Activities of Daily Living
- Article Author:
- Peter Edemekong
- Article Author:
- Deb Bomgaars
- Article Author:
- Sukesh Sukumaran
- Article Editor:
- Shoshana Levy
- Updated:
- 6/26/2020 8:24:16 AM
- For CME on this topic:
- Activities of Daily Living CME
- PubMed Link:
- Activities of Daily Living
Introduction
The activities of daily living (ADLs) is a term used to collectively describe fundamental skills that are required to independently care for oneself such as eating, bathing, and mobility. The term activities of daily living was first coined by Sidney Katz in 1950.[1][2]
ADL is used as an indicator of a person’s functional status. The inability to perform ADLs results in the dependence of other individuals and/or mechanical devices. The inability to accomplish essential activities of daily living may lead to unsafe conditions and poor quality of life. Measurement of an individual’s ADL is important as these are predictors of admission to nursing homes, need for alternative living arrangements, hospitalization and use of paid home care. The outcome of a treatment program can also be assessed by reviewing a patient’s ADLs.[3][4][5][6]
Nurses are often the first to note when patients' functionality declines during hospitalization; therefore, routine screening of ADLs is imperative and nursing assessment of ADL's is performed on all hospitalized patients. Hospitalization for an acute or chronic illness may influence a person’s ability to meet personal goals and sustain independent living. Chronic illnesses progress over time, resulting in a physical decline that may lead to a loss of ability to perform ADL's.
In 2011, the United States National Health Interview Survey determined that 20.7% of adults aged 85 or older, 7% of those aged 75 to 84 and 3.4% of those aged 65 to 74 needed help with ADLs. [7][8]
Function
Types of ADL
The activities of daily living are classified into basic ADLs and Instrumental Activities of Daily Living (IADLs). The basic ADLs (BADL) or physical ADL are those skills required to manage one’s basic physical needs including personal hygiene or grooming, dressing, toileting, transferring or ambulating, and eating. The Instrumental Activities of Daily Living (IADLs), which include more complex activities that are related to the ability to live independently in the community. This would include activities such as e.g., managing finances and medications, food preparation, housekeeping, laundry.
Basic ADLs
The basic ADL include the following categories:
- Ambulating: The extent of an individual’s ability to move from one position to another and walk independently.
- Feeding: The ability of a person to feed oneself.
- Dressing: The ability to select appropriate clothes and to put the clothes on.
- Personal hygiene: The ability to bathe and groom oneself and to maintaining dental hygiene, nail and hair care.
- Continence: The ability to control bladder and bowel function
- Toileting: The ability to get to and from the toilet, using it appropriately, and cleaning oneself.
Learning how each basic ADL affects an individual to care for themselves can help determine whether a patient would need daily assistance. It can also help the elderly or disabled people to determine their eligibility got state and federal assistance programs.
Instrumental ADLs
The instrumental ADLs are those that require more complex thinking skills, including organizational skills.
- Transportation and shopping: Ability to procure groceries, attend events Managing transportation, either via driving or by organizing other means of transport.
- Managing finances: This includes the ability to pay bills and managing financial assets.
- Shopping and meal preparation. ie everything required to get a meal on the table. It also covers shopping for clothing and other items required for daily life.
- Housecleaning and home maintenance. Cleaning kitchens after eating, maintaining living areas reasonably clean and tidy, and keeping up with home maintenance.
- Managing communication with others: The ability to manage telephone and mail.
- Managing medications: Ability to obtain medications and taking them as directed.
