Genital leiomyoma
Genital leiomyomas (also known as "Dartoic leiomyomas") are leiomyomas that originate in the dartos muscles, or smooth muscles, of the genitalia, areola, and nipple.[1] They are a subtype of cutaneous leiomyomas that affect smooth muscle found in the scrotum, labia, or nipple. They are benign tumors, but may cause pain and discomfort to patients.[2] Signs and symptoms of Genital leiomyoma can be symptomatic or asymptomatic and is dependent on the type of leiomyoma. In most cases, pain in the affected area or region is most common. For vaginal leiomyoma, vaginal bleeding and pain may occur. Uterine leiomyoma may exhibit pain in the area as well as painful bowel movement and/or sexual intercourse. Nipple pain, enlargement, and tenderness can be a symptom of nipple-areolar leiomyomas. Genital leiomyomas can be caused by multiple factors, one can be genetic mutations that affect hormones such as estrogen and progesterone. Moreover, risk factors to the development of genital leiomyomas include age, race, and gender. Ultrasound and imaging procedures are used to diagnose genital leiomyomas, while surgically removing the tumor is the most common treatment of these diseases. Case studies for nipple areolar, scrotal, and uterine leiomyoma were used, since there were not enough secondary resources to provide more evidence.
Types of genital leiomyomas
Uterine
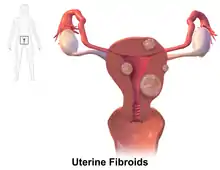
Uterine Leiomyomas are benign tumors that affect 70% of European people with uteri and more than 80% African descent people with uteri by the time they turn 50 years of age. Although, only 30% of people with uteri experience symptoms.[3] Of those with uterine leiomyomas, 29% result in hospitalizations.[4] One-third of patients with these fibroids experience life-threatening anemia, a condition where the body does not have enough oxygen due to lack of red blood cells to carry oxygen throughout the body.[5] These tumors are mainly treated by performing hysterectomies, a procedure in which the uterus is removed, and account for approximately 40-60% of all performed hysterectomies.[4][6] Symptoms are dependent on the location of the tumor, which may occur in the submucosal (under the mucous membranes and lines the inner part of some organs), intramural (within the walls of the organs), or subserosal areas (under the serosa and lines the outer part of some organs).
Nipple-areolar
Nipple-Areolar leiomyoma is a rare type of genital leiomyoma. It presents as either unilateral or bilateral growth of benign tumor of the smooth muscle that can be painful, tender, and inflamed.[7] They are typically less than 2 cm in length.[8] Since this is an extremely rare tumor, with only 50 cases reported in literature, it often only reported to physicians due to chronic nipple pain.[9]
Vaginal
Vaginal paraurethral leiomyoma is another type of genital leiomyoma that is also less common compared to other types of leiomyoma. It presents as a benign tumor of the smooth muscle in the genitourinary tract, which includes urinary and genital organs, that can grow rapidly during pregnancy. On the other hand, the tumor tend to decrease in size upon menopause. This may be due to the growth of tumor that is dependent on hormones. There is not a definite cause for the development of the disease, but one that was hypothesized is that it originates from a blood vessel tissue and smooth muscle fiber residue in an embryo. Imaging and histopathological examination is used for diagnosis of the disease. Furthermore, treatment of the disease is to surgically remove the tumor.[10]
Vulvar Leiomyomas are one the most prominent types of genital leiomyomas. Lesions to the vulva may be up to 15 cm in length and they are reported to be acutely painful. Enlargement of these leiomyomas may occur during pregnancy.[8]
Scrotal
Scrotal leiomyoma is considered to be an extremely rare type of genital leiomyoma. Because leiomyomas in the scrotum are usually painless and slowly grows over time, there is a delay in physician referral, with an average of 6–7 years. Physician referral usually occurs when people notice their testicles growing and getting heavier.[11] A review of 11,000 cases of benign and malignant tumors of the scrotum found 11 cases of scrotal leiomyoma. Scrotal leiomyomas can affect males of any age and race, but are more common in Caucasians from the ages of 40-60. The tumor in the scrotum has an average diameter of 6.4 cm.[12]
Signs and symptoms
People with leiomyoma can be presented as asymptomatic, or having no symptoms. However, some people may experience severe symptoms that can interfere with daily activities. Common symptoms are recurrent pain and pressure in the affected region.[13] People with uterine leiomyoma can experience pain during urination, bowel movements, and sexual intercourse. Other symptoms are abnormal vaginal bleeding and severe menstrual cramps.[14]
