, particularly with a diet composed of fruits, vegetables, and meats so that calories consumed do not substantially exceed calories expended in a given time period and vice versa.[5] This energy balance is regulated by hormones like Leptin (suppresses), Ghrelin (stimulates), and Cholecystokinin (suppresses) which either suppress or stimulate appetite.[5]

Diet
The quantity of food and drink consumed by an individual may play a role in weight management, as may the types of food and drink a person consumes.[5][9][12] For example, intake of sweetened drinks such as sodas or juices can lead to increased energy intake that is not neutralized by a decrease in accompanying food intake.[5] Increased portion sizes may also lead to increased energy intake.[5]
Physical activity

Physical activity can be related to a person's professional activities, non-work related daily activities like walking or cycling, or it can be in the form of activities such as recreation or team sports. [5] The specific type of activity can be tailored to populations such as children, pregnant women, and elderly adults.[5] Tailored activity to one's fitness level also encourages the body to heal properly and prevent any injuries as a result of exercise.[16]
Physical inactivity leads to less energy expenditure and is a factor that impacts obesity rates in both children and adults.[17] Physical inactivity has become a worldwide concern since inactivity also elevates the risk of heart disease.[16] Regular physical activity can reduce the risk for noncommunicable diseases like diabetes, heart disease, and dyslipidemia (high cholesterol). [5]
Basal metabolic rate
Basal metabolic rate (BMR) is one of the main components of a person's daily energy expenditure. It is defined as the amount of energy that is expended during a given amount of time by a person at rest. This energy at rest is used to pump blood throughout the body, maintain proper brain function, break down toxins, and ensure other bodily functions. Technically speaking, BMR is the energy the body expends during the following specific conditions: immediately after waking up, while in a resting state, and after fasting for 12–14 hours. Sometimes the term Resting Metabolic (RMR) is used in place of BMR, but RMR is not solely measured under the previously listed stringent conditions and it is about 10% more than BMR.[18]
The BMR is directly proportional to a person's lean body mass.[5][18] In other words, the more lean body mass a person has, the higher their BMR. BMR is also affected by acute illnesses and increases with burns, fractures, infections, fevers, etc. It can be measured via direct and indirect calorimetry. However, it is also possible to approximately estimate BMR using several equations that factor in a person's age, sex, height, and weight.[18] Some of the most popular and accurate equations used to calculate BMR are the original Harris-Benedict equations, the revised Harris-Benedict equations, and the Mifflin St. Jeor equation.[19]
The original Harris-Benedict Equations are as follows:
- BMR (Males) in Kcals/day = 66.47 + 13.75 (weight in kg) + 5.0 (height in cm) - 6.76 (age in years)
- BMR (Females) in Kcals/day = 655.1 + 9.56 (weight in kg) + 1.85 (height in cm) – 4.68 (age in years)[19]
The revised Harris-Benedict Equations are as follows:
- BMR (Males) in Kcals/day = 88.36 + 13.40 (weight in kg) + 4.8 (height in cm) – 5.68 (age in years)
- BMR (Females) in Kcals/day = 447.59 + 9.25 (weight in kg) + 3.10 (height in cm) – 4.33 (age in years)[19]
The Mifflin St. Jeor Equation is as follows:
- BMR (Males) in Kcals/day = 9.99 (weight in kg) + 6.25 (height in cm) – 4.92 (age in years) + 5
- BMR (Females) in Kcals/day = 9.99 (weight in kg) + 6.25 (height in cm) – 4.92 (age in years) – 161[19]
The Mifflin St. Jeor Equation has been found to be the most accurate predictor of BMR compared to BMR measured by direct and indirect calorimetry.[19]
Body mass index
Body mass index (BMI) is a value used to get a general sense of a person's overall mass and is calculated using a person's height and weight. It is more often used than weight alone to determine if an individual is underweight, normal weight, overweight, or obese. The following two equations can used to calculate BMI depending on the units used for height (meters vs. inches) and weight (kilograms vs. pounds):[5]

or

Though BMI is often used to help assess for excess weight, it is not a perfect representation of a person's body fat percentage. For example, an individual can have a higher than normal BMI but a normal body fat percentage if they have higher than average muscle mass. This is because excess muscle contributes to a higher weight. Since BMI is not a perfect representation of a person's body fat percentage, other measurements like waist circumference are often used to better assess for unhealthy excess weight.