The IADL differs from ADL as people often begin asking for outside assistance when these tasks become difficult to manage independently. [9]
Causes for limitations in ADLs
Decline or impairment in physical function arises from many conditions. Aging is a natural process that may present a decline in the functional status of patients and is a common cause of subsequent loss of ADLs. [10] Musculoskeletal, neurological, circulatory, or sensory conditions can lead to decreased physical function leading to impairment in ADLs. A cognitive or mental decline can also lead to impaired ADL's. [11] Severe cognitive fluctuations in dementia patients have a significant association with impaired engagement in activities of daily living that negatively affect the quality of life. Social isolation can lead to impairment in instrumental activities of daily living. Other factors such as side effects of medications, social isolation, or the patient's home environment can influence the ability to perform ADLs.[12][13]
Hospitalization and acute illnesses have also been associated with a decline in ADLs. Sands et al reported that among frail older adults, loss of ADL functioning over 1 year is independently associated with both acute hospital admission for acute illness and cognitive impairment. Similarly, Cinvinsky et al performed a prospective observational study that evaluated the changes in ADL function occurring before and after hospital admission. They found that many hospitalized older people are discharged with ADL function that is worse than their baseline function.
Measurement of ADLs
Defining the extent of loss of ADL and IADL is important to help define and ensure appropriate care support. Several checklists have been developed by various entities. Although there is some consensus among what ADLs should be included, there exists significant variability on how these questionnaires ask about ADL functions. [14][15]
The most frequently used checklists are the Katz Index of Independence in Activities of Daily Living and the Lawton Instrumental Activities of Daily Living (IADL) Scale. The Katz scale assesses the basic activities of daily living but does not assess more advanced activities of daily living. The Katz ADL scale is sensitive to changes in declining health status but its limitations include the limited in its ability to measure small elements of change seen in the rehabilitation of older adults. However, it is very useful in creating a common language about patient function for healthcare providers involved in the overall care and discharge planning.[16][1]
The Lawton Instrumental Activities of Daily Living (IADL) Scale is used to evaluate independent living skills (Lawton & Brody, 1969). The instrument is most useful for identifying how a person is functioning at the present time, and to identify improvement or deterioration over time. The scale measures eight domains of function including food preparation, housekeeping, laundering. Individuals are scored according to their highest level of functioning in that category. A summary score ranges from 0 (low function, dependent) to 8 (high function, independent). The scale is easy to administer assessment instrument that provides self-reported information about functional skills necessary to live in the community. Specific deficits identified can assist nurses and other disciplines in planning for safe discharge. The limitations of this scale are that it is a self-administered test rather than the actual demonstration of the functional task. This may lead either to over-estimation or under-estimation of the ability to perform the activity.[17][18]
Clinical Significance
Assessment of ADL's is an important aspect of routine patient assessment and assists healthcare providers to assess the patient’s status, plan, and to intervene appropriately. It is important for a provider to address a patient’s general medical condition when determining his/her level of accomplishing functional capabilities that otherwise ensure independent living and personal care.[4]
An ADL assessment helps to determine whether or not a patient may require further rehabilitation or assistance at home or if a skilled nursing or long-term care facility would be a safer environment for the patient. Inability to ambulate may result in an increased risk of falls. It is well-reported that falls are associated with an increased mortality rate. Individuals who have experienced more than one incidence of falling and are 65 years of age and older tend to have a poor prognosis after a fall. Such falls and subsequent hospitalization also place a burden on healthcare utilization and costs. [19] Other issues to consider before placement in assisted living or nursing home as opposed to independent living at home include a patient’s ability to cook and clean their homes, shop, use of public transportation or drive.[20]
It is important to recognize the impact of a loss of ADL on the patient. Independent living is highly encouraged and advocated in American society, and many aging individuals fear a loss of autonomy.[20][21]
