Acute Stroke
- Article Author:
- Prasanna Tadi
- Article Editor:
- Forshing Lui
- Updated:
- 8/10/2020 5:19:14 PM
- For CME on this topic:
- Acute Stroke CME
- PubMed Link:
- Acute Stroke
Introduction
Acute stroke is also commonly called a cerebrovascular accident which is not a term preferred by most stroke neurologists. Stroke is NOT an accident. The better and more meaningful term is "brain attack", similar in significance to "heart attack". Acute stroke is defined as the acute onset of focal neurological findings in a vascular territory as a result of underlying cerebrovascular disease. In the United States, there are 800,000 new strokes every year. There is one new stroke every 40 seconds. Stroke is the 5th leading cause of death and the first leading cause of disability. There are two main types of strokes. The commoner type is an ischemic stroke, caused by interruption of blood flow to a certain area of the brain. Ischemic stroke accounts for 85% of all acute strokes. 15% of acute strokes are hemorrhagic strokes which are caused by bursting of a blood vessel i.e. acute hemorrhage. There are two main types of hemorrhagic strokes, intracerebral hemorrhage (ICH) and subarachnoid hemorrhage which accounts for about 5% of all strokes.
According to the TOAST[1] classification, there are four main types of ischemic strokes. These are large vessel atherosclerosis, small vessel diseases (lacunar infarcts), cardioembolic strokes and cryptogenic strokes. Each of these has different causes and pathophysiology. Regardless o the type of stroke, it is important to know that with each minute of large vessel ischemic stroke untreated, close to two million neurons die. This is the most important "time is brain" concept in understanding acute stroke and its treatment.
There are numerous causes of stroke, such as prolonged hypertension, arteriosclerosis, and emboli that have formed in the heart as a result of atrial fibrillation or rheumatic heart disease. In younger patients, the possible list of causes may be broadened to include clotting disorders, cervical arterial dissection, and various forms of vasculitis. In the event of a possible stroke presentation, a precise history and physical must be performed alongside emergent neurological imaging before administering any form of treatment. With early, focused treatment based on the stroke etiology, rehabilitation programs, and long-term lifestyle changes, one can maximize his/her chances for a meaningful recovery.[2]
Etiology
There is a multitude of etiologies that can lead to a stroke. Some of the most common risk factors include hypertension, diabetes mellitus, hypercholesterolemia, physical inactivity, obesity, genetics, and smoking. Cerebral emboli commonly originate from the heart, especially in patients with preexisting heart arrhythmias (atrial fibrillation), valvular disease, structural defects (atrial and ventricular septal defects) and chronic rheumatic heart disease. Emboli may lodge in areas of preexisting stenosis.[3] Alcohol intake has a J-shaped relationship with ischemic stroke. Mild to moderate drinking carries a slightly lower risk of ischemic stroke yet heavier drinking increases the risk drastically. Alcohol intake increases the risk of hemorrhagic stroke in a near linear relationship.
Strokes that occur in small vessels(lacunar infarcts) are most commonly caused by chronic, uncontrolled hypertension resulting in the pathological entity of lipohyalinosis and arteriolosclerosis. These strokes occur in the basal ganglia, internal capsule, thalamus, and pons. Uncontrolled hypertension in these areas can also lead to hypertensive intracerebral hemorrhages (ICH).[4]
About 15% of all strokes are classified as hemorrhagic, with the etiology being the most commonly uncontrolled hypertension. Other causes of hemorrhagic strokes include cerebral amyloid angiopathy, a disease in which amyloid plaques deposit in small and medium vessels, which causes vessels to become rigid and more vulnerable to tears. Deposition can occur anywhere, but they occur most commonly on the surfaces of the frontal and parietal lobes. The structural integrity of vessels is another important consideration in hemorrhagic stroke etiology, with aneurysms, arteriovenous malformations, cavernous malformations, capillary telangiectasias, venous angiomas, and vasculitis being more common reasons for stroke.[5]
Epidemiology
Pathophysiology
Atherosclerosis is the most common and important underlying pathology which leads to the formation of an atherothrombotic plaque secondary to low-density lipoprotein cholesterol (LDL) build up in the arteries supplying the brain. These plagues may block or decrease the diameter of the neck or intracranial arteries resulting in distal ischemia of the brain. More commonly they may also rupture. Plague rupture leads to exposure of the underlying cholesterol crystals which attract platelets and fibrin. Release of fibrin-platelet rich emboli causes strokes in the distal arterial territories via an artery-to-artery embolic mechanism. The nature of the cardiac source of emboli depends on the underlying cardiac problem. In atrial fibrillation, clots tend to be formed in the left atrium. These are red blood cell rich clots. There may be tumor emboli in left atrial myxoma and bacterial clumps from vegetations when emboli arise during infective endocarditis.