The following table shows how different ranges of BMIs are often categorized into underweight, normal weight, overweight, and obese:[5]
| Category[20] | BMI |
|---|---|
| Underweight | < 18.5 |
| Normal Weight | 18.5 – 24.9 |
| Overweight | 25.0 – 29.9 |
| Obesity (Class I) | 30.0 – 34.9 |
| Obesity (Class II) | 35.0 – 39.9 |
| Obesity (Class III) | ≥ 40.0 |
On average, groups of people with "obese" BMIs may have a higher risk of developing illnesses like diabetes, hypertension, dyslipidemia (high cholesterol), liver disease, and some cancers. "Underweight" BMIs may indicate malnutrition or other health problems. However, BMI has limitations when used to describe individual health rather than describing populations of people. [5]
Complicating factors
Thermogenic effect of food
The thermogenic effect of food is another component of a person's daily energy expenditure and refers to the amount of energy it takes the body to digest, absorb, and metabolize nutrients in the diet.[5] The amount of energy expended while processing food differs by individual but on average it amounts to about 10% the number of calories consumed during a given time period.[5][18] Processing proteins and carbohydrates has more of a thermogenic effect than does processing fats.[5]
Medications
Certain medications can cause either weight loss or weight gain.[5] Such side effects are often listed for each medication and should be considered when attempting to manage a person's weight.[5]
Metanalysis has shown that phentermine and topiramate, pramlintide, naltrexone, bupropion, and liraglutide have been shown to induce weight loss.[21] Semaglutide is another anti-obesity drug that is also used for blood sugar control.[22]
Diseases
Medical conditions associated with weight gain include hypothyroidism,[23] Cushing's syndrome, Polycystic Ovary Syndrome (PCOS), and congestive heart failure.[5][24] Medical conditions such as cancer, gastrointestinal illness, psychiatric disorders, infections, endocrine disorders, and neurologic disorders may lead to weight loss.[5]
Commonly associated with weight gain
Polycystic ovary syndrome (PCOS), which is characterized by insulin resistance and hyperandrogenism, is a common condition that has been linked to obesity.[25] A combination of genetics, lifestyle, and environment appear to contribute to the hormonal changes responsible for weight gain and obesity seen in individuals with PCOS.[25]There appears to be a bidirectional relationship between obesity and PCOS, whereby PCOS increases the risk of obesity and similarly, obesity has been found to exacerbate PCOS hormonal differences and clinical symptoms.[25] [26]

Obesity has been linked with pancreatic β-cell dysfunction and insulin resistance.[27] In diabetes, impaired β-islet cells are responsible for the lack of blood glucose control.[27] Individuals with a higher body mass index concerning for obesity may have increased levels of hormones, proinflammatory markers, and glycerol, which can contribute to insulin resistance.[27] The combined effects of impaired pancreatic β-islet cells and insulin resistance increase the likelihood of developing diabetes.[27]
In individuals with blood sugar levels in the prediabetic range, weight loss was demonstrated to have many benefits including improved glycemic control and a reduced risk of developing type 2 diabetes.[28]
Commonly associated with weight loss
Common gastrointestinal disorders associated with weight loss are malabsorption due to Celiac disease or chronic pancreatitis.[5] Depression and eating disorders such as anorexia nervosa can also contribute to weight loss.[5] Infectious causes of weight loss include HIV/AIDS.[5]
While Type 1 diabetes has been found to cause weight loss, type 2 diabetes has been associated with weight gain.[5] Other endocrine causes of weight loss include hyperthyroidism and chronic adrenal insufficiency.[5]
Intentional weight loss
Diets
As weight loss depends partly on calorie intake, different kinds of calorie-reduced diets, such as those emphasizing particular macronutrients (low-fat, low-carbohydrate, etc.), have been shown to be equally effective as weight loss tools.[29][30][31][32][33][34][35] Nonetheless, a low-saturated fat diet complemented with high fiber can be helpful for those who are found to be obese based on BMI.[12] Furthermore, a low-carbohydrate diet can have the added benefits of blood sugar control in those with Type 2 Diabetes Mellitus.[12] A low-carbohydrate diet can also improve weight loss, HDL, and cholesterol in certain individuals.[36] Compared to a typical diet, low-carbohydrate, low-fat, and moderate macronutrient diets can all positively impact weight loss.[35] However, weight regain is common, and the outcome of a diet can vary widely depending on the individual.[12][30][33][37] Rather than focusing on the nuances of each diet type, molding one diet in a way that the person can continuously adhere in the long-term could be beneficial for weight loss.[5]
- DASH diet
The Dietary Approaches to Stop Hypertension (DASH) diet focuses on increasing the consumption of fruits, vegetables, whole grains and low-fat dairy products.[12] [38][39] DASH offers an intervention to manage elevated blood pressures and prevent cardiovascular disease non-pharmacologically.[39][40][41][42] In addition, combining the DASH diet with a reduced sodium intake will further decrease blood pressure, but is not required for therapeutic effect.[38] This is because it has been proven to be effective at a wide range of sodium intake levels.[38] More recent reviews of DASH have continued to advocate its efficacy as an affordable weight loss tool, but stress that diet adherence is key to produce the desired results.[43]

- Mediterranean diet
The Mediterranean diet involves eating fruits, vegetables, whole grains and beans while replacing butter with extra-virgin olive oil and limiting red meats, dairy, sweets, and processed foods.[44] It has been shown to be effective for long term weight loss with added cardiovascular health benefits.[12][45] For example, the Mediterranean diet can lead to decreased triglyceride and lipid levels as well as improved blood pressure readings.[34] It can also improve blood sugar levels in those diagnosed with Type 2 Diabetes Mellitus.[34]
- Ketogenic diet
The ketogenic or "keto" diet involves intake of less than 50 g of carbohydrates daily along with increased fat and protein amounts.[46] One type of ketogenic or low carbohydrate diet is the "Atkins" Diet, which does not restrict protein and fat amounts.[12] However, there are other ketogenic diets that place restrictions on the total amount of daily proteins and fats.[12]
- Plant-based diet
The plant-based diet is largely based on consumption of beans, grains, fruits, and vegetables and removal of meat, fish, and occasionally dairy and egg products from intake.[47] In other words, fiber and unsaturated fat intake is increased and consumption of higher calorie meats and saturated fats is decreased.[47] This diet has been shown to reduce BMI and introduce positive body composition changes when compared to a carnivore diet.[48]
- Intermittent fasting