An ADL assessment is also required to determine benefits for disability insurance and long-term care insurance policies. The cost of home care, skilled care, assisted living, and nursing homes is a concern for many families. Not all supportive care is covered by Medicare or private insurance, thus leading to financial concerns for patients and significant others. The high cost of care may lead to decisions that preclude patients from receiving the care required to support ADL's. [22]
Access to care can also be an issue. Often lower socioeconomic groups or disadvantaged persons have difficulty accessing quality care for seniors. Access can be difficult due to transportation, distance, and availability. [23] Though many placements at care facilities are short-term, most patients end up staying longer than a year due to the inability to perform more than two of the six ADLs.[24]
Other Issues
Nurses need to communicate patient ability to perform ADLs and IADLs with providers so that the health care team and their families can discuss if a patient meets the pre-defined criteria to either continue to live in their homes or be placed in assisted living, skilled care, or nursing home facilities. (United States National Library of Medicine, 2017) Depending on the severity of the patient's impairment, most home health nurses complete assessments to make plans for improvements, help with medication administration, and bring resources to assist with independence. Unlicensed assistive personnel help with bathing, light housekeeping, shopping, and activity to support the patient's desire for continued independent living.[25][5]
Enhancing Healthcare Team Outcomes
All healthcare workers, including providers, nurses, physical therapy, and occupational therapy should collaborate to assess the functionality of patients before discharge. Patients who are unable to perform activities of daily living may require further rehabilitation or assistance at home. The inability to dress or toilet can lead to poor quality of life. Difficulty ambulating or transferring can lead to falls and further decline. Difficulty in eating independently can lead to poor nutrition, dehydration, and further weakness. Appropriate referrals to OT, PT, and dieticians should be considered. Assessment of functionality should become routine practice for all patients as it can affect people of all ages. An interprofessional team communicating and collaborating together will provide the best patient evaluation and discharge with good follow up care. The nursing staff should report to the medical team concerns in regards to patients unable to complete ADLs. The clinical team assists in directing the nursing home health and social work coordinators to make sure patients receive the care they need. The home health nursing staff needs to provide ongoing monitoring and reporting back to the clinical team should increase in deficiency of ADLs occur. [Level V]
Nursing, Allied Health, and Interprofessional Team Interventions
The implications and role of a change in ADLs in any particular patient differ among the various stakeholders in the patient’s care team.
- Case Manager, Nurse, and Social Worker
- Primary care Physician
- Home health or Skilled nursing Agencies
- Physical and Occupational Therapy
- Long Term Care Insurance Providers
- Government Agencies
The nurse and care manager typically assess and collect information on a person’s ability to perform ADLs. This data enables them to plan ahead for each person’s continuum of care. The physicians use the assessments to formulate and plan of care which is then provided to the home health agency or skilled nursing agency. The agency will then select the appropriate staff needed for each client. The physical and occupational therapists work with the plan of care and document the progress in ADL to ensure the rehabilitation goals are achieved to the extent possible. Insurance providers and government agents use the assessments of ADL to determine the qualifications of the patient and pay for the services rendered.[5][26]
Nursing, Allied Health, and Interprofessional Team Monitoring
Nurses assess ADLs and IADLs daily in all hospitalized patients. Appropriately assessing, planning, intervening, and evaluating ADLs and IADLs can mean the difference between independent aging and needing daily assistance.
There are many tools included in daily shift assessments, but all nurses should be aware of each patient's needs for assistance in managing ADL's. When a patient is at risk for a change in ADLs or IADLs, the nurse should assist patients and report to the interprofessional team members so that a new plan of care can be established.
Possible NANDA nursing diagnoses include altered health maintenance, defined as a "State in which an individual has no physiological or psychological energy enough to resist or complete required or desired daily activities". Other possible nursing diagnoses include: risk of injury, activity intolerance, social isolation, or ineffective family coping.
(Click Image to Enlarge)
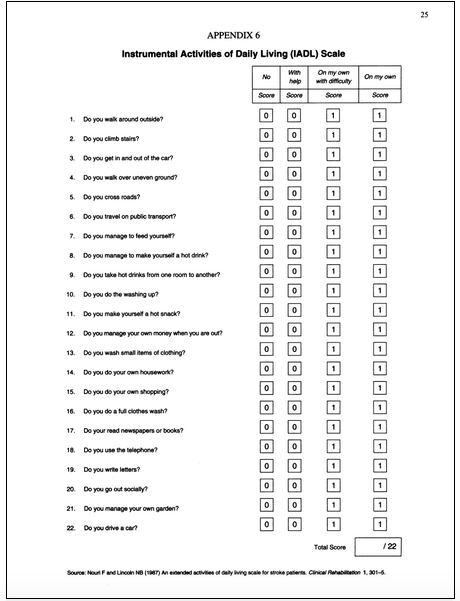
Instrumental Activities of Daily Living
Contributed by the US National Library of Medicine (NIH, 2017)