Cardiac arrhythmia (irregular heartbeat) is any of a large and heterogeneous group of conditions in which there is abnormal electrical activity in the heart. The heartbeat may be too fast or too slow, and may be regular or irregular. Some arrhythmias are life-threatening medical emergencies that can result in cardiac arrest. Others cause symptoms such as an abnormal awareness of heart beat (palpitations), and may be merely uncomfortable. These palpitations have also been known to be caused by atrial/ventricular fibrillation, wire faults, and other technical or mechanical issues in cardiac pacemakers/defibrillators. Still others may not be associated with any symptoms at all, but may predispose the patient to potentially life threatening stroke or embolism. SADS, or sudden arrhythmic death syndrome, is a term (as part of sudden unexpected death syndrome) used to describe sudden death due to cardiac arrest brought on by an arrhythmia in the absence of any structural heart disease on autopsy.
The conduction system: Automaticity refers to a cardiac muscle cell firing off an impulse on its own. All of the cells in the heart have the ability to initiate an action potential; however, only some of these cells are designed to routinely trigger heart beats. These cells are found in the conduction system of the heart and include the SA node, AV node, Bundle of His, and Purkinje fibers. The sinoatrial node is a single specialized location in the atrium which has a higher automaticity (a faster pacemaker) than the rest of the heart and, therefore, is usually responsible for setting the heart rate and initiating each heart beat.
In normal electrical activity, each heart beat originates as an electrical impulse from a small area of tissue in the right atrium of the heart called the sinus node or sino-atrial node or SA node. The impulse initially causes both atria to contract, then activates the atrioventricular (or AV) node which is normally the only electrical connection between the atria and the ventricles (main pumping chambers). The impulse then spreads through both ventricles causing a synchronized contraction of the heart muscle and, thus, the pulse. In adults the normal resting heart rate ranges from 60 to 80 beats per minute. The resting heart rate in children is much faster. A slow rhythm (less than 60 beats/min), is labeled bradycardia. This may be caused by a slowed signal from the sinus node (sinus bradycardia), a pause in the normal activity of the sinus node (sinus arrest), or by blocking of the electrical impulse on its way from the atria to the ventricles (AV block or heart block). Heart block comes in varying degrees and severity. Bradycardias may be present in the normally functioning heart of endurance athletes or other well-conditioned persons.
Cardiac conduction system
Electrical mpulse arising in SA node, traversing atria to AV node, then entering ventricle. Rhythm originating at or above AV node constitutes supraventricular tachycardia (SVT).
Arrhythmias - types: Arrhythmia may be classified by rate (normal, tachycardia, bradycardia), or mechanism (automaticity, reentry, fibrillation). It is also appropriate to classify by site of origin. Arrhythmias with atrial origin include: Premature Atrial Contractions (PACs), Wandering Atrial Pacemaker, Atrial flutter , and Atrial fibrillation (Afib). Arrhythmias arising at the junction: Supraventricular tachycardia (SVT), Junctional rhythm, and Junctional tachycardia. Arrythmias arising from pathologies at the AV node (AV blocks): First degree heart block, which manifests as PR prolongation, Second degree heart block, and Third degree heart block, also known as complete heart block.
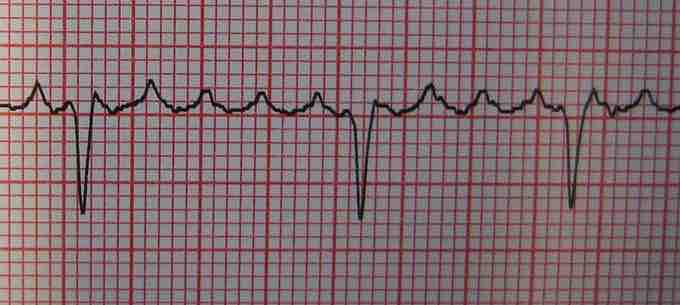
Atrial flutter
Atrial flutter, shown here, is a cardiac arrhythmia that occurs in the atria of the heart and falls into the category of supra-ventricular tachycardias. While this rhythm occurs most often in individuals with cardiovascular disease (e.g. hypertension, coronary artery disease, and cardiomyopathy) and diabetes, it may occur spontaneously in people with otherwise normal hearts. It is typically not a stable rhythm, and frequently degenerates into atrial fibrillation (AF). However, it does rarely persist for months to years.
Arrhythmias - fibrillation: When an entire chamber of the heart is involved in a multiple micro-reentry circuits and, therefore, quivering with chaotic electrical impulses, it is said to be in fibrillation. Fibrillation can affect the atrium (atrial fibrillation) or the ventricle (ventricular fibrillation); ventricular fibrillation is imminently life-threatening. Atrial fibrillation affects the upper chambers of the heart, known as the atria. Atrial fibrillation may be due to serious underlying medical conditions and should be evaluated by a physician. It is not typically a medical emergency. Ventricular fibrillation occurs in the ventricles (lower chambers) of the heart; it is always a medical emergency. If left untreated, ventricular fibrillation (VF, or V-fib) can lead to death within minutes. When a heart goes into V-fib, effective pumping of the blood stops. V-fib is considered a form of cardiac arrest.