Intermittent fasting (IF) involves consistent fasting blocks of time where fewer or no calories are consumed.[12] Intermittent fasting has been shown to improve fasting blood glucose levels and insulin resistance with a concurrent reduction in BMI.[49]
Strategies

Modifying plate size
Some studies have suggested that using smaller plates might help people to consume smaller portion sizes. [50]
Modifying portion sizes may impact energy intake.[51] Those who are presented with larger portion sizes do not report to have high levels of satiety. [51] In other words, hunger and satiety signals could be ignored with large portion sizes. [51] In a study focused on portion sizes, participants consumed 31% less calories with the small portion sized of a 6-inch submarine sandwich compared with the large portion size of a 12-inch submarine sandwich.[51] Increased portions have occurred simultaneously with the increase in obesity rates. Large portion sizes could be one of the factors contributing to the current increase in average body weight in the US.[51] Evidence from a systematic review of 72 randomized controlled trials indicates that people consistently eat more food when offered larger portion, package, or tableware sizes as opposed to smaller size alternatives.[52]
Choosing low-calorie foods
The majority of guidelines agree that a calorie deficit, particularly 500-750 kcal daily, can be recommended to those who want to lose weight.[5][12] A moderate decrease in caloric intake will lead to a slow weight loss, which is often more beneficial than a rapid weight loss for long term weight management.[8] For example, low fat meats reduce the total amount of calories and cholesterol consumed.[53]
Increasing protein intake
A high protein diet relative to a low-fat or high-carbohydrate diet may increase thermogenesis and decrease appetite leading to weight reduction,[54] particularly 3-6 months into a diet when rapid weight loss is observed.[55] However, these advantages may be reduced later at 12–24 months into a diet during the slow weight loss phase.[55]
Eating more soup
Studies have demonstrated that when compared to solid foods, soup ingestion decreases the amount of energy intake and increases feelings of satiety.[56] When soup is consumed before a meal, there is a 20% decrease in the number of calories consumed during said meal.[57]
Eating more dairy

Studies have shown that a diet high in dairy decreases total body fat.[58] This occurs because a high amount of dietary calcium increases the amount of energy and fat excreted from the body.[59] Other studies have noted that dairy sources of calcium lead to greater weight loss than supplemental calcium intake.[60] This could be due to the bioactive components of dairy sources, especially when combined with a lower calorie diet.[61] Since most natural dairy products contain fat content, there is a common understanding that this may cause weight gain.[60] However, dairy contains ingredients such as whey protein and certain combinations of protein/calcium nutrients that induce a positive effect on satiety, increase energy loss, and assists weight loss.[62]
Eating more vegetables
Fruits and vegetables have been shown to increase satiety and decrease hunger signals.[63] These food groups have a low energy density, mainly due to the high water content and partly due to the fiber content.[63] The reduction of energy density has been shown to enhance satiety.[63] The water content adds satisfying weight without excess calories and fiber slows gastric emptying.[63] Studies have also shown that fiber decreases hunger and also decreases total energy intake.[63]
Increasing fiber intake
Fruits and vegetables are two sources of fiber as discussed above. Dietary fiber has been suggested to aid weight management by inducing satiety,[5] decreasing absorption of macronutrients and promoting secretion of gut hormones.[64] Dietary fiber consists of non-digestible carbohydrates and lignin, which are a structural component in plants.[65]

Due to the high volume or water content of fiber-rich foods, fiber displaces available calories and nutrients from the diet.[66] Consumption of viscous fibers delays gastric emptying, which may cause an extended feeling of fullness.[67] Satiety is also induced by increasing chewing, which limits food intake by promoting the secretion of saliva and gastric juice, resulting in an expansion of the stomach.[68] In addition, hormone secretion is affected during fiber ingestion.[69] Insulin response is reduced and cholecystokinin (CCK) in the small intestine is increased.[64] Insulin regulates blood glucose levels while CCK adjusts gastric emptying, pancreatic secretion, and gall bladder contraction.[64] There is a direct correlation between CCK and satiety after foods of different fiber contents are consumed.[70]
In general, large intakes of dietary fiber at breakfast have been associated with less food intake at lunchtime.[71] Fiber may have the added benefit of helping consumers reduce food intake throughout the day, but results of studies examining this possibility have been conflicting.[70]
Increasing resistant starch intake
Resistant starch is a type of non-digestible, fermentable fiber resistant to amylase digestion in the small intestine.[72] It is broken down to short-chain fatty acids by microflora in the large intestine.[72] It is commonly found in cooked and cooled potatoes, green bananas, beans and legumes.[72] The short chain fatty acids can lead to further oxidation of fat and a higher energy expenditure.[73] Resistant starch dilutes energy density of food intake, maintains a bulking effect similar to non-fermentable fiber, and increases the expression of gut hormones PYY and GLP-1.[72][74][75][76] The increase in gut hormone expression affects neuronal pathways in the brain that contribute to long-term energy balance[77][78] and improved overall health of the intestines.[79]
Increasing caffeine intake
Caffeine and black coffee have been associated with increased energy expenditure and subsequent weight loss.[80] Caffeine belongs to a class of compounds called methylxanthines and is present in coffee, tea, cocoa, chocolate and some cola drinks.[81] Caffeine induces a thermogenic effect in the body by increasing sympathetic nervous system activity, which is an important regulator of energy expenditure.[82][83][84]
Increasing green tea intake
Catechins are polyphenols that are a major component of green tea extract.[85] Green tea has been associated with decreasing blood glucose,[86] inhibiting hepatic and body fat accumulation,[86][87] and stimulating thermogenesis[88] due to the catechins present in formulations. Moreover, catechins in the brain play a major role in satiety.[89] Independent of the caffeine content, green tea has also been shown to increase energy expenditure and fat oxidation in humans.[88][90]
While green tea intake alone may not significantly reduce weight or BMI, combining intake with other strategies aimed at weight loss could be helpful for both loss and weight maintenance. [91]
References
- "Healthy Weight". Centers for Disease Control and Prevention. 2022-06-03. Retrieved 2023-01-17.
