Perforated eardrum
A perforated eardrum (tympanic membrane perforation) is a hole in the eardrum. It can be caused by infection (otitis media), trauma, overpressure (loud noise), inappropriate ear clearing, and changes in middle ear pressure. An otoscope can be used to view the eardrum to diagnose a perforation. Perforations may heal naturally, or require surgery.
| Perforated eardrum | |
|---|---|
| Other names | Punctured eardrum |
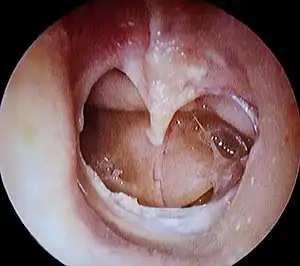 | |
| A completely perforated eardrum, showing the handle of the malleus (hammer bone). | |
| Specialty | ENT surgery |
| Symptoms | conductive hearing loss, tinnitus, ear pain, vertigo |
| Causes | ear infection, physical trauma, overpressure, ear cleaning |
| Diagnostic method | otoscopy |
| Treatment | conservative or surgery |
Presentation
A perforated eardrum leads to conductive hearing loss, which is usually temporary. Other symptoms may include tinnitus, ear pain, vertigo, or a discharge of mucus.[1] Nausea and/or vomiting secondary to vertigo may occur.[2]
Causes
A perforated eardrum can have one of many causes, such as:
- infection (otitis media).[3] This infection may then spread through the middle ear, and may reoccur.[3]
- trauma. This may be caused by trying to clean ear wax with sharp instruments. It may also occur due to surgical complications.[4]
- overpressure (loud noise or shockwave from an explosion).
- inappropriate ear clearing.
- flying with a severe cold, due to changes in air pressure and blocked Eustachian tubes resulting from the cold. This is especially true on landing.
Diagnosis
An otoscope can be used to look at the ear canal. This gives a view of the ear canal and eardrum, so that a perforated eardrum can be seen. Tympanometry may also be used.[5]
Treatment
Conservative management
A perforated eardrum often heals naturally.[2][6] It may heal in a few weeks, or may take up to a few months.[2]
Surgery
Some perforations require surgical intervention.[3] This may take the form of a paper patch to promote healing (a simple procedure by an ear, nose and throat specialist), or surgery (tympanoplasty).[2] However, in some cases, the perforation can last several years and will be unable to heal naturally. For patients with persistent perforation, surgery is usually undertaken to close the perforation. The objective of the surgery is to provide a platform of sort to support the regrowth and healing of the tympanic membrane in the two weeks post surgery period. There are two ways of doing the surgery:
- Traditional tympanoplasty, usually using the microscope and performed through a 10 cm incision behind the ear lobe. This technique was introduced by Wullstien and Zollner[7] and popularized by the Jim Sheehy at the House Ear Institute.[8]
- Endoscopic tympanoplasty, usually using the endoscope through the ear canal without the need for incision. This technique was introduced and popularized by Professor Tarabichi of TSESI: Tarabichi Stammberger Ear and Sinus Institute.[9]
The success of surgery is variable based on the cause of perforation and the technique being used. Predictors of success include traumatic perforation, dry ear, and central perforations. Predictors of failure includes young age and poor eustachian tube function.[8] The use of minimally invasive endoscopic technique does not reduce the chance of successful outcome.[9] Hearing is usually recovered fully, but chronic infection over a long period may lead to permanent hearing loss. Those with more severe ruptures may need to wear an ear plug to prevent water contact with the ear drum.
References
- "Perforated eardrum - Symptoms". National Health Service. Retrieved 17 August 2011.
- "Ruptured eardrum (perforated eardrum) - Symptoms and causes". Mayo Clinic.
- McGurk, Mark (2006). "12 - ENT Disorders". Essential Human Disease for Dentists. Churchill Livingstone. pp. 195–204. doi:10.1016/B978-0-443-10098-7.50015-4. ISBN 978-0-443-10098-7.
- McCain, Joseph P.; Kim, King (2012). "6 - Endoscopic Oral and Maxillofacial Surgery". Current Therapy In Oral and Maxillofacial Surgery. Saunders. pp. 31–62. doi:10.1016/B978-1-4160-2527-6.00006-2. ISBN 978-1-4160-2527-6.
- Hain, Timothy C. (2007-01-01), Goetz, Christopher G. (ed.), "Chapter 12 - Cranial Nerve VIII: Vestibulocochlear System", Textbook of Clinical Neurology (Third Edition), Philadelphia: W.B. Saunders, pp. 199–215, ISBN 978-1-4160-3618-0, retrieved 2021-11-12
- Martin, Lisa (2012). "43 - Chinchillas as Experimental Models". The Laboratory Rabbit, Guinea Pig, Hamster, and Other Rodents. Academic Press, American College of Laboratory Animal Medicine. pp. 1009–1028. doi:10.1016/B978-0-12-380920-9.00043-2. ISBN 978-0-12-380920-9.
- Zöllner, Fritz (October 1955). "The Principles of Plastic Surgery of the Sound-Conducting Apparatus". The Journal of Laryngology & Otology. 69 (10): 637–652. doi:10.1017/s0022215100051240. ISSN 0022-2151.
- Sheehy, J. L.; Glasscock, M. E. (1967-10-01). "Tympanic Membrane Grafting With Temporalis Fascia". Archives of Otolaryngology–Head & Neck Surgery. 86 (4): 391–402. doi:10.1001/archotol.1967.00760050393008. ISSN 0886-4470. PMID 6041111.
- Tarabichi, Muaaz; Poe, Dennis S.; Nogueira, João Flávio; Alicandri-Ciufelli, Matteo; Badr-El-Dine, Mohamed; Cohen, Michael S.; Dean, Marc; Isaacson, Brandon; Jufas, Nicholas; Lee, Daniel J.; Leuwer, Rudolf (October 2016). "The Eustachian Tube Redefined". Otolaryngologic Clinics of North America. 49 (5): xvii–xx. doi:10.1016/j.otc.2016.07.013. PMID 27565395.