Coronary circulation is the circulation of blood in the blood vessels of the heart muscle. The vessels that deliver oxygen-rich blood to the myocardium are known as coronary arteries. The vessels that remove the deoxygenated blood from the heart muscle are known as cardiac veins. The blood supply to the heart is greater than that of other body tissues since the heart has a constant metabolic demand that must be satisfied to keep the heart pumping at all times.
Coronary Circulation
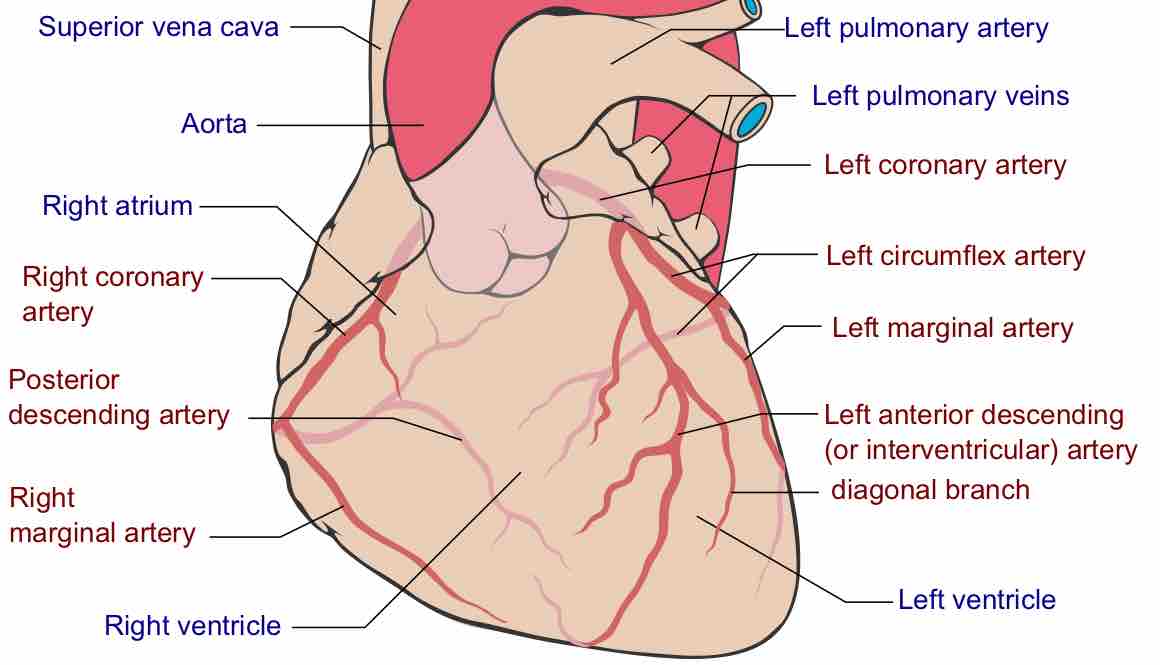
Coronary arteries labeled in red text and other landmarks in blue text.
Coronary Artery Structure
The coronary arteries originate from the left side of the heart descending from the aorta. There are multiple coronary arteries derived from the larger right and left coronary arteries. For example, important coronary arteries that branch off from the larger arteries include the left anterior descending (LAD) coronary and the right posterior coronary.
Coronary arteries run both along the surface of the heart and deep within the myocardium, which has the greatest metabolic demands of all the heart tissues due to its muscle content. Epicardial coronary arteries, which run along on the surface of the heart, are capable of autoregulating vasodilation and vasoconstriction to maintain coronary blood flow at appropriate levels to fit the metabolic demands of the heart muscle. These vessels are relatively narrow and thus vulnerable to blockage, which may cause a myocardial infarction. Subendocardial coronary arteries run deep within the myocardium to provide oxygen throughout the muscle tissue of the cardiac wall.
Systole and Diastole
In systole, the ventricular myocardium contracts, generating high intraventricular pressure and compressing the subendocardial coronary vessels while allowing the epicardial coronary vessels to remain fully open. With the subendocardial coronary vessels compressed, blood flow essentially stops below the surface of the myocardium.
In diastole, the ventricular myocardium contracts, lowering the intraventricular pressure and allowing the subendocardial vessels to become open again. Due to the high pressures generated in the ventricular myocardium during systole, most myocardial tissue perfusion occurs during diastole. Additionally, catecholamines such as norephinephrine, which normally cause vasoconstriction will instead cause vasodilation within the coronary arteries. This mechanism is due to beta-adrenergic receptors in the coronary arteries and helps enable the increased cardiac output associated with fight-or-flight responses.
Myocardial Infarctions
A myocardial infarction (heart attack) may be caused by prolonged ischemia (oxygen deprivation) in the heart, which occurs due to blockage of any of the coronary arteries. Since there is very little unnecessary blood supply to the myocardium, blockage of these vessels can cause serious damage. When these vessels become blocked, the myocardium becomes oxygen-deprived, a condition called ischemia. Brief periods of ischemia in the heart are associated with intense chest pain called angina, which may either be transient if the clot breaks up on its own or stable if it does not. As the time period of ischemia increases, the hypoxic conditions cause muscle tissue to die, causing a myocardial infarction (heart attack).
Myocardial infarction is one of the most common causes of death worldwide. The clots that cause the infarction are usually the result of ruptured atherosclerotic plaques that break off and occlude the coronary arteries, but arterial thrombosis from injury or pooled blood may also cause a heart attack. The tissues of the heart do not regenerate, so those that survive a myocardial infarction will generally have scar tissue in their myocardium and may be more susceptible to other heart problems in the future.