- "Understanding Adult Overweight & Obesity | NIDDK". National Institute of Diabetes and Digestive and Kidney Diseases. Retrieved 2023-01-17.
- Seagle HM, Strain GW, Makris A, Reeves RS (February 2009). "Position of the American Dietetic Association: weight management". Journal of the American Dietetic Association. 109 (2): 330–346. doi:10.1016/j.jada.2008.11.041. PMID 19244669.
- Ryan DH, Kahan S (January 2018). "Guideline Recommendations for Obesity Management". The Medical Clinics of North America. Obesity Medicine. 102 (1): 49–63. doi:10.1016/j.mcna.2017.08.006. PMID 29156187.
- Goldman L, Schafer AI (2020). Goldman-Cecil Medicine (26th ed.). Philadelphia, PA: Elsevier. pp. 1418–1427. ISBN 9780323532662.
- Tylka TL, Annunziato RA, Burgard D, Daníelsdóttir S, Shuman E, Davis C, Calogero RM (2014). "The weight-inclusive versus weight-normative approach to health: evaluating the evidence for prioritizing well-being over weight loss". Journal of Obesity. 2014: 983495. doi:10.1155/2014/983495. PMC 4132299. PMID 25147734.
- Bacon L, Aphramor L (January 2011). "Weight science: evaluating the evidence for a paradigm shift". Nutrition Journal. 10: 9. doi:10.1186/1475-2891-10-9. PMC 3041737. PMID 21261939.
- Klein S, Sheard NF, Pi-Sunyer X, Daly A, Wylie-Rosett J, Kulkarni K, Clark NG (August 2004). "Weight management through lifestyle modification for the prevention and management of type 2 diabetes: rationale and strategies. A statement of the American Diabetes Association, the North American Association for the Study of Obesity, and the American Society for Clinical Nutrition". The American Journal of Clinical Nutrition. 80 (2): 257–263. doi:10.1093/ajcn/80.2.257. PMID 15277143.
- "Maintain a Healthy Weight". National Heart, Lung, and Blood Institute (NHLBI). Retrieved 2018-11-28.
- Mendenhall E, Singer M (February 2019). "The global syndemic of obesity, undernutrition, and climate change". Lancet. 393 (10173): 741. doi:10.1016/S0140-6736(19)30310-1. PMID 30765124. S2CID 72333975.
- Katzmarzyk PT, Martin CK, Newton RL, Apolzan JW, Arnold CL, Davis TC, et al. (September 2020). "Weight Loss in Underserved Patients - A Cluster-Randomized Trial". The New England Journal of Medicine. 383 (10): 909–918. doi:10.1056/NEJMoa2007448. PMC 7493523. PMID 32877581.
- Kim JY (March 2021). "Optimal Diet Strategies for Weight Loss and Weight Loss Maintenance". Journal of Obesity & Metabolic Syndrome. 30 (1): 20–31. doi:10.7570/jomes20065. PMC 8017325. PMID 33107442.
- "Obesity in adults: Dietary therapy". 10 May 2022.
- Flore G, Preti A, Carta MG, Deledda A, Fosci M, Nardi AE, et al. (March 2022). "Weight Maintenance after Dietary Weight Loss: Systematic Review and Meta-Analysis on the Effectiveness of Behavioural Intensive Intervention". Nutrients. 14 (6): 1259. doi:10.3390/nu14061259. PMC 8953094. PMID 35334917.
- Madigan CD, Graham HE, Sturgiss E, Kettle VE, Gokal K, Biddle G, et al. (May 2022). "Effectiveness of weight management interventions for adults delivered in primary care: systematic review and meta-analysis of randomised controlled trials". BMJ. 377: e069719. doi:10.1136/bmj-2021-069719. PMC 9150078. PMID 35636762.
- Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, Braunwald E (2022). Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine (12th ed.). Philadelphia, PA: Elsevier. pp. 442–470. ISBN 9780323824675. OCLC 1286711171.
- Feldman M, Friedman LS, Brandt LJ (2020). Sleisenger and Fordtran's Gastrointestinal and Liver Disease (11th ed.). Philadelphia, PA: Elsevier. pp. 92–100. ISBN 978-0-323-71094-7. OCLC 1159444603.
- Kellerman RD, Bope ET (2018). Conn's Current Therapy 2018. Philadelphia, PA: Elsevier, Inc. pp. 336–345. ISBN 978-0-323-52769-9.
