Anatomy, Head and Neck, Sympathetic Chain
- Article Author:
- Nrusheel Kattar
- Article Editor:
- Thomas Flowers
- Updated:
- 10/25/2020 11:48:43 AM
- For CME on this topic:
- Anatomy, Head and Neck, Sympathetic Chain CME
- PubMed Link:
- Anatomy, Head and Neck, Sympathetic Chain
Introduction
The sympathetic nervous system is comprised exclusively of efferent neurons. It divides into the left and right sympathetic chains.[1] Each sympathetic chain extends from the skull base to the coccyx paravertebrally, carrying preganglionic fibers from the spinal cord that synapse in an adjacent ganglion, from which ascending and descending postganglionic fibers head toward viscera.[2][3]
The ganglia adjacent to the sympathetic chain are known as sympathetic chain ganglia, comprised of the cervical, thoracic, lumbar, and sacral ganglia.[4] This article will discuss the defining features of the cervical sympathetic chain and its associated ganglia.
Structure and Function
The cervical sympathetic chain has three adjacent ganglia: superior cervical ganglion, middle cervical ganglion, and inferior cervical ganglion. However, in most (80%) patients, the inferior cervical ganglion is combined with the first thoracic ganglion, forming the cervicothoracic ganglion, commonly referred to as the stellate ganglion.[5]
Superior Cervical Ganglion: The superior cervical ganglion (SCG) has been demonstrated in cadaveric studies to be a fusiform/cylindrical structure that is the largest of the cervical ganglia and most often appears embedded within soft tissue anterior to the transverse processes of the C2-C3 vertebrae.[6][7][8] The average length, width, and thickness of the SCG measured in separate cadaveric studies ranged from 15 to 32 mm, 4.6 to 7.2 mm, and 1.8 to 2.7 mm, respectively.[7][8]
Middle Cervical Ganglion: The middle cervical ganglion (MCG) is the smallest of the cervical ganglia and is often absent.[6] When present, the MCG is located anterior to the transverse process of the C6 vertebra, usually beneath the inferior thyroid artery. In cadaveric studies, the average length and width of the MCG are 6.5 mm and 3.9 mm, respectively.[8]
Stellate Ganglion: The stellate ganglion is a fusiform or bilobed structure located anterior to the transverse process at the level of the C6 vertebra, superior to the subclavian artery & the posterior aspect of the pleura, and posterior to the vertebral vasculature.[4][5][9] Other vital anatomic landmarks include the costocervical trunk, which branches out near the lower aspect of the stellate ganglion, and the superior intercostal artery, which lies lateral to the stellate ganglion.[10] The average length, width, and thickness are reportedly 18.7 mm, 7.0 mm, and 2.5 mm, respectively.[8]
Though all of the cervical ganglia supply postganglionic fibers to the head and neck region, the SCG is the primary contributor via the oculosympathetic pathway (OSP)[6][11][12]:
- First-order neurons descend from the posterolateral hypothalamus to the initial synapse in the intermediolateral (IML) gray substance of the spinal cord at the levels C8-T2 (known as the Ciliospinal Center of Budge-Waller)
- Second-order neurons exit the Ciliospinal Center of Budge-Waller via white rami communicantes (only present between levels T1-L2), followed by ascension through the stellate and middle cervical ganglia (without synapsing) and culminating with synapse in the superior cervical ganglion
- Third-order neurons exit the superior cervical ganglion as postganglionic fibers that travel with either the internal or external carotid artery to reach their final destination (the specific nerves that comprise these postganglionic fibers are covered below under "Nerves").
