Anisocoria
- Article Author:
- William Payne
- Article Editor:
- Michael Barrett
- Updated:
- 8/10/2020 10:51:47 PM
- For CME on this topic:
- Anisocoria CME
- PubMed Link:
- Anisocoria
Introduction
Anisocoria has a wide range of causes, from those which are benign extending to those which are life-threatening. There are many complicated pathways involved in determining pupillary size and reactivity. Pupillary size may be influenced by systemic drug use or topical ophthalmics. Anisocoria also may be present in a cluster headache with lacrimation and rhinorrhea. Other rare forms of a headache also may invoke anisocoria. Additionally, some autonomic ganglion pathology may manifest as anisocoria. Also, there are reports of a variety of unusual causes involving a number of medicines as well as surgical procedures that usually occur on the face. Although anisocoria may be caused by abnormalities or injuries of the iris dilation and sphincter muscles, this discussion concentrates on specific neurologic abnormalities as the cause.[1][2][3][4]
Etiology
Pupillary size is controlled by both parasympathetic and sympathetic neurological pathways acting on the dilator and constrictor muscles of the pupillary sphincter of the iris. Lesions anywhere along these pathways may alter the neurological input to cause an imbalance, leading to a variation in pupillary size from one pupil to the other. Additionally, injuries or structural lesions of the sphincter itself may cause anisocoria. Pharmacological agents may lead to anisocoria along neurological pathways without causing lesions. The challenge with anisocoria is first to evaluate whether the small or large pupil is abnormal and then to ascertain a specific etiology from the possible diagnoses. Depending on the findings, minimal or extensive workup may be required.[5][6][7][8]
Epidemiology
Anisocoria is usually defined as a pupillary inequality of 0.4mm, seldom is it greater 0.8mm. It is almost universally noted to be less than 10mm. The prevalence at any one moment is given at 15-40% but generally considered to be about 20%. Perhaps 15-30% or more of the population may exhibit physiologic anisocoria which is less than 1mm and stable in light and dark conditions. This category of anisocoria is unchanged in light and dark, and the pupil reacts briskly to light. This finding is stable over time.
Pathophysiology
Anisocoria can be caused due to:
1. Constriction of pupil on one side - As a result of the involvement of the sympathetic pathway fibers
2. Dilatation of pupil on one side - As a result of the involvement of parasympathetic (oculomotor) fibers
History and Physical
The first approach is to decide which pupil is abnormal. Anisocoria greater in the light indicates the large pupil to be abnormal due to poor pupillary contraction from the parasympathetic abnormality. An example is a third nerve palsy. Anisocoria greater in the dark shows the small pupil to be abnormal which indicates poor dilation from impairment in the sympathetic system. An example is Horner syndrome.
The examination room should be dimly lit. An accurate assessment of anisocoria cannot be done in a brightly lit room. The patient should focus on a distant object to avoid miosis from a near pupillary reaction which may confuse the response to the examiner’s light.
Evaluation
Distinct pathways control miosis and mydriasis. The parasympathetic pathway causes miosis by activating the iris sphincter. These pathways rise within the brain stem and then extend along cranial nerve III to finally innervate the iris sphincter to cause miosis. There are four neurons involved in this pathway. Dilation is caused by a sympathetic pathway which dilates the iris to cause mydriasis. Sympathetic fibers arise in the hypothalamus, extend to synapse at the C8-T2 spinal cord level, and finally, course through the sympathetic chain to synapse with a third neuron in the superior cervical ganglion which travels with the internal carotid artery and then cranial nerve VI to reach the iris dilator. Three neurons comprise this pathway. Although complicated, these pathways illustrate that dilated or constricted pupils are influenced by different anatomical areas and may exhibit different secondary symptoms.[9][10]
Treatment / Management
The treatment of anisocoria depends on the underlying condition causing the condition.
A posterior communicating artery aneurysm causing oculomotor palsy may need surgical clipping. An intracranial bleed causing the same may need a prompt evacuation. Pathology in the lungs or thyroid causing sympathetic involvemnt and anisocoria may need appropriate treatment.
Differential Diagnosis
Third nerve palsy (TNP) may spare the pupil or cause it to dilate with no reaction to light or convergence. Isolated pupillary dilation is not classically considered a third nerve palsy; however, careful evaluation for subtle ptosis or abnormal extraocular movement is necessary to eliminate a TNP using this criterion. The most well-known, life-threatening cause of TNP is a posterior communicating artery aneurysm causing pressure on the third nerve. Patients usually experience pain with this entity. Diagnosis is radiological with computed tomogram (CT) or magnetic resonance imaging (MRI). Magnetic resonance angiogram (MRA) has a threshold 3 to 5 mm and may indicate other pathologies. CTA has a resolution down to 1 to 2mm. TNP is an example of a large, abnormal pupil.
Tonic pupil, or Adie pupil, is a well-known cause of anisocoria. Here the large pupil is also abnormal. The pupil is large and more commonly occurs in young women. The affected pupil demonstrates a response with poor constriction to light but significantly better to accommodation; this is referred to as light near dissociation. The tonic pupil is often benign but may eventually become miotic. Anatomical abnormalities may exist to cause this entity. The diagnosis of a tonic pupil is usually clinical. There are no cranial nerve palsies in tonic pupil cases.