Arrhythmias - treatment: Dysrhythmias may also be treated electrically, by applying a shock across the heart — either externally to the chest wall or internally to the heart via implanted electrodes. Cardioversion is either achieved pharmacologically or via the application of a shock synchronized to the underlying heartbeat. It is used for treatment of supraventricular tachycardias. Defibrillation differs in that the shock is not synchronized. It is needed for the chaotic rhythm of ventricular fibrillation and is also used for pulseless ventricular tachycardia. Often, more electricity is required for defibrillation than for cardioversion. In most defibrillation, the recipient has lost consciousness so there is no need for sedation.
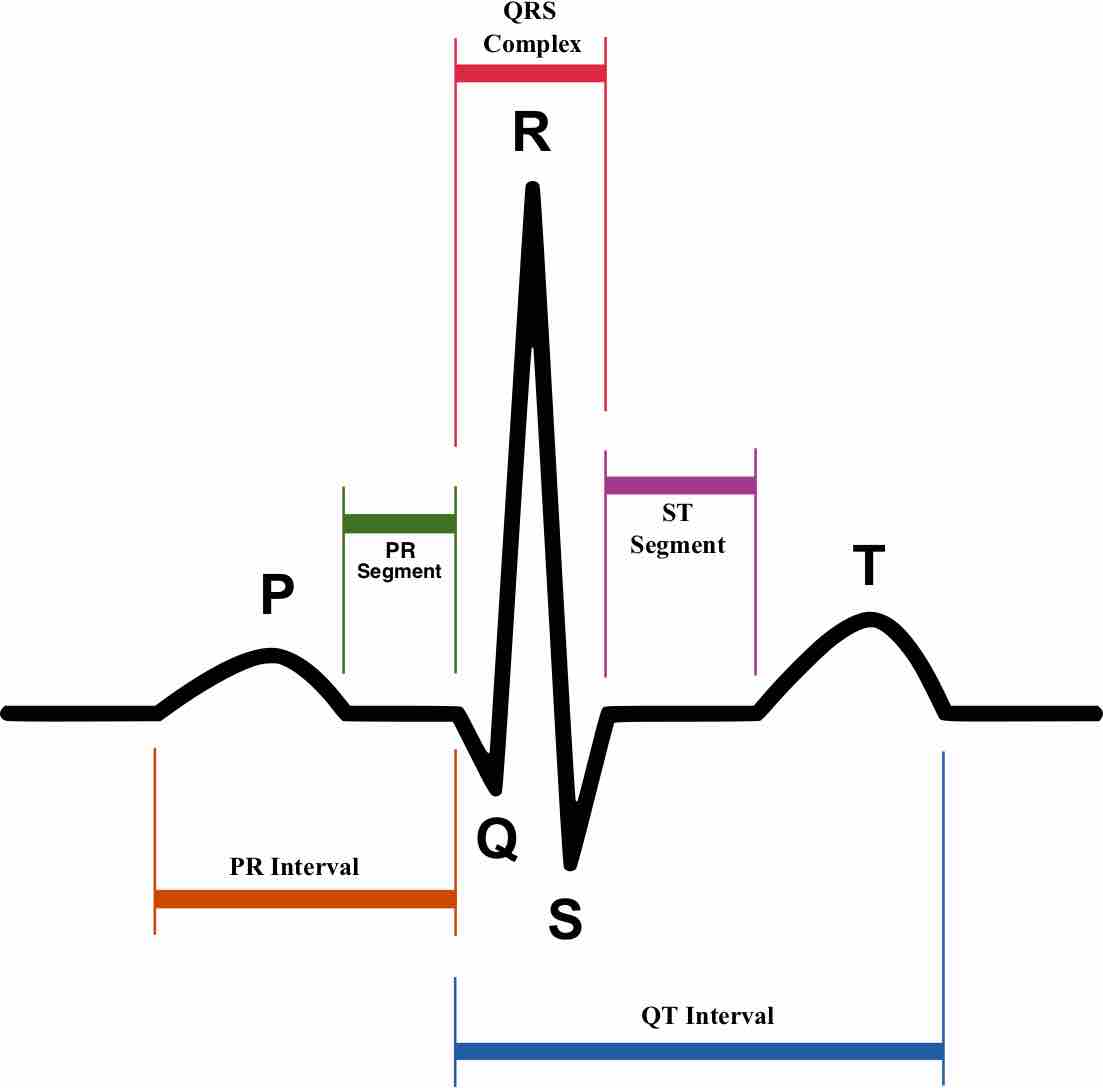
Normal sinus rhythm
Schematic diagram of normal sinus rhythm for a human heart as seen on ECG. In atrial fibrillation, one form of cardiac arrhythmia, the P waves, which represent depolarization of the atria, are absent.