- Rakel RE, Rakel DP (2016). Textbook of Family Medicine (Ninth ed.). Philadelphia, PA: Elsevier, Inc. pp. 891–911. ISBN 978-0-323-23990-5.
- The SuRF Report 2 (PDF). The Surveillance of Risk Factors Report Series (SuRF). World Health Organization. 2005. p. 22.
- Salari N, Jafari S, Darvishi N, Valipour E, Mohammadi M, Mansouri K, Shohaimi S (October 2021). "The best drug supplement for obesity treatment: a systematic review and network meta-analysis". Diabetology & Metabolic Syndrome. 13 (1): 110. doi:10.1186/s13098-021-00733-5. PMC 8522222. PMID 34663429.
- Bays HE, Fitch A, Christensen S, Burridge K, Tondt J (2022-06-01). "Anti-Obesity Medications and Investigational Agents: An Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022". Obesity Pillars. 2: 100018. doi:10.1016/j.obpill.2022.100018. ISSN 2667-3681. S2CID 248205315.
- Wing EJ, Schiffman FJ, Cecil RL (2022). Cecil Essentials of Medicine (10th ed.). Philadelphia, PA. pp. 626–634. ISBN 978-0-323-72272-8. OCLC 1252630759.
{{cite book}}: CS1 maint: location missing publisher (link) - Khaodhiar L, McCowen KC, Blackburn GL. Obesity and its comorbid conditions. Clin Cornerstone. 1999;2(3):17-31. doi: 10.1016/s1098-3597(99)90002-9. PMID 10696282.
- Barber TM, Hanson P, Weickert MO, Franks S. Obesity and Polycystic Ovary Syndrome: Implications for Pathogenesis and Novel Management Strategies. Clin Med Insights Reprod Health. 2019 Sep 9;13:1179558119874042. doi: 10.1177/1179558119874042. PMID 31523137; PMCID: PMC6734597.
- Lim SS, Hutchison SK, Van Ryswyk E, Norman RJ, Teede HJ, Moran LJ, et al. (Cochrane Gynaecology and Fertility Group) (March 2019). "Lifestyle changes in women with polycystic ovary syndrome". The Cochrane Database of Systematic Reviews. 2019 (3): CD007506. doi:10.1002/14651858.CD007506.pub4. PMC 6438659. PMID 30921477.
- Al-Goblan AS, Al-Alfi MA, Khan MZ (2014). "Mechanism linking diabetes mellitus and obesity". Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy. 7: 587–591. doi:10.2147/DMSO.S67400. PMC 4259868. PMID 25506234.
- Crandall JP, Shamoon H (2020). Goldman-Cecil Medicine (26th ed.). Philadelphia, PA. pp. 1490–1510. ISBN 978-0-323-53266-2. OCLC 1118693594.
{{cite book}}: CS1 maint: location missing publisher (link) - Strychar I (January 2006). "Diet in the management of weight loss". CMAJ. 174 (1): 56–63. doi:10.1503/cmaj.045037. PMC 1319349. PMID 16389240.
- Thom G, Lean M (May 2017). "Is There an Optimal Diet for Weight Management and Metabolic Health?" (PDF). Gastroenterology (Review). 152 (7): 1739–1751. doi:10.1053/j.gastro.2017.01.056. PMID 28214525.
- Guth E (September 2014). "JAMA patient page. Healthy weight loss". JAMA. 312 (9): 974. doi:10.1001/jama.2014.10929. PMID 25182116.
- Sacks FM, Bray GA, Carey VJ, Smith SR, Ryan DH, Anton SD, et al. (February 2009). "Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates". The New England Journal of Medicine. 360 (9): 859–873. doi:10.1056/NEJMoa0804748. PMC 2763382. PMID 19246357.
- Wadden TA, Webb VL, Moran CH, Bailer BA (March 2012). "Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy". Circulation (Narrative review). 125 (9): 1157–1170. doi:10.1161/CIRCULATIONAHA.111.039453. PMC 3313649. PMID 22392863.
- Mancini JG, Filion KB, Atallah R, Eisenberg MJ (April 2016). "Systematic Review of the Mediterranean Diet for Long-Term Weight Loss". The American Journal of Medicine. 129 (4): 407–415.e4. doi:10.1016/j.amjmed.2015.11.028. PMID 26721635.
- Ge L, Sadeghirad B, Ball GD, da Costa BR, Hitchcock CL, Svendrovski A, et al. (April 2020). "Comparison of dietary macronutrient patterns of 14 popular named dietary programmes for weight and cardiovascular risk factor reduction in adults: systematic review and network meta-analysis of randomised trials". BMJ. 369: m696. doi:10.1136/bmj.m696. PMC 7190064. PMID 32238384.
- Chawla S, Tessarolo Silva F, Amaral Medeiros S, Mekary RA, Radenkovic D (December 2020). "The Effect of Low-Fat and Low-Carbohydrate Diets on Weight Loss and Lipid Levels: A Systematic Review and Meta-Analysis". Nutrients. 12 (12): 3774. doi:10.3390/nu12123774. PMC 7763365. PMID 33317019.
- Anderson JW, Konz EC, Frederich RC, Wood CL (November 2001). "Long-term weight-loss maintenance: a meta-analysis of US studies". The American Journal of Clinical Nutrition. 74 (5): 579–584. doi:10.1093/ajcn/74.5.579. PMID 11684524.