When an arterial blockage occurs, the immediately adjacent neurons lose their supply of oxygen and nutrients. The inability to go through aerobic metabolism and produce ATP causes the Na+/K+ ATPase pumps to fail, leading to an accumulation of Na+ inside the cells and K+ outside the cells. The Na+ ion accumulation leads to cell depolarization and subsequent glutamate release. Glutamate opens NMDA and AMPA receptors and allows for calcium ions to flow into the cells. A continuous flow of calcium leads to continuous neuronal firing and eventual cell death via excitotoxicity.[8]
In the first 12 hours, there are no significant macroscopic changes. There is cytotoxic edema related to energy production failure with neuronal cellular swelling. This early infarction state can be visualized by diffusion-weighted MRI which shows restricted diffusion as a result of neuronal cellular swelling. Six to twelve hours after the stroke, vasogenic edema develops. This phase may be best visualized with FLAIR sequence MRI. Both cytotoxic and vasogenic edema causes swelling of the infarcted area and increases in intracranial pressure. These are followed by the invasion of phagocytic cells which try to clear away the dead cells. Extensive phagocytosis causes softening and liquefaction of the affected brain tissues, with peak liquefaction occurring 6 months post-stroke. Several months after a stroke, astrocytes form a dense network of glial fibers mixed with capillaries and connective tissue.[9][10]
Hemorrhagic strokes lead to a similar type of cellular dysfunction and concerted events of repair with the addition of blood extravasation and resorption.[11]
History and Physical
Time is brain! An expedited yet thorough history is an absolutely critical first step toward making a diagnosis. A stroke should be high on the differential for a patient presenting with sudden, focal neurological deficits and/or altered level of consciousness. Based on clinical presentation alone, it is difficult to differentiate between a hemorrhagic or ischemic stroke on a consistent basis. Headache at the onset and/or altered level of awareness does indicate more likely a hemorrhage yet a small intracerebral hemorrhage can present clinically exactly like a deep hemisphere ischemic infarction. The signs and symptoms elicited from the history and physical can aid in localizing the affected region. Common signs and symptoms include hemiparesis, sensory deficits, diplopia, dysarthria, and facial droop. Strokes in the posterior circulation present with a sudden onset of ataxia and vertigo. Symptoms commonly attributed to increased intracranial pressure, such as nausea, vomiting, headache, and blurred or double vision, may also provide evidence supporting a hemorrhagic stroke. In addition to gathering information about the symptoms, one needs to establish the time of their onset to decide subsequent therapy once the diagnosis of ischemic stroke is confirmed.[12]
A neurological exam is performed to ascertain stroke location, establish baseline function upon hospital admission, rule out a transient ischemic attack (TIA) and other stroke mimickers, and deduce potential comorbidities. It is composed of testing cranial nerve function, the range of motion and muscle strength, sensory integrity, vibratory sense, cerebellar function, gait, language, mental status, and level of consciousness. Baseline function is determined via the National Institutes of Health Stroke Scale (NIHSS), which focuses on the level of consciousness, visual and motor function, sensation and neglect, cerebellar function, and language capabilities.[13]
In addition to the neurological exam, the neck is examined to rule out signs of meningitis via palpation of the paraspinal musculature and testing the range of motion. Presence of a carotid bruit indicates underlying atherosclerosis. Besides testing extraocular muscle function and the visual field for visual defects, a fundus examination is performed to check for hypertensive changes, retinal hemorrhage, and emboli. A peripheral vasculature exam includes palpation of the carotid, radial, femoral, and posterior tibial pulses. A cardiac exam is also performed to detect murmurs, rubs, gallops, or arrhythmias.[14]
Features of middle cerebral artery stroke:
- Contralateral hemiparesis and hypesthesia (Weakness of arm& face is worse than in the lower limb)
- Gaze towards to side of lesion
- Ipsilateral hemianopsia
