Endometrioma
Endometrioma is the presence of tissue similar to, but distinct from, the endometrium in and sometimes on the ovary. It is the most common form of endometriosis.[1] Endometrioma is found in 17–44% patients with endometriosis.[2] More broadly, endometriosis is the presence of tissue similar to, but distinct from, endometrial tissue located outside the uterus. The presence of endometriosis can result in the formation of scar tissue, adhesions and an inflammatory reaction. It usually is a benign growth. An endometrioma is most often found in the ovary.[3] This ovarian endometriosis forms dark, fluid-filled cysts.[4] These fluid-filled sacs can vary greatly in size and are known as endometriomas, also called "chocolate cysts". The fluid inside the cysts is thick, dark, old blood, giving it a chocolate-like appearance. It can also develop in the cul-de-sac (the space behind the uterus), the surface of the uterus, and between the vagina and rectum.[5]
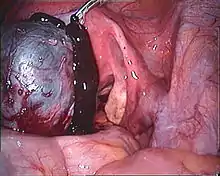
| Endometriosis of ovary | |
|---|---|
 | |
| Transvaginal ultrasonography showing a 67 x 40 mm endometrioma as distinguished from other types of ovarian cysts by a somewhat grainy and not completely anechoic content. | |
| Specialty | Gynecology |
Pathophysiology
Endometrial tissue is the mucous membrane that normally lines the uterus. The endometrium is richly supplied with blood and its growth is regulated by estrogen and progesterone.[6] It consists of glandular and stroma tissue from the lining of the uterus.[3] When the endometrial mucous membrane is found outside of the uterus in places such as the ovaries, it causes chronic pelvic pain with intercourse and menstrual cycles.
Endometriomas can produce a toxic environment by producing estrogen, cytokines, interleukins, and other inflammatory substances, that could damage healthy endometriomal tissue. This toxic fluid content can cause dire alterations to the normal surrounding endometriotic cells, potentially impacting the embryo, the ability of an embryo to implant successfully, and the responsiveness of the endometrium.[7] Endometrioma can potentially lead to premature ovarian failure, decreased ovarian function, or problems with ovulation.[4] Studies have also found that endometriomas occur two times more frequently in the left ovary (67%) than in the right one (33%), possibly due to the presence of the sigmoid colon on the left side.[2][8]
Risks
Endometriomas can increase the risk of ovarian cancer in reproductive women, decrease normal ovarian function, and cause pain in the pelvis during or after periods or during sexual intercourse. Although most endometriomas are found to be benign, the possibility of malignant tumors still exists, and surgery is needed to confirm malignancy and determine what future treatment must be administered.
Another factor that endometrioma can impact is the ovarian reserve, or the number of quality follicles left in the ovary to produce viable eggs.[9] Ovaries with endometriomas showed significantly less follicular density as compared to healthy ovaries, leading to a decrease in fertility.
Treatment
Medication
Nonsteroidal anti-inflammatory drugs (NSAIDs) are frequently used first in patients with pelvic pain, particularly if the diagnosis of endometriosis has not been definitively (excision and biopsy) established. The goal of directed medical treatment is to achieve an anovulatory state. Typically, this is achieved initially using hormonal contraception. This can also be accomplished with progestational agents (i.e., medroxyprogesterone acetate), danazol, gestrinone, or gonadotropin-releasing hormone agonists (GnRH), as well as other less well-known agents. These agents are generally used if oral contraceptives and NSAIDs are ineffective. GnRH can be combined with estrogen and progestogen (add-back therapy) without loss of efficacy but with fewer hypoestrogenic symptoms. These medications are often ineffective in treating endometriomas and any relief is short lived while taking the medications. Therapy with these agents has a large number of sometimes permanent side effects, such as hot flushes, loss of bone mass, deepening of voice, weight gain, and facial hair growth.[10]
Surgery
Laparoscopic surgical approaches include excision of ovarian adhesions and of endometriomas. Endometriomas require surgical removal and excision is considered to be superior to cyst vaporization or coagulation in terms of permanent removal of the disease and pain relief.[11] Surgery can sometimes have the effect of improving fertility but can have the adverse effect of leading to increases in cycle day 2 or 3 FSH for many patients. It can also pose the risk of diminishing the ovarian reserve, which could lead to post-surgery infertility. The removal of healthy ovarian tissue or compromising blood flow to the ovary are both risk factors of the surgery that could lead to detrimental affects on the ovarian reserve. However, despite the fact that there is a risk of loss of ovarian function, studies have shown the recurrence rate of endometrioma is reduced.[9]
Recurrence rate after the surgery varies from 5 to 20%.[12]
References
- Kaponis, Apostolos; Taniguchi, Fuminori; Azuma, Yukihiro; Deura, Imari; Vitsas, Charalampos; Decavalas, George O.; Harada, Tasuku (March 2015). "Current treatment of endometrioma". Obstetrical & Gynecological Survey. 70 (3): 183–195. doi:10.1097/OGX.0000000000000157. ISSN 1533-9866. PMID 25769433. S2CID 22099824.