Nipple-Areolar leiomyomas can affect one or both nipples, presenting with symptoms of nipple tenderness.[7] People with leiomyomas in the scrotum generally notice a growing testicle over a span of multiple years, where it can grow and become heavy to the point of discomfort. Due to the painless and slow, progressive growth of the tumor, the time frame between recognizing the tumor and surgical removal can be anywhere from 2 to 20 years.[11]
Causes
Genetics
Development and progression of uterine leiomyomas may be contributed by changes in gene regulation or mutation of genes found to be associated with uterine fibroids. Abnormalities of these genes may initiate the formation or growth of these tumors.[15] Modification of signaling pathways and genes (e.g. CYP1A1, CYP1b1, and MED12) exhibits a correlation with the development and growth of tumors in the uterus.[6]
Hormones
The occurrence of uterine leiomyomas is mostly common during reproductive years. This suggests that the role of ovarian hormones, estrogen and progesterone, is important in the development of this disease. Studies have shown that the development of tumors rely on these hormones and that tumors have shown to affect estrogen metabolism as it can increase the amount both its estrogen and progesterone receptors.[16]
Diet and nutrition
Long-term results suggests that diets that are mostly plant-based, composed of fruits and vegetables, and rich in Vitamin D have a positive effect on the development of diseases, including uterine leiomyomas. On the other hand, alcohol, coffee, and red meat may have an effect on the progression or growth of these diseases based on observational and epidemiological studies.[17]
Risk Factors
Race
At the age of 35, incidence is reported to be 60% in African-American with-uterus persons and 40% in Caucasian with-uterus persons. By the age of 50, the incidence of uterine fibroids was >80% in African-American with uterus persons and >70% of Caucasian with uterus persons.[18]
Recurrence of uterine leiomyomas 4–5 years after removal occurs up to 59% of the time for with-uterus persons of African origin.[19]
Age
People with uteri who delay their first pregnancy past the age of 30 are at a higher risk for uterine fibroids.[20]
Genetic factors
Specific genetic alterations may play a role in the development of uterine leiomyomas. A mutation of a single mesenchymal cell, a stem cell that plays an important role in making and repairing bone, and fat - found in the bone marrow and adipose tissues, with the involvement of progesterone and 17 b-estrodiol can lead to these fibroids.[21]
Early menarche
Some early studies report early age onset of menstruation increases the risk of developing fibroids. However, the biological mechanism of how this occurs is not well understood and further investigation is needed.[22]
Age
The occurrence of benign tumors of the nipple commonly starts at the age of 20 and peaks around the age of 40 to 50. Growth of nipple-areolar leiomyomas may increase even after menopause.[23]
Diagnosis
There are many ways genital leiomyomas can be diagnosed. Those who have genital leiomyomas can be asymptomatic or symptomatic. Symptoms including but not limited to pelvic pain or abnormal menstrual bleeding are used to assess fibroids. Imaging are often used to detect the presence of fibroids, particularly uterine fibroids. This includes ultrasonography, a procedure that uses high-frequency sound waves to capture tissue and organ images; Sonohysterography, a painless procedure similar to ultrasonography to capture images inside the uterus; Hysteroscopy, which examines the inside of the uterus and cervix using a flexible tube called hysteroscope. [24]
Treatment
Treatment for genital leiomyomas primarily consist of removal by surgeries.[25][26] However, genital leiomyomas typically re-occur and may reappear from 6 weeks to over 15 years post-removal.[8] When managing leiomyomas, radiation treatment should be avoided due to the inducing effect of malignant transformation in the smooth muscle of the tumor.[11]
For uterine leiomyomas, complete removal of the uterus is required.[27] There is minimal evidence to support the use of myomectomy to preserve fertility.[28] Evidence shows that preoperative use of gonadotropin-releasing hormone agonists, which prevents or lessen the production of hormones like progesterone, estrogen, and testosterone, can reduce surgical complications.[29]
Subareolar leiomyomas require surgical removals. Precise surgical margins are needed to prevent re-occurrences.[30]
Leiomyomas in the scrotum require an orchidectomy, or surgical removal of one or two testicles.