The anatomy of the sympathetic chain is demonstrated in Figure 1 with its associated plexuses. This article covers the postganglionic fibers associated with each cervical ganglia in detail below under "Nerves." Ultimately, these sympathetic fibers serve key roles in the "fight or flight" mechanics of the autonomic nervous system in the head and neck through pupil dilation, inhibition of tear production, vasoconstriction of skin vasculature, and widening of the palpebral fissures.[4]
Embryology
The autonomic nervous system derives from neural crest cells, a migratory cohort of embryonic cells that arise from neuroepithelial precursors in the neural tube.[13][14] Neural crest cells anterior to somite 5 give rise to sympathetic ganglia, whereas neural crest cells formed posterior to somite 4 give rise to sympathetic neurons.[13] Migration and differentiation of these neural crest cells into the eventual structures of the sympathetic nervous system is under the control of specific expression of receptors and ligands that are unique to each lineage of neural crest cells.[13]
Blood Supply and Lymphatics
The blood supply of the sympathetic trunk can divide into anatomic thirds. The lower third, which begins superior to the stellate ganglion and extends to the middle cervical ganglion, is supplied by branches from the inferior thyroid artery and the subclavian and ascending cervical arteries.[15] The middle third, typically extending from the middle cervical ganglion to the hyoid bone, receives blood supply primarily from the ascending cervical artery with rare contributions from the superior thyroid artery. The upper third of the sympathetic trunk, which runs from the level of the hyoid bone to the skull base, is also supplied by the ascending cervical and superior thyroid arteries.[15]
Despite being anatomically adjacent to the sympathetic trunk, the cervical sympathetic ganglia tend to have a different blood supply:
Superior Cervical Ganglion: The superior cervical ganglion has been shown in cadaveric studies to mostly receive blood supply from branches of the ascending pharyngeal artery with rare branches from the superior thyroid artery.[15]
Middle Cervical Ganglion: The middle cervical ganglion has a variable blood supply, with cadavers demonstrating consistent contributions from either inferior thyroid or ascending cervical arteries.[15]
Inferior Cervical/Stellate Ganglion: The inferior cervical ganglion (when present) and the stellate ganglion both receive vascular supply from the supreme intercostal branch of the costocervical trunk of the subclavian artery.[15]
Nerves
The post-ganglionic fibers of the cervical sympathetic ganglia with their respective courses and destinations are as follows:
Superior Cervical Ganglion [16][17]
- Internal carotid nerve: The internal carotid nerve travels with the internal carotid artery, eventually forming a plexus of nerves that innervate the internal carotid artery, pterygopalatine artery critical eye structures (Müller's muscles, pupillary dilator muscles, orbital vasomotor muscles, and lacrimal glands).
- External carotid nerve: The external carotid network of nerves travel with the common and external carotid arteries to innervate the smooth muscle of arteries, with some fibers traveling with the internal maxillary artery to innervate the sweat glands of the face.
- Gray rami communicantes: Some post-ganglionic fibers distribute to spinal nerves of vertebral levels C1-C4 via gray rami communicantes, which essentially serve as conduits.
- Nerve to pharyngeal plexus: One of the post-ganglionic neurons travels to the pharyngeal plexus, where it becomes intertwined with branches from the vagus and glossopharyngeal nerves.
- Superior cardiac nerve: The superior cardiac nerve travels to the thoracic cavity to reach the cardiac plexus.
Middle Cervical Ganglion [16][17]
- Inferior thyroid nerves: Some post-ganglionic fibers travel along the inferior thyroid artery to innervate the esophagus, pharynx, trachea, and larynx.
- Gray rami communicantes: Post-ganglionic fibers distribute to spinal nerves of C5-C6 vertebral levels.
- Middle cardiac nerve: The middle cardiac nerve travels to the thoracic cavity to reach the cardiac plexus
Inferior Cervical/Stellate Ganglion [16][17]
- Nerves to subclavian and vertebral arteries: Branches to these vessels innervate the smooth muscles in the arteries.
- Gray rami communicantes: Post-ganglionic fibers route to the spinal nerves of C7, C8, and T1.
- Inferior cardiac nerve: The inferior cardiac nerve travels to the thorax and contributes to the cardiac plexus.