- Receptive or expressive aphasia is dominant hemisphere is affected
- Agnosia
- Inattention, neglect
Features of anterior cerebral artery stroke:
- Speech is preserved but there is disinhibition
- Mental status is altered
- Judgment is impaired
- Contralateral cortical sensory deficits
- Contralateral weakness greater in legs than arms
- Urinary incontinence
- Gait apraxia
Posterior cerebral artery stroke:
- Cortical blindness
- Contraletarl homonynous heminopsia
- Altered mental status
- Visual agnosia
- Memory impairment
Vertebral/basilar artery stroke:
- Nystagmus
- Vertigo
- Diploia and visual field deficits
- Dysarthria
- Dysphagua
- Syncope
- Facial hypersthesia
- Ataxia
Evaluation
Emergency CT without contrast is the most important first diagnostic tool utilized to confirm the diagnosis and rule out any bleed or a hemorrhagic stroke. Based on the CT results and symptom onset, a patient may be a candidate for fibrinolytic therapy. A diffusion-weighted MRI is most diagnostic of acute ischemic infarction. It may confirm the diagnosis and also reveal the size and location of the infarction. It is not considered to be the first line imaging due to the time needed to obtain the images and the relative lack of availability. Other MRI protocols especially the diffusion-perfusion mismatch describes the area of tissue at risk ("penumbra") that can be saved with early treatment and identifies patients that benefit from reperfusion therapy beyond the initial 4.5 - 6 hours of an acute ischemic stroke.[15][16] A cardiac pacemaker is still an absolute contraindication for an MRI. A CT angiogram aids in localizing the blockage in the vasculature. It can identify patients with large vessel occlusion for interventional thrombectomy therapy. CT perfusion studies may also identify the ischemic core and penumbra mismatch which may be a guide to a decision on revascularization beyond the 6 hours window. Doppler studies can also be utilized to determine the degree of carotid stenosis.[17]
Labs are drawn to determine the patient’s baseline health and provide potential clues toward stroke etiology. Some of the basic labs include a metabolic panel, complete blood count with differential, lipid profile, hemoglobin A1c (HbA1c), blood urine nitrogen (BUN), creatinine, albumin, and glomerular filtration rate (GFR). Among these, random blood sugar, platelet count and PT/PTT are important to determine if the patient is an IV thrombolysis candidate. In younger patients presenting with stroke symptoms, other labs that might be ordered include a coagulation panel, rheumatoid factor (RF), antinuclear antibodies (ANA), and other markers for vasculitis.[18]
An ECG, echocardiogram and prolonged ECG monitoring may be indicated to rule out a cardiac etiology especially atrial fibrillation in "cryptogenic strokes". An EEG may also be warranted to rule out a post-seizure state.[19]
Treatment / Management
Before any treatment can be administered, the patient must be assessed for stable airway, breathing, and circulation. The next step is to assess if he/she is a candidate for alteplase (rt-PA). The exclusion criteria are based on guidelines from the American Heart Association/American Stroke Association. Fibrinolytic therapy aims to dissolve the clot and restore blood flow to the affected regions. The fibrinolytic must be administered within 3 to 4.5 hours after symptom onset to be effective, depending on exclusion criteria. As with the treatment of myocardial infarction and sepsis care, during a stroke, the "time is brain" approach is important and requires a fast and team-based treatment approach. Mobile stroke units and telemedicine have evolved to reduce time to treatment window.[20][21][22] The time frame for treatment has recently been expanded due to the option of endovascular treatment.[23]
Criteria for Thrombolytic Therapy
- Symptoms suggest an ischemic stroke
- No recent head trauma
- No MI in the past 3 months
- No GI bleed in past 21 days
- No arterial puncture in past 7 days
- No major surgery in the past 2 weeks
- No history of an intracranial bleed
- SBP less than 185 mmHg, DBP less than 111 mmHg
- No recent trauma or bleeding
- Not on any oral anticoagulant
- Blood glucose more than 50 mg/dl and platelet count more than 100,000