To manage pain that arises from the fibroids, drugs that affect smooth muscle contraction such as nitroglycerin, nifedipine, phenoxybenzamine and doxazosin can be employed to ease the pain. For nerve pain or tenderness, gabapentin and topical analgesics may be employed.[8]
Clinical cases
41-year-old-male
A 41-year-old-male presented with a yellow nodule in the upper left areola. He reported mild pain and itching, but denied other symptoms. Sebaceous glands, epidermal hyperplasia, and tumor nests were among the numerous findings that lead to preceded a diagnosis of diagnosis of areolar leiomyoma with sebaceous hyperplasia. Characteristics of the leiomyoma included positive for estrogen and progesterone receptors and high expression of epidermal growth factor, insulin-like growth factor 1, and fibroblast growth factor-2. It is suspected that these growth factors led to the growth of the leiomyoma through an autocrine process.. The patient declined resection and the region has remained stable since.[31]
67-year-old-female
A 67-year-old-female presented with a growing mass on the left breast areolar region. The patient had been taking methotrexate to treat her rheumatoid arthritis. Magnetic resonance imaging revealed led to a conclusion that the tumor arose from the areola. A biopsy led to a diagnosis of diffuse large, non GC B-cell lymphoma that was suspected to be associated with methotrexate. The tumor reduced in size following the withdrawal of methotrexate. Three months later, another tumor developed in the areolar region of the opposite breast.[32]
35-year-old-female
A 35-year-old-female presented with a painful lump in the right nipple. The patient reported the lump occurred after a breastfeeding injury 3 years prior to coming into the outpatient center. The tumor has been growing ever since. A biopsy was performed to confirm the leiomyoma in the nipple.[9]
48-year-old-female
A 48-year-old-female presented with several uterine fibroids that were asymptomatic. The tumor was removed vaginally which revealed to be a vaginal leiomyoma. Vaginal leiomyomas are rare and removal by vaginal route is the preferred treatment option.[33]
39-year-old-male
A 39-year-old-male presented with a dull aching pain in the right scrotum. The patient had a history of his right scrotum slowly growing for the past year. There were no other symptoms of urinary tract infections (UTIs), cough, fever, weight loss, or night sweats. Further examination and an ultrasound scan found a firm mass in the right scrotum with a size of 6 cm x 4 cm that was inseparable from the testis. The patient underwent a right radical orchiectomy, or a surgical operation to remove the one or more testicles, since malignancy of the tumor could not be determined. The patient recovered and was discharged home after the operation.[12]
71-year-old-male
A 71-year-old-male presented with a large and heavy left scrotum that has been growing for 10 years. Further examination confirmed a firm tumor in the left scrotum that was attached to the testis. The tumor was measured to be 11 cm in diameter. The patient underwent orchidectomy, or surgical removal of the testicle.[11]
See also
References
- Freedberg, et al. (2003). Fitzpatrick's Dermatology in General Medicine. (6th ed.). Page 1033. McGraw-Hill. ISBN 0-07-138076-0.
- Bernett CN, Mammino JJ (2022). "Cutaneous Leiomyomas". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 29489175. Retrieved 2022-07-31.
- Lewis TD, Malik M, Britten J, San Pablo AM, Catherino WH (2018). "A Comprehensive Review of the Pharmacologic Management of Uterine Leiomyoma". BioMed Research International. 2018: 2414609. doi:10.1155/2018/2414609. PMC 5893007. PMID 29780819.
- Merrill RM (January 2008). "Hysterectomy surveillance in the United States, 1997 through 2005". Medical Science Monitor. 14 (1): CR24–CR31. PMID 18160941.