Pharmacologic agents may cause both mydriasis, which is more common, and miosis. Dilating agents are nasal vasoconstrictors, scopolamine patches, glycopyrrolate deodorants, and various herbals, such as Jimson weed. Small pupils may be caused by opiates, clonidine, organophosphates, pilocarpine, and prostaglandins. The diagnostic approach first involves a careful ophthalmological examination. A dilated pupil can be tested pharmacologically. The muscarinic agent pilocarpine, both dilute (0.05-0.15) and non-dilute (1% to 2%), acts on the neuromuscular junction of the pupillary constrictor to cause miosis. Dilute pilocarpine will cause constriction in a dilated pupil of greater than two weeks duration due to denervation of the neuromuscular junction. This previously was thought to help differentiate this form of mydriasis from TNP, but newer results cast some questions on this. If non-dilute pilocarpine fails to constrict the pupil, then the pupil is pharmacologically dilated.
Horner syndrome (HS) involves an abnormally small pupil. Classic clinical findings are unilateral miosis, ptosis, and anhydrosis, which may be present in any combination and also be incomplete and difficult to ascertain. Dilation lag of the pupil in the dark may be helpful (greatest at 5 sec and less at 25 sec). No abnormality of pupillary constriction to light or near occurs. Four percent to 10% of cocaine may be used as one confirmation of the diagnosis, and 0.5% to 1% apraclonidine is also used. Cocaine blocks norepinephrine reuptake, resulting in pupillary dilation 45 to 60 minutes after use. The pupil in Horner will minimally dilate or not dilate at all; post drop anisocoria of 0.8mm or more is positive. Apraclonidine has different findings; thirty to 45 minutes after using, the abnormal eyelid will rise, and the pupil dilates to “reverse” the deficit. The normal pupil will be unchanged or slightly smaller. Apraclonidine relies on super denervation sensitivity; the minimum time is 36 hours, and it may take a week or longer.
Neither of the above agents is any value in the localization of the lesion in the sympathetic chain. As noted earlier, the sympathetic pathway for mydriasis is long. First-order neurons, which originate in the hypothalamus, may be affected by the hypothalamic, brain stem, cervical cord lesions, or other causes. Second-order neurons may be affected by the pathology of the lung, thyroid, sympathetic chain, and other causes. Third-order neurons may indicate carotid pathology or cavernous sinus lesions or other abnormalities such as a lesion of the sixth nerve. Hydroxyamphetamine (1%) may distinguish third from first- and second-order neuron etiologies. Hydroxyamphetamine releases norepinephrine and causes bilateral pupillary dilation when first- or second-order neurons are involved. Failure for the Horner pupil to dilate indicates third-order neuron dysfunction. Use must wait 48 hours after cocaine or apraclonidine, and false-positive and negative rates are high. Radiological workup involves MRI of the neck and MRA. Comprehensive imagining in adults extends to the brain, neck, and chest.
Prognosis
The prognosis of anisocoria depends on the etiological factor. If a head injury patient has anisocoria, it can denote a bad prognosis. The same applies to a lung or thyroid malignancy causing Horner syndrome and resultant anisocoria.
Complications
As such, anisocoria is less likely to cause complications. If an intracranial bleed is causing anisocoria, it denotes an uncal herniation and later on leads to posterior cerebral artery compression and infarction of the occipital lobe.
Deterrence and Patient Education
Anisocoria is a clinical sign and patients may not be able to identify this. However, they can be educated to report to the hospital if they develop a sudden severe headache, blood in sputum or sudden blurring of vision.
Pearls and Other Issues
Anisocoria has a variety of causes, many of which may be benign. The two entities causing anisocoria that are the most significant to the clinician and require prompt and accurate diagnosis are TNP and Horner syndrome. TNP is potentially life-threatening if caused by an aneurysm, and Horner’s syndrome can indicate carotid dissection among many other possibilities. A comprehensive radiological workup may be required in these cases. A final point is that an accurate examination is essential in evaluating anisocoria; this can only be done in a darkened room with the patient focusing on a distant object.
Enhancing Healthcare Team Outcomes
The primary care provider, nurse practitioner or emergency department physician may come across a patient with uneven pupils. It is important to know that while the condition can be benign, there are many serious pathologies associated with this eye finding.
Anisocoria has a wide range of causes, from those which are benign extending to those which are life-threatening. There are many complicated pathways involved in determining pupillary size and reactivity. Pupillary size may be influenced by systemic drug use or topical ophthalmics. Anisocoria also may be present in a cluster headache with lacrimation and rhinorrhea. Other rare forms of a headache also may invoke anisocoria. Additionally, some autonomic ganglion pathology may manifest as anisocoria. Also, there are reports of a variety of unusual causes involving a number of medicines as well as surgical procedures that usually occur on the face.[7] Although anisocoria may be caused by abnormalities or injuries of the iris dilation and sphincter muscles, this discussion concentrates on specific neurologic abnormalities as the cause. A referral to a neurologist and/or ophthalmologist is highly recommended in cases of acute anisocoria.[10]
(Click Image to Enlarge)
Anisocoria
Contributed by Steve Bhimji, MS, MD, PhD
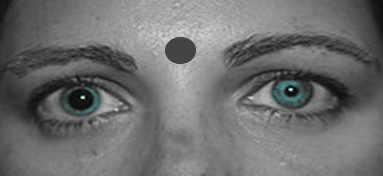
(Click Image to Enlarge)

Anisocoria (unequal pupils)
Image courtesy S Bhimji