- Gałczyński, Krzysztof; Jóźwik, Maciej; Lewkowicz, Dorota; Semczuk-Sikora, Anna; Semczuk, Andrzej (2019-11-07). "Ovarian endometrioma – a possible finding in adolescent girls and young women: a mini-review". Journal of Ovarian Research. 12 (1): 104. doi:10.1186/s13048-019-0582-5. ISSN 1757-2215. PMC 6839067. PMID 31699129.
- Bulletti, Carlo; Coccia, Maria Elisabetta; Battistoni, Silvia; Borini, Andrea (2010-08-01). "Endometriosis and infertility (a review)". Journal of Assisted Reproduction and Genetics. 27 (8): 441–447. doi:10.1007/s10815-010-9436-1. ISSN 1058-0468. PMC 2941592. PMID 20574791.
- "Endometriomas - Deep Ovarian Endometriosis - Brigham and Women's Hospital". www.brighamandwomens.org. Retrieved 2020-04-29.
- Venes, p. 808.
- Venes, p. 810.
- "Kristin Patzkowsky, MD - Endometriomas and fertility". Endometriosis : Causes - Symptoms - Diagnosis - and Treatment. 2016-10-24. Retrieved 2020-04-29.
- Sznurkowski, Jacek J.; Emerich, Janosz (2008). "Endometriomas are more frequent on the left side". Acta Obstetricia et Gynecologica Scandinavica. 87 (1): 104–106. doi:10.1080/00016340701671929. ISSN 1600-0412. PMID 17943469. S2CID 23135054.
- Kitajima, Michio; Khan, K. N.; Harada, A.; Taniguchi, K.; Inoue, T.; Kaneuchi, M.; Miura, K.; Masuzaki, H. (December 31, 2017). "Association between ovarian endometrioma and ovarian reserve". Frontiers in Bioscience. Frontiers In Bioscience, Elite ed., vol. 10. 10 (1): 92–102. doi:10.2741/e810. PMID 28930606. Retrieved 2020-04-29.
- "What are the treatments for endometriosis?". Retrieved 2018-11-08.
- Vercellini, Paolo; Viganò, Paola; Somigliana, Edgardo; Fedele, Luigi (2013-12-24). "Endometriosis: pathogenesis and treatment". Nature Reviews. Endocrinology. Springer Science and Business Media LLC. 10 (5): 261–275. doi:10.1038/nrendo.2013.255. ISSN 1759-5029. PMID 24366116. S2CID 13050344.
- Koninckx, Philippe R.; Ussia, Anastasia; Keckstein, Jorg; Adamyan, Leila V.; Zupi, Errico; Wattiez, Arnaud; Gomel, Victor (2018). "Evidence-Based Medicine: Pandora's Box of Medical and Surgical Treatment of Endometriosis". Journal of Minimally Invasive Gynecology. Elsevier BV. 25 (3): 360–365. doi:10.1016/j.jmig.2017.11.012. ISSN 1553-4650. PMID 29180308.
Bibliography
- Taber's cyclopedic medical dictionary. Venes, Donald, 1952-, Taber, Clarence Wilbur, 1870-1968. (Ed. 22, illustrated in full color ed.). Philadelphia: F.A. Davis. 2013. ISBN 9780803629783. OCLC 808316462.
{{cite book}}: CS1 maint: others (link)