- Bartels CB, Cayton KC, Chuong FS, Holthouser K, Arian SE, Abraham T, Segars JH (March 2016). "An Evidence-based Approach to the Medical Management of Fibroids: A Systematic Review". Clinical Obstetrics and Gynecology. 59 (1): 30–52. doi:10.1097/GRF.0000000000000171. PMID 26756261. S2CID 10329880.
- Mathew RP, Francis S, Jayaram V, Anvarsadath S (October 2021). "Uterine leiomyomas revisited with review of literature". Abdominal Radiology. 46 (10): 4908–4926. doi:10.1007/s00261-021-03126-4. PMID 34057564. S2CID 235250560.
- Chiorean A, Pintican RM, Szep M, Feier D, Rogojan L, Fetica B, et al. (August 2020). "Nipple Ultrasound: A Pictorial Essay". Korean Journal of Radiology. 21 (8): 955–966. doi:10.3348/kjr.2019.0831. PMC 7369201. PMID 32677380.
- Malik K, Patel P, Chen J, Khachemoune A (February 2015). "Leiomyoma cutis: a focused review on presentation, management, and association with malignancy". American Journal of Clinical Dermatology. 16 (1): 35–46. doi:10.1007/s40257-015-0112-1. PMID 25605645.
- Spyropoulou GA, Pavlidis L, Trakatelli M, Athanasiou E, Pazarli E, Sotiriadis D, Demiri E (January 2015). "Rare benign tumours of the nipple". Journal of the European Academy of Dermatology and Venereology. 29 (1): 7–13. doi:10.1111/jdv.12623. PMID 25124255. S2CID 25298700.
- Braga A, Soave I, Caccia G, Regusci L, Ruggeri G, Pitaku I, et al. (June 2021). "What is this vaginal bulge? An atypical case of vaginal paraurethral leiomyoma. A case report and literature systematic review". Journal of Gynecology Obstetrics and Human Reproduction. 50 (6): 101822. doi:10.1016/j.jogoh.2020.101822. PMID 32492525. S2CID 219315417.
- Ariafar A, Soltani M, Khajeh F, Zeighami S, Naghdi Sedeh N, Miladpour B (September 2020). "Scrotal leiomyoma a rare benign intra-scrotal mass could lead to unnecessary orchiectomy". Urology Case Reports. 32: 101170. doi:10.1016/j.eucr.2020.101170. PMC 7184519. PMID 32368497.
- Egharevba PA, Omoseebi O, Okunlola AI, Omisanjo OA (2020). "Scrotal leiomyoma: a rare cause of scrotal swelling". African Journal of Urology. 26 (1): 72. doi:10.1186/s12301-020-00082-1. ISSN 1961-9987.
- Florence AM, Fatehi M (2022). "Leiomyoma". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 30855861. Retrieved 25 July 2022.
- Costantini E, Cochetti G, Porena M (August 2008). "Vaginal para-urethral myxoid leiomyoma: case report and review of the literature". International Urogynecology Journal and Pelvic Floor Dysfunction. 19 (8): 1183–1185. doi:10.1007/s00192-008-0588-9. PMID 18351279. S2CID 40050485.
- Medikare V, Kandukuri LR, Ananthapur V, Deenadayal M, Nallari P (July 2011). "The genetic bases of uterine fibroids; a review". Journal of Reproduction & Infertility. 12 (3): 181–191. PMC 3719293. PMID 23926501.
- Cook JD, Walker CL (May 2004). "Treatment strategies for uterine leiomyoma: the role of hormonal modulation". Seminars in Reproductive Medicine (in German). 22 (2): 105–111. doi:10.1055/s-2004-828616. PMID 15164305.
- Afrin S, AlAshqar A, El Sabeh M, Miyashita-Ishiwata M, Reschke L, Brennan JT, et al. (May 2021). "Diet and Nutrition in Gynecological Disorders: A Focus on Clinical Studies". Nutrients. 13 (6): 1747. doi:10.3390/nu13061747. PMC 8224039. PMID 34063835.
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM (January 2003). "High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence". American Journal of Obstetrics and Gynecology. 188 (1): 100–107. doi:10.1067/mob.2003.99. PMID 12548202.