Muscles
Physiologic Variants
Cadaveric studies estimate the incidence of the superior, middle, and stellate ganglia as 100%, 81%, and 85%, respectively.[19] In cases where the stellate ganglion was absent, an unfused inferior cervical ganglion and T1 thoracic ganglion were present in 15% of cases.[5]
Whereas the superior cervical ganglion appears bilaterally, the middle and stellate/inferior cervical ganglia vary with both unilateral and bilateral appearance in cadavers.[8]
Surgical Considerations
The cervical sympathetic trunk and ganglia are at risk during surgery involving the carotid sheath and parapharyngeal space as well as during anterolateral approaches to the cervical spine.[17][20][21] A recent case series of 714 neck dissections have demonstrated the incidence of sympathetic chain damage in these cases to be only 0.56%.[22]
As referenced in the "muscles" section above, transverse dissection of the longus colli muscle can lead to sympathetic chain injury since the medial edge of the longus colli approaches closer to the sympathetic structures and further from the midline of the spine as they traverse down the cervical spine.[17] To mitigate risk, surgeons should avoid deviating considerably from the midline spine in lower cervical surgeries via the anterolateral approach and, when possible, avoid excessive stretching of the carotid sheath due to the proximity of the sympathetic structures immediately posterior to this.[8]
Clinical Significance
Horner Syndrome
Horner syndrome can occur due to damage along any point in the OSP (covered above in Structure and Function), including at preganglionic (first- and second-order neurons) and postganglionic (third-order neurons) fibers. [11] The cardinal symptoms of Horner syndrome are ptosis (drooping of upper eyelid), miosis (decrease in pupil size), and anhidrosis (lack of sweat production). Conjunctival hyperemia due to vasodilation of capillaries secondary to sympathetic denervation is a transient acute sign of HS.[11] These clinical findings can vary based on the location of the lesion in the OSP. Pharmacologic testing with cocaine followed by hydroxyamphetamine can help to diagnose Horner Syndrome and then localize the lesion as preganglionic or postganglionic.
The cocaine solution blocks norepinephrine reuptake at the synapse of preganglionic and postganglionic fibers in the OSP, which will manifest as decreased pupillary dilation in patients with Horner syndrome relative to the normal eye (Figure 3).[11] Conversely, hydroxyamphetamine promotes the release of norepinephrine into the postganglionic synaptic cleft, which will manifest as normal pupillary dilation in preganglionic lesions (First- and Second-order neurons) but impaired dilation in postganglionic lesions (third-order neurons) compared to the unaffected eye (Figure 3).
Common first-, second-, and third-order neuron lesions in the OSP (pathway covered above in "Structure and Function") along with differentiating factors are as follows[11]:
- First-Order Neuron Lesions (Preganglionic): Miosis is the most prevalent symptom with the distribution of anhidrosis being the entire half of the body ipsilateral to the lesion. Pharmacologic provocation will show reduced pupillary dilation with cocaine administration, followed by an increase in dilation after administering hydroxyamphetamine.
- Examples: Hypothalamic lesions, Wallenberg syndrome, syringohydromelia, multiple sclerosis, spinal cord neoplasms
- Second-Order Neuron Lesions (Preganglionic): Patients with lesions in second-order neurons typically present with the full spectrum of miosis, ptosis, and anhidrosis (distribution is localized only to the ipsilateral head and neck). Pharmacologic testing with cocaine and hydroxyamphetamine will have the same results as first-order lesions.
- Examples: Pancoast tumors, sympathetic schwannomas, neuroblastic tumors, goiters
- Third-Order Neuron Lesions (Postganglionic): The full triad of ptosis, miosis, and anhidrosis will be present. Lesions proximal to the superior cervical ganglion will have anhidrosis of the entire ipsilateral head and neck. In contrast, lesions distal to the superior cervical ganglion will present with anhidrosis limited only to the ipsilateral forehead and nose. Testing with cocaine solution will show reduced pupillary dilation relative to the normal eye, but hydroxyamphetamine application will reveal no dilation since postganglionic fibers will become depleted of norepinephrine.
