Ilizarov apparatus
The Ilizarov apparatus is a type of external fixation used in orthopedic surgery to lengthen or reshape limb bones; as a limb-sparing technique to treat complex and/or open bone fractures; and in cases of infected nonunions of bones that are not amenable with other techniques. It is named after the orthopedic surgeon Gavriil Abramovich Ilizarov from the Soviet Union, who pioneered the technique.
| Ilizarov apparatus | |
|---|---|
 | |
| ICD-9-CM | 78.3, 84.53 |
| MeSH | D018889 |
History

Ilizarov used external fixation devices on patients to treat non-unions in the 1950s.[1] Ilizarov observed the callus formation and discovered distraction osteogenesis when one patient lengthened his frame rather than compressing it.[1] The procedure, and the first apparatus he designed for it, was inspired by a shaft bow harness on a horse carriage (see photo to the right).[2] Originally bicycle parts were used for the frame.
The technique gained fame across the Soviet Union when he successfully treated Soviet world-record holder, and gold medalist high jumper, Valery Brumel in 1968.[1][2] Brumel broke his tibia in a motorcycle accident and had 20 unsuccessful operations over a three-year period to try to repair his non-union.[2] Ilizarov used distraction osteogenesis to heal the non-union and 3.5 cm (1.4 in) leg length discrepancy.[2]
Ilizarov gained more fame in 1980 when he successfully treated Italian journalist and adventurer, Carlo Mauri.[1][3] Mauri had broken his leg in a skiing accident ten years earlier and his tibia never properly healed.[1] When he was on an expedition across the Atlantic, the wound on his leg reopened and a Russian doctor advised him to see Ilizarov.[1][3] When Mauri returned to Italy after his treatment, Italian doctors were impressed that his tibial non-union was repaired.[1] They invited Ilizarov to speak at the Italian AO Conference in Bellagio.[1] This was the first time Ilizarov spoke outside of the "Iron Curtain".[3]
The technique was brought to the US in 1987 by Victor Frankel, president of Hospital for Joint Diseases,[3] and Dr. Stuart Green who, in 1992, edited the first English translation of Ilizarov's book.
The Ilizarov external fixators can be used to correct angular deformity in the leg, to correct leg-length differences, and treat non-unions.[1] In most developing countries it is a highly specialized technique used mainly for deformity correction by experienced surgeons due to its complexity. Further development of the ring construct led to the Taylor Spatial Frame which is more versatile and far easier to use, but very costly. Intramedullary limb lengthening devices are also available, but are also a very costly option.
Mechanics and physics
The device is a specialized form of external fixator, a circular fixator, modular in construction. Stainless steel (or titanium) rings are fixed to the bone via stainless heavy-gauge wire (called "pins" or Kirschner wires). The rings are connected to each other with threaded rods attached through adjustable nuts. The circular construction and tensioned wires of the Ilizarov apparatus provide far more structural support than the traditional monolateral fixator system. This allows early weightbearing.
The apparatus is based on the principle which Ilizarov called "the theory of tensions". Through controlled and mechanically applied tension stress, Ilizarov was able to show that the bone and soft tissue can be made to regenerate in a reliable and reproducible manner.[4] The top rings of the Ilizarov (fixed to the healthy bone by the tensioned wire) allow force to be transferred through the external frame (the vertical metal rods), bypassing the fracture site. Force is then transferred back to the healthy bone through the bottom ring and the tensioned wires. This allows the Ilizarov apparatus to act as a sort of bridge, both immobilizing the fracture site and relieving it of stress, while allowing for the movement of the entire limb and partial weight-bearing. Middle rings (and tensioned wires) act to hold the bone fragments in place and to give greater structural support to the apparatus and limb. However, the critical load bearing rings are the top and bottom rings which transfer the force from the healthy bone down to the healthy bone, bypassing the fracture site.
Bone lengthening and reshaping
In addition to being used to support a fractured limb, the Ilizarov frame is also commonly used to correct deformity through distraction osteogenesis.
The procedure consists of an initial surgery, during which the bone is surgically fractured and the ring apparatus is attached. As the patient recovers, the fractured bone begins to grow together. While the bone is growing, the frame is adjusted by means of turning the nuts, thus increasing the space between two rings. As the rings are connected to opposite sides of the fracture, this adjustment, done four times a day, moves the now-healing fracture apart by approximately one millimeter per day. The incremental daily increases result in a considerable lengthening of the limb over time. Once the lengthening phase is complete, the apparatus stays on the limb for a consolidation period. The patient is able to fully weight bear on the Ilizarov frame, using crutches initially and pain is lessened. Once healing is complete, a second surgery is necessary to remove the ring apparatus. The result is a limb that is significantly longer. Additional surgery may be necessary, in the case of leg lengthening, to lengthen the Achilles tendon to accommodate the longer bone length. The major advantage of this procedure is that because the apparatus provides complete support while the bone is recovering the patient can remain active aiding recovery.
A further use is in bone transport, whereby a defect in a long bone can be treated by transporting a segment of bone, whilst simultaneously lengthening regenerating bone to reduce the defect and finally dock with the other segment, producing a single bony unit.