- Svetkey LP, Simons-Morton D, Vollmer WM, Appel LJ, Conlin PR, Ryan DH, et al. (February 1999). "Effects of dietary patterns on blood pressure: subgroup analysis of the Dietary Approaches to Stop Hypertension (DASH) randomized clinical trial". Archives of Internal Medicine. 159 (3): 285–293. doi:10.1001/archinte.159.3.285. PMID 9989541.
- Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, et al. (April 1997). "A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group". The New England Journal of Medicine. 336 (16): 1117–1124. doi:10.1056/NEJM199704173361601. PMID 9099655. S2CID 15227903.
- Appel LJ, Champagne CM, Harsha DW, Cooper LS, Obarzanek E, Elmer PJ, et al. (2003-04-23). "Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial". JAMA. 289 (16): 2083–2093. doi:10.1001/jama.289.16.2083. PMID 12709466. S2CID 38404996.
- Siervo M, Lara J, Chowdhury S, Ashor A, Oggioni C, Mathers JC (January 2015). "Effects of the Dietary Approach to Stop Hypertension (DASH) diet on cardiovascular risk factors: a systematic review and meta-analysis". The British Journal of Nutrition. 113 (1): 1–15. doi:10.1017/S0007114514003341. PMID 25430608.
- Craddick SR, Elmer PJ, Obarzanek E, Vollmer WM, Svetkey LP, Swain MC (November 2003). "The DASH diet and blood pressure". Current Atherosclerosis Reports. 5 (6): 484–491. doi:10.1007/s11883-003-0039-5. PMID 14525682. S2CID 27229087.
- Steinberg D, Bennett GG, Svetkey L (April 2017). "The DASH Diet, 20 Years Later". JAMA. 317 (15): 1529–1530. doi:10.1001/jama.2017.1628. PMC 5509411. PMID 28278326.
- CDC (2022-12-06). "Healthy Eating for People With Diabetes". Centers for Disease Control and Prevention. Retrieved 2023-01-17.
- Sánchez-Sánchez ML, García-Vigara A, Hidalgo-Mora JJ, García-Pérez MÁ, Tarín J, Cano A (June 2020). "Mediterranean diet and health: A systematic review of epidemiological studies and intervention trials". Maturitas. 136: 25–37. doi:10.1016/j.maturitas.2020.03.008. PMID 32386663. S2CID 216280612.
- Paoli A, Rubini A, Volek JS, Grimaldi KA (August 2013). "Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets". European Journal of Clinical Nutrition. 67 (8): 789–796. doi:10.1038/ejcn.2013.116. PMC 3826507. PMID 23801097.
- Tran E, Dale HF, Jensen C, Lied GA (2020-09-30). "Effects of Plant-Based Diets on Weight Status: A Systematic Review". Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy. 13: 3433–3448. doi:10.2147/DMSO.S272802. PMC 7533223. PMID 33061504.
- Tran E, Dale HF, Jensen C, Lied GA (2020-09-30). "Effects of Plant-Based Diets on Weight Status: A Systematic Review". Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy. 13: 3433–3448. doi:10.2147/DMSO.S272802. PMC 7533223. PMID 33061504.
- Cho Y, Hong N, Kim KW, Cho SJ, Lee M, Lee YH, et al. (October 2019). "The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis". Journal of Clinical Medicine. 8 (10): 1645. doi:10.3390/jcm8101645. PMC 6832593. PMID 31601019.
- Rolls BJ, Morris EL, Roe LS (December 2002). "Portion size of food affects energy intake in normal-weight and overweight men and women". The American Journal of Clinical Nutrition. 76 (6): 1207–13. doi:10.1093/ajcn/76.6.1207. PMID 12450884.
- Ello-Martin JA, Ledikwe JH, Rolls BJ (July 2005). "The influence of food portion size and energy density on energy intake: implications for weight management". The American Journal of Clinical Nutrition. 82 (1 Suppl): 236S–241S. doi:10.1093/ajcn/82.1.236S. PMID 16002828.
- Hollands GJ, Shemilt I, Marteau TM, Jebb SA, Lewis HB, Wei Y, et al. (September 2015). "Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco". Cochrane Public Health Group. The Cochrane Database of Systematic Reviews. 2018 (9): CD011045. doi:10.1002/14651858.CD011045.pub2. PMC 4579823. PMID 26368271.

- Chizzolini R, Zanardi E, Dorigoni V, Ghidini S (April 1999). "Calorific value and cholesterol content of normal and low-fat meat and meat products". Trends in Food Science & Technology. 10 (4–5): 119–128. doi:10.1016/S0924-2244(99)00034-5.
- Paddon-Jones D, Westman E, Mattes RD, Wolfe RR, Astrup A, Westerterp-Plantenga M (May 2008). "Protein, weight management, and satiety". The American Journal of Clinical Nutrition. 87 (5): 1558S–1561S. doi:10.1093/ajcn/87.5.1558S. PMID 18469287.
- Magkos F (September 2020). "The role of dietary protein in obesity". Reviews in Endocrine & Metabolic Disorders. 21 (3): 329–340. doi:10.1007/s11154-020-09576-3. PMID 32740867. S2CID 220888114.
- Mattes R (January 2005). "Soup and satiety". Physiology & Behavior. 83 (5): 739–47. doi:10.1016/j.physbeh.2004.09.021. PMID 15639159. S2CID 2637690.