- Examples: Fibromuscular dysplasia, carotid dissection, skull base/orbital lesions, parasellar lesions
First-Bite Syndrome
Occasionally, sympathetic trunk division during parapharyngeal space or deep lobe parotid surgery can lead to parotid region pain after the first bite of every meal.[20][21] Typically, this pain resolves after several bites. First-bite syndrome appears to occur due to parasympathetic hyperactivation of parotid gland myoepithelial cells after denervation of sympathetic neurons to the parotid gland.[23]
Ganglion Blocks and Sympathetectomy
Ultrasound-guided injections to the sympathetic ganglia have received attention as treatments for chronic pain.[5] Thoracic sympathectomy has also been an option as a treatment option for intractable angina.[19]
(Click Image to Enlarge)
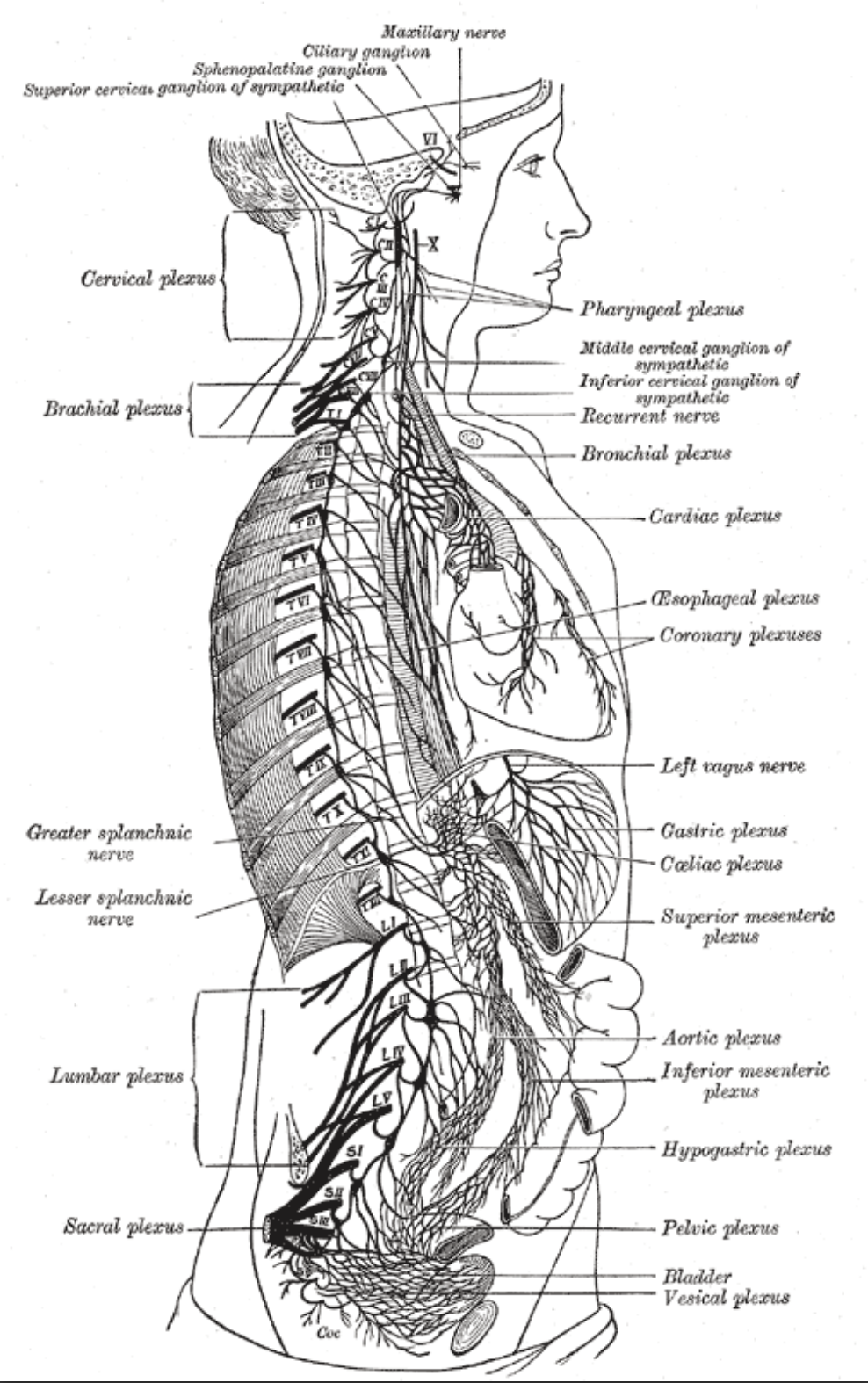
Anatomy of the right sympathetic chain with its associated plexuses
Contributed by Katherine Humphreys from StatPears article "Anatomy, Back, Lumbar Sympathetic Chain".