While the Ilizarov apparatus is minimally invasive (no large incisions are made), it is not free of complications. Pain is common and can be severe, but is treatable with analgesics. Careful attention to cleaning and hygiene is necessary to prevent pin site infection. Other complications include swelling, muscle transfixion, and joint contractures. Physical therapy is often indicated.
Bone fracture treatment
The Ilizarov method is widely used to treat complex and/or open bone fractures. This method is preferred over conventional treatment options (such as internal fixator or cast) where there is a high risk of infection or the fracture is of such severity that internal fixators are unworkable. Journalist Ed Vulliamy wrote a detailed description from the patient's viewpoint of Ilizarov apparatus treatment of a bad fracture.[5]
Images
The following case study illustrates the Ilizarov apparatus treatment procedure for a fractured limb. The photographs are of the same patient during the course of treatment.
 X-ray of fracture and initial external fixator applied within 24 hours of patient's admission to hospital
X-ray of fracture and initial external fixator applied within 24 hours of patient's admission to hospital Front-left view of the Ilizarov apparatus treating a fractured tibia and fibula. The patient suffered an open fracture. It is located slightly above black metal ring. Photographs 1 through 4 are taken four weeks following the fracture and two weeks following the installation of the Ilizarov apparatus.
Front-left view of the Ilizarov apparatus treating a fractured tibia and fibula. The patient suffered an open fracture. It is located slightly above black metal ring. Photographs 1 through 4 are taken four weeks following the fracture and two weeks following the installation of the Ilizarov apparatus. Front (top) view with a view of the healthy leg. The patient is lying on his stomach.
Front (top) view with a view of the healthy leg. The patient is lying on his stomach. View of several pin sites (two weeks following surgery)
View of several pin sites (two weeks following surgery) X-ray of the fracture site immediately following the application of the Ilizarov method
X-ray of the fracture site immediately following the application of the Ilizarov method X-ray of the fracture site, part 1 (two months following fracture)
X-ray of the fracture site, part 1 (two months following fracture) X-ray of the fracture site, part 2 (two months following fracture)
X-ray of the fracture site, part 2 (two months following fracture) X-ray of the fracture site (three months following fracture). Note formation of bone callus around fracture site.
X-ray of the fracture site (three months following fracture). Note formation of bone callus around fracture site. X-ray of the fracture site, part 2 (three months following fracture). Note formation of bone callus around fracture site.
X-ray of the fracture site, part 2 (three months following fracture). Note formation of bone callus around fracture site.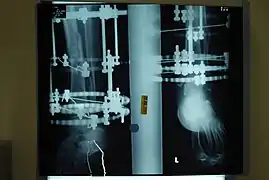 X-ray of the fracture site, part 2 (four months following fracture)
X-ray of the fracture site, part 2 (four months following fracture)
See also
- Bone healing
- Fibrocartilage callus
- Osteoporosis
- Stress fracture
- Blowout fracture
- Octopod External Fixator
- Pseudarthrosis
- List of Russian inventions
- Instruments used in general surgery
- Timeline of Russian inventions and technology records
- Fibular hemimelia
References
- Spiegelberg B, Parratt T, Dheerendra SK, Khan WS, Jennings R, Marsh DR. (2010). "Ilizarov principles of deformity correction". Annals of the Royal College of Surgeons of England. 92 (2): 101–5. doi:10.1308/003588410X12518836439326. PMC 3025247. PMID 20353638.
{{cite journal}}: CS1 maint: uses authors parameter (link) - Svetlana Ilizarov (2006). "The Ilizarov Method: History and Scope". In S. Robert Rozbruch; Svetlana Ilizarov (eds.). Limb Lengthening and Reconstruction Surgery. CRC Press. pp. 3–6. ISBN 0849340519.
- Svetlana Ilizarov (2006). "The Ilizarov Method: History and Scope". In S. Robert Rozbruch; Svetlana Ilizarov (eds.). Limb Lengthening and Reconstruction Surgery. CRC Press. pp. 15–16. ISBN 0849340519.
- Paley, Dror; Kovelman, Harry F; Herzenberg, John E (October 1993). "Ilizarov technology". In Stauffer, Richard (ed.). Advances in Operative Orthopaedics: Volume 1 (PDF). Mosby Inc. pp. 243–287. ISBN 978-0-8151-7939-9. Archived from the original (PDF) on 19 March 2012. Retrieved 14 January 2012.
- Ed Vulliamy (13 December 2015). "How Comrade Ilizarov saved my leg". The Observer. Retrieved 13 December 2015.
External links
- Living with an Ilizarov/Taylor Spatial Frame UK newspaper article
- ilizarov.com (English)
- The ILIZAROV frame wearer's support group
- More information and pictures about the Ilizarov surgical technique
- Institute for Limb Lengthening and Reconstruction
- Taylor Spatial Frame
- Legs lengthening and correction with Ilizarov frame
- Providing excellent case summaries for Ilizarov treatment of complex fractures, including X-rays