- Flood JE, Rolls BJ (November 2007). "Soup preloads in a variety of forms reduce meal energy intake". Appetite. 49 (3): 626–34. doi:10.1016/j.appet.2007.04.002. PMC 2128765. PMID 17574705.
- Zemel MB, Richards J, Milstead A, Campbell P (July 2005). "Effects of calcium and dairy on body composition and weight loss in African-American adults". Obesity Research. 13 (7): 1218–1225. doi:10.1038/oby.2005.144. PMID 16076991.
- Jacobsen R, Lorenzen JK, Toubro S, Krog-Mikkelsen I, Astrup A (March 2005). "Effect of short-term high dietary calcium intake on 24-h energy expenditure, fat oxidation, and fecal fat excretion". International Journal of Obesity. 29 (3): 292–301. doi:10.1038/sj.ijo.0802785. PMID 15672116. S2CID 19841675.
- Zemel MB, Thompson W, Milstead A, Morris K, Campbell P (April 2004). "Calcium and dairy acceleration of weight and fat loss during energy restriction in obese adults". Obesity Research. 12 (4): 582–590. doi:10.1038/oby.2004.67. PMID 15090625.
- Stonehouse W, Wycherley T, Luscombe-Marsh N, Taylor P, Brinkworth G, Riley M (July 2016). "Dairy Intake Enhances Body Weight and Composition Changes during Energy Restriction in 18-50-Year-Old Adults-A Meta-Analysis of Randomized Controlled Trials". Nutrients. 8 (7): 394. doi:10.3390/nu8070394. PMC 4963870. PMID 27376321.
- Egger G, Egger S (November 2009). "Weight management - Facts and fallacies". Australian Family Physician. 38 (11): 921–923. PMID 19893844.
- Rolls BJ, Ello-Martin JA, Tohill BC (January 2004). "What can intervention studies tell us about the relationship between fruit and vegetable consumption and weight management?". Nutrition Reviews. 62 (1): 1–17. doi:10.1111/j.1753-4887.2004.tb00001.x. PMID 14995052.
- Slavin JL (March 2005). "Dietary fiber and body weight". Nutrition. Burbank, Los Angeles County, Calif. 21 (3): 411–8. doi:10.1016/j.nut.2004.08.018. PMID 15797686.
- Institute of Medicine of the National Academies (2001). Dietary reference intakes. Proposed definition of dietary fiber. Washington, DC: National Academies Press.
- Saris WH (May 2003). "Glycemic carbohydrate and body weight regulation" (PDF). Nutrition Reviews. 61 (5 Pt 2): S10–6. doi:10.1301/nr.2003.may.S10-S16. PMID 12828187. S2CID 43180717.
- Schneeman BO (November 2002). "Gastrointestinal physiology and functions". The British Journal of Nutrition. 88 (Suppl 2): S159–63. doi:10.1079/BJN2002681. PMID 12495458.
- Heaton KW (December 1973). "Food fibre as an obstacle to energy intake". Lancet. 2 (7843): 1418–21. doi:10.1016/s0140-6736(73)92806-7. PMID 4128728.
- Korner J, Leibel RL (September 2003). "To eat or not to eat - how the gut talks to the brain". The New England Journal of Medicine. 349 (10): 926–8. doi:10.1056/NEJMp038114. PMID 12954739.
- Holt SH, Brand-Miller JC, Stitt PA (July 2001). "The effects of equal-energy portions of different breads on blood glucose levels, feelings of fullness and subsequent food intake". Journal of the American Dietetic Association. 101 (7): 767–73. doi:10.1016/S0002-8223(01)00192-4. PMID 11478473.
- Levine AS, Tallman JR, Grace MK, Parker SA, Billington CJ, Levitt MD (December 1989). "Effect of breakfast cereals on short-term food intake". The American Journal of Clinical Nutrition. 50 (6): 1303–7. doi:10.1093/ajcn/50.6.1303. PMID 2556910.
- Nugent AP (March 2005). "Health properties of resistant starch". Nutrition Bulletin. 30 (1): 27–54. doi:10.1111/j.1467-3010.2005.00481.x.
- Canfora EE, Meex RC, Venema K, Blaak EE (May 2019). "Gut microbial metabolites in obesity, NAFLD and T2DM". Nature Reviews. Endocrinology. 15 (5): 261–273. doi:10.1038/s41574-019-0156-z. PMID 30670819. S2CID 58948657.
- Englyst HN, Kingman SM, Cummings JH (October 1992). "Classification and measurement of nutritionally important starch fractions". European Journal of Clinical Nutrition. 46 (Suppl 2): S33–50. PMID 1330528.
- Higgins JA (2004). "Resistant starch: metabolic effects and potential health benefits". Journal of AOAC International. 87 (3): 761–8. doi:10.1093/jaoac/87.3.761. PMID 15287677.
- Zhou J, Hegsted M, McCutcheon KL, Keenan MJ, Xi X, Raggio AM, Martin RJ (April 2006). "Peptide YY and proglucagon mRNA expression patterns and regulation in the gut". Obesity. Silver Spring, Md. 14 (4): 683–9. doi:10.1038/oby.2006.77. PMID 16741270. S2CID 20183780.