A notable potential complication after fibrinolytic therapy is hemorrhage. Hemorrhagic transformation is classified as hemorrhagic infarction and parenchymal hematoma, each with 2 subsets. Hemorrhagic infarctions occur more often than parenchymal hematomas. Predictive factors for the occurrence of this complication include increased infarction area, gray matter location, atrial fibrillation, and cerebral embolism, acute hyperglycemia, low platelet count, and poor collateral circulation.[24]
In recent years there are significant advancements in acute stroke care. Multiple trials published in 2015 showed that endovascular thrombectomy in the first six hours is much better than standard medical care in patients with large vessel occlusion in the anterior circulation. These benefits sustained irrespective of geographical location and patient characteristics. [25]
Again in 2018, a significant paradigm shift happened in stroke care. DAWN and DEFUSE 3 trials showed significant benefits of Endovascular thrombectomy in patients with large vessel occlusion in the arteries of the proximal anterior circulation. This trial extended stroke window up to 16 -24 hours in selected patients using perfusion imaging. Due to this, we can treat more patients even up to 16 - 24 hours. [26][27]
Within 24 to 48 hours of symptoms onset, patients should be placed on antiplatelet therapy, aspirin orally. Blood pressure should be maintained slightly elevated for the first few days after a stroke to improve perfusion to the peri-infarction zones. Blood pressure should also be lowered by no more than 15% if diastolic blood pressure is over 220 mm Hg or if systolic blood pressure is over 120 mm Hg. BP does need to be lower than 180/110 for IV Alteplase therapy. Comorbidities also need to be addressed and managed during the patient’s hospital stay.[28]
Oxygen should be provided if the room air saturation is less than 95%. In addition, both hypo and hyperglycemia should be identified and treated.
Cerebral Edema Management
Cerebral edema reaches a peak at 72-96 hours after a stroke and is diagnosed with a non-contrast CT. Change in mental status, loss of consciousness and pupillary size may be a clue. It is managed with mannitol but the use of corticosteroids remains controversial. Patient positioning, hypothermia, hyperventilation, and hyperosmolar therapy will suffice in most patients.
Seizures
Seizures occur in 2-25% of patients within the first several days following an ischemic stroke. These seizures may require treatment with standard antiepileptic drugs.
Patients are admitted to the stroke unit that is equipped and trained to treat and care for people with stroke. The superiority of stroke units compared to non-specialised units has been proven in studies.[29] Acute stroke treatment is best performed with a team approach involving the stroke neurologist, an interventional neuroradiologist, speech pathologist, physical therapist, occupational therapist, pharmacist, social worker, and the nursing care team. General care of a patient with acute stroke will include BP care as described above, swallowing evaluation and aspiration prevention, IV fluid with isotonic fluids, avoid and treat fever aggressively, treat hyperglycemia, prevent infection and DVT prophylaxis and early evaluation and plan for subsequent rehabilitation.
Differential Diagnosis
The differential diagnosis is broad and can include stroke mimics such as TIA, metabolic derangement (in other words, hypoglycemia, hyponatremia), a hemiplegic migraine, infection, brain tumor, syncope, and conversion disorder.[30]
Prognosis
The prognosis after a stroke is multifactorial, with patient age, stroke severity, stroke etiology, infarct location, and associated comorbidities being significant contributing factors. Stroke complications can also impact a patient’s prognosis. Common complications include pneumonia, deep vein thrombosis, urinary tract infections, and pulmonary embolism. However, patients who do not experience any complications within the first week tend to experience steady neurological improvement. The majority of patients experience the most improvement during the first 3 to 6 months after a stroke.[23]
Deterrence and Patient Education
- Smoking cessation
- Blood pressure control
- Diabetes control
- Low salt diet
- Weight loss
Pearls and Other Issues
"Time is brain" is the most important concept in acute stroke care.
"FAST" approach is most important in educating the public about acute stroke. It stands for facial asymmetry, unilateral arm weakness or drift, speech problem and time - note the time of onset and call 911 immediately.