- Donnez J, Dolmans MM (November 2016). "Uterine fibroid management: from the present to the future". Human Reproduction Update. 22 (6): 665–686. doi:10.1093/humupd/dmw023. PMC 5853598. PMID 27466209.
- Petraglia F, Serour GI, Chapron C (December 2013). "The changing prevalence of infertility". International Journal of Gynaecology and Obstetrics. 123 Suppl 2 (Suppl 2): S4–S8. doi:10.1016/j.ijgo.2013.09.005. PMID 24112745. S2CID 45271567.
- Hattori T, Singh VK, McGeer EG, McGeer PL (January 1976). "Immunohistochemical localization of choline acetyltransferase containing neostriatal neurons and their relationship with dopaminergic synapses". Brain Research. 102 (1): 164–173. doi:10.1016/0006-8993(76)90583-7. PMID 2366. S2CID 1071780.
- Khan AT, Shehmar M, Gupta JK (2014). "Uterine fibroids: current perspectives". International Journal of Women's Health. 6: 95–114. doi:10.2147/IJWH.S51083. PMC 3914832. PMID 24511243.
- Spyropoulou GA, Pavlidis L, Trakatelli M, Athanasiou E, Pazarli E, Sotiriadis D, Demiri E (January 2015). "Rare benign tumours of the nipple". Journal of the European Academy of Dermatology and Venereology. 29 (1): 7–13. doi:10.1111/jdv.12623. PMID 25124255.
- De La Cruz MS, Buchanan EM (January 2017). "Uterine Fibroids: Diagnosis and Treatment". American Family Physician. 95 (2): 100–107. PMID 28084714.
- Rakotomahenina H, Rajaonarison J, Wong L, Brun JL (August 2017). "Myomectomy: technique and current indications". Minerva Ginecologica. 69 (4): 357–369. doi:10.23736/S0026-4784.17.04073-4. PMID 28447445.
- Sabry M, Al-Hendy A (April 2012). "Medical treatment of uterine leiomyoma". Reproductive Sciences. 19 (4): 339–353. doi:10.1177/1933719111432867. PMC 3343067. PMID 22378865.
- Juhasz-Böss I, Gabriel L, Bohle RM, Horn LC, Solomayer EF, Breitbach GP (2018). "Uterine Leiomyosarcoma". Oncology Research and Treatment. 41 (11): 680–686. doi:10.1159/000494299. PMID 30321869. S2CID 53114823.
- Metwally M, Raybould G, Cheong YC, Horne AW (January 2020). "Surgical treatment of fibroids for subfertility". The Cochrane Database of Systematic Reviews. 1 (1): CD003857. doi:10.1002/14651858.CD003857.pub4. PMC 6989141. PMID 31995657.
- Lethaby A, Puscasiu L, Vollenhoven B (November 2017). "Preoperative medical therapy before surgery for uterine fibroids". The Cochrane Database of Systematic Reviews. 11 (11): CD000547. doi:10.1002/14651858.CD000547.pub2. PMC 6486044. PMID 29139105.
- Salemis NS (November 2020). "Subareolar male genital leiomyoma: An exceedingly rare clinical entity". The Breast Journal. 26 (11): 2248–2249. doi:10.1111/tbj.14052. PMID 32935434. S2CID 221748592.
- Oya K, Nakamura Y, Fujisawa Y (2022). "Unilateral areolar leiomyoma with sebaceous hyperplasia". Indian Journal of Dermatology, Venereology and Leprology. 88 (4): 536–540. doi:10.25259/IJDVL_7_2020. PMID 35593282. S2CID 248713094.
- Matsubayashi RN, Iwasaki H, Iwakuma N, Momosaki S (2019). "Methotrexate (MTX)-associated malignant lymphoma of the bilateral breast: imaging features in comparison to other nipple-areolar tumors". Clinical Imaging. 53: 120–125. doi:10.1016/j.clinimag.2018.10.004. PMID 30340074. S2CID 53008893.
- Shah M, Saha R, Kc N (May 2021). "Vaginal Leiomyoma: A Case Report". Journal of Nepal Medical Association. 59 (237): 504–505. doi:10.31729/jnma.6180. PMC 8673445. PMID 34508428.