- Abbott CR, Monteiro M, Small CJ, Sajedi A, Smith KL, Parkinson JR, Ghatei MA, Bloom SR (May 2005). "The inhibitory effects of peripheral administration of peptide YY(3-36) and glucagon-like peptide-1 on food intake are attenuated by ablation of the vagal-brainstem-hypothalamic pathway". Brain Research. 1044 (1): 127–31. doi:10.1016/j.brainres.2005.03.011. PMID 15862798. S2CID 13546829.
- Badman MK, Flier JS (March 2005). "The gut and energy balance: visceral allies in the obesity wars". Science. 307 (5717): 1909–14. Bibcode:2005Sci...307.1909B. doi:10.1126/science.1109951. PMID 15790843. S2CID 7681272.
- Davie JR (July 2003). "Inhibition of histone deacetylase activity by butyrate". The Journal of Nutrition. 133 (7 Suppl): 2485S–2493S. doi:10.1093/jn/133.7.2485S. PMID 12840228.
- Acheson KJ, Zahorska-Markiewicz B, Pittet P, Anantharaman K, Jéquier E (May 1980). "Caffeine and coffee: their influence on metabolic rate and substrate utilization in normal weight and obese individuals". The American Journal of Clinical Nutrition. 33 (5): 989–97. doi:10.1093/ajcn/33.5.989. PMID 7369170.
- Westerterp-Plantenga M, Diepvens K, Joosen AM, Bérubé-Parent S, Tremblay A (August 2006). "Metabolic effects of spices, teas, and caffeine". Physiology & Behavior. 89 (1): 85–91. doi:10.1016/j.physbeh.2006.01.027. PMID 16580033. S2CID 16414937.
- Dulloo AG (August 2002). "Biomedicine. A sympathetic defense against obesity". Science. 297 (5582): 780–1. doi:10.1126/science.1074923. PMID 12161638. S2CID 71039869.
- Astrup A, Toubro S, Cannon S, Hein P, Breum L, Madsen J (May 1990). "Caffeine: a double-blind, placebo-controlled study of its thermogenic, metabolic, and cardiovascular effects in healthy volunteers". The American Journal of Clinical Nutrition. 51 (5): 759–67. doi:10.1093/ajcn/51.5.759. PMID 2333832.
- Astrup A, Toubro S (February 1993). "Thermogenic, metabolic, and cardiovascular responses to ephedrine and caffeine in man". International Journal of Obesity and Related Metabolic Disorders. 17 (Suppl 1): S41–3. PMID 8384179.
- Graham HN (May 1992). "Green tea composition, consumption, and polyphenol chemistry". Preventive Medicine. 21 (3): 334–50. doi:10.1016/0091-7435(92)90041-f. PMID 1614995.
- Matsumoto N, Ishigaki F, Ishigaki A, Iwashina H, Hara Y (April 1993). "Reduction of blood glucose levels by tea catechin". Bioscience, Biotechnology, and Biochemistry. 57 (4): 525–527. doi:10.1271/bbb.57.525.
- Ishigaki A, Tonooka F, Matsumoto N, Hara Y (August 1991). Suppression of the accumulation of body and liver fat by tea catechin. Organizing Committee of International Symposium on Tea Science. Shizuoka, Japan. pp. 309–313.
- Dulloo AG, Seydoux J, Girardier L, Chantre P, Vandermander J (February 2000). "Green tea and thermogenesis: interactions between catechin-polyphenols, caffeine and sympathetic activity". International Journal of Obesity and Related Metabolic Disorders. 24 (2): 252–8. doi:10.1038/sj.ijo.0801101. PMID 10702779. S2CID 6895328.
- Wellman PJ (October 2000). "Norepinephrine and the control of food intake". Nutrition (Burbank, Los Angeles County, Calif.). 16 (10): 837–42. doi:10.1016/s0899-9007(00)00415-9. PMID 11054588.
- Chantre P, Lairon D (January 2002). "Recent findings of green tea extract AR25 (Exolise) and its activity for the treatment of obesity". Phytomedicine. 9 (1): 3–8. doi:10.1078/0944-7113-00078. PMID 11924761.
- Jurgens TM, Whelan AM, Killian L, Doucette S, Kirk S, Foy E, et al. (Cochrane Metabolic and Endocrine Disorders Group) (December 2012). "Green tea for weight loss and weight maintenance in overweight or obese adults". The Cochrane Database of Systematic Reviews. 2012 (12): CD008650. doi:10.1002/14651858.CD008650.pub2. PMC 8406948. PMID 23235664.
Further reading
- Brownell KD (2004). The Learn Program for Weight Management: lifestyle, exercise, attitudes, relationships, nutrition (10th ed.). Dallas, Tex.: American Health Pub. Co. ISBN 978-1-878513-41-0.
- Dalton S (1997). Overweight and weight management: the health professional's guide to understanding and practice. Gaithersburg, Md.: Aspen Publishers. ISBN 978-0-8342-0636-6.
- Laliberte M, Taylor V, McCabe RE (2009). The cognitive behavioral workbook for weight management: a step-by-step program. Oakland, Calif.: New Harbinger Publications. ISBN 978-1-57224-625-6.
- Fulda J (2008). Half-Assed: A Weight-Loss Memoir. Berkeley, CA: Seal Press. ISBN 978-1-58005-278-8.
- Mann T (7 April 2015). Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet Again. HarperCollins. ISBN 978-0-06-232926-4.