Non-contrast CT head is the imaging modality of choice in acute stroke.
IV thrombolysis within 3 - 4.5 hours with slightly different contraindications.
Mechanical thrombectomy in Primary Stroke Center with thrombectomy capability or Comprehensive Stroke Centers for anterior circulation ischemic strokes within 6 hours for large vessel occlusion.
Thrombectomy may be extended for wake-up strokes and onset within 16 - 24 hours by selecting patients with a large mismatch of their infarct core and ischemic penumbra.
Enhancing Healthcare Team Outcomes
The prevention and management of stroke is best done with an interprofessional team approach.
Education of the public and Emergency Medical Services(EMS) are extremely important in improving stroke outcomes. The stroke system of care varies among different counties depending on the availability of accredited primary or comprehensive stroke centers and the different EMS guidelines about where to send the patients.
During the time-dependent early stroke phase and rehabilitation, stroke care involves an interprofessional team to manage the disease.[31] Evidence reveals that hospitals with stroke teams with demonstrated knowledge in stroke and decreased door to needle times have decreased mortality and improved outcomes. The acute care of a stroke patient requires close cooperation between the radiologist, neurologist, emergency department physician, emergency nurses, neurology ICU nurses, and the pharmacist. Each of these professionals plays a role in the diagnosis and management of the acute stroke patient. Often, the emergency nurse is the first individual that encounters the stroke patient, usually during triage. Recognizing the condition and implementing the stroke team's involvement is crucial. The emergency pharmacist needs to assist in rapidly reviewing for any potential drug interactions and appropriate dosing of acute treatments provided.
Once the diagnosis of stroke is made and acutely treated, the patient may need extensive physical rehabilitation, speech therapy and/or a dietary consult. For those who recover function within 3 months, the prognosis is good, but for those with residual neurological deficits, the outcome is guarded. Nursing rehabilitation and physical therapists at this point play a crucial role in providing family and patient education as often activities of daily living may be a challenge.
Secondary prevention after an acute stroke depends on the underlying stroke mechanism. An acute ischemic stroke due to an underlying symptomatic extracranial large artery stenosis of >70% is best treated with carotid endarterectomy in most cases and stenting in some selected cases. A cardiac source of cerebral embolism, most commonly due to atrial fibrillation is best treated with long term oral anticoagulation. A small vessel lacunar infarct is best prevented with an antiplatelet agent and good control of hypertension. Finally, a combination multimodality approach including an antiplatelet agent, good BP control, good blood sugar control, high dose statin, healthy diet, weight control, tobacco quitting and healthy lifestyle are able to prevent at least 80% of subsequent strokes.[32]
Management of stroke is one of the single most difficult and challenging issues for health professionals. Only through an interprofessional approach will the best outcomes be achieved. [Level V]
(Click Image to Enlarge)
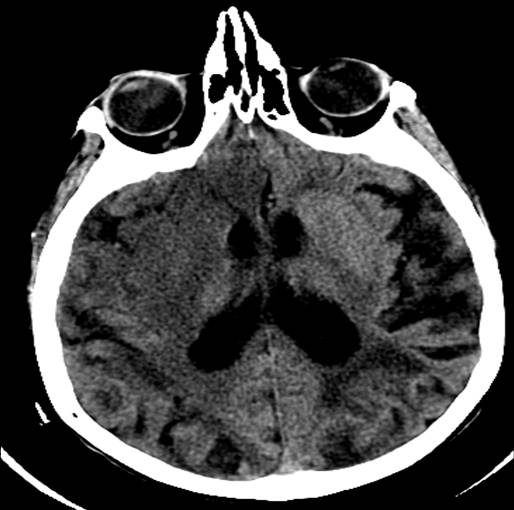
CT head RIght MCA Stroke
Contributed by Scott Dulebohn, MD
(Click Image to Enlarge)

Illustration of an embolic stroke, showing a blockage lodged in a blood vessel.
Contributed by Blausen Medical Communications, Inc. - Donated via OTRS
(Click Image to Enlarge)

Stroke, Posterior Cerebral Artery
Contributed by Dr. Okkes KUYBU, M.D.