Anatomy, Back
- Article Author:
- Robert Modes
- Article Editor:
- Sevda Lafci Fahrioglu
- Updated:
- 7/27/2020 9:18:26 PM
- For CME on this topic:
- Anatomy, Back CME
- PubMed Link:
- Anatomy, Back
Introduction
The back is the posterior portion of the human body between the neck superiorly and the pelvis inferiorly.
The human back is composed of skin and fascia overlying the vertebral column, scapulae, muscle groups, nerves, and arterial supply. The primary motions of the back are flexion/extension, side bending, and rotation.[1]
Structure and Function
The back serves many different functions in the human body. It primarily serves as the primary structural support for the human torso as well as allowing flexibility for movement. Running centrally down the posterior midline is the spinal column. The spinal column is composed of bony vertebra which house and protect the human spinal cord.[2] The column is a continuation of the seven cervical vertebrae in the neck and is composed of twelve thoracic vertebrae, located more superiorly, and five inferior lumbar vertebrae. The column terminates in the sacrum. Ribs articulate with the twelve thoracic vertebrae. Two bony scapulae are situated on either side of the spinal column laterally.[3] They function to provide a bony attachment for several muscles, including the rotator cuff muscles of the upper extremity.[3] In addition to the bones, three groups of muscles comprise the back. The intrinsic muscle group, also known as the deep group, the superficial muscle group, and the intermediate muscle group.[1] These groups serve to allow primary movements in the back, including flexion/extension, rotation, and side bending, movement of the limbs, and assistance in the respiratory effort.[1]
Embryology
The development of the structures in the back stems from early divisions of several key embryologic structures. In the third week of human development, germ layers form during a process called gastrulation.[4] The three germ layers in human development are the ectoderm, the mesoderm, and the endoderm.[4] The paraxial mesoderm, which forms the dermis of the skin, also develops the skeletal muscles in the body and the majority of the axial skeleton.[4] The epidermis of the skin in the back derives from the ectoderm.[4] The spinal cord derives from an ectodermal structure called the neural plate.[5][4] The neural plate develops neural folds bilaterally that rise, come together and fuse to form the neural tube.[5] The tube completely fuses and separate from communication with the amniotic cavity by day 27. Failure of this fusion can result in the condition anencephaly.[6]
Blood Supply and Lymphatics
Blood supply to the skin and muscles in the back is primarily from dorsal branches of the posterior intercostal arteries. These arteries arise from intercostal arteries, or in some variants from the descending aorta directly.[7] The intercostal arteries run in a groove along with the intercostal vein and nerve caudal to the ribs.[8][9] The thoracic aorta runs anteriorly to the vertebral column and slightly lateral on the left side. The azygous and hemiazygous veins may also be present anterior to the spinal cord. The spinal cord itself has several different sources of blood supply, depending on location and embryological development.[2] The anterior spinal artery, the posterior spinal arteries, and the artery of Adamkiewicz are responsible for vascular supply to the spinal cord.[2]
Nerves
Nervous supply to the back primarily arises from dorsal branches of spinal nerves, also known as rami. The sensory innervation to the back organizes in a dermatomal pattern, which corresponds to a specific spinal nerve at different spinal nerves.[10] In addition to providing sensation the skin of the back, the dorsal rami also serve to innervate the intrinsic muscles of the back.[11] This innervation is in contrast to the extrinsic muscles of the back, which are innervated by ventral rami.[12]
Muscles
The muscles of the back subdivide into three categories.[1]
The first category is the superficial, or extrinsic, back muscles.[3] These muscles are located posteriorly on the back, but they assist in the movement of the limbs.[3] The superficial muscles include:
- Trapezius
- Latissimus dorsi
- Levator scapulae
- Rhomboids
The second group of muscles is the intermediate group. These muscles assist in the human respiratory effort and intimately associate with the ribs.[1] This muscle group consists of:
- Serratus posterior inferior
- Serratus posterior superior
The final group of muscles is known as intrinsic or deep muscles.[1] These muscles are responsible for the motion of the axial skeleton. The main movements are flexion/extension, side bending, and rotation.[1] This group further subdivides into several categories in the back and neck. The main muscle groups in the intrinsic muscle group are the erector spinae group and the transversospinalis group.[1] The erector spinae group, medially to laterally, consists of:
- Iliocostalis
- Longissimus
- Spinalis
The muscle group is bilateral on either side of the vertebral column and when both sides are engaged function as the primary extensor of the back.[1] Unilaterally they assist with lateral bending and rotation of the spine.[1]
The second component of the intrinsic muscles in the human back is the transversospinalis group.[1] These muscles are deep to the erector spinae group.[1] The transversospinalis group consists, from superficial to deep, of:
- Semispinalis
- Multifidus
- Rotatores
Like the erector spinae group, the transversospinalis group is located bilaterally on the vertebral column between the transverse processes and the spinous processes. These muscles assist in bending the back posteriorly when contracted bilaterally.[1] When unilateral contraction occurs, they are responsible for assisting with lateral bending and rotation.[1]
Surgical Considerations
The primary surgical considerations with the back have to deal with the placement of the needle for the administration of spinal anesthesia before surgical procedures. The conus medullaris is the most distal end of the spinal cord and must be avoided. The conus medullaris terminates at the level of L2/L3 in newborns,[13] and is at the L1 level in adults.[14] The surgeon inserts a needle into the dural sac between the L3/L4 levels in adults to avoid the conus medullaris during the administration of anesthesia prior to surgery.[14]
Clinical Significance
Generalized back pain is a common presenting symptom for patients. The underlying etiology of the pain most commonly traces to a strain of the skeletal muscle. The differential for back pain is vast, and lumbar disc issues, like herniation or rupture, and fractures must merit consideration.[15] Additionally, osteoarthritis and spondylolisthesis, a condition where a vertebra slips anteriorly compared to the others in the column, can both be causes of back pain.[16]
Spina bifida is a congenital condition seen on the back when there is incomplete closure of the vertebral column. There are three different subcategories of the condition.[17]
Spina bifida occulta is the result of the incomplete fusion of the vertebral arch. The patients are usually asymptomatic, and the only clinical index of suspicion may be a small tuft of hair overlying the defect.[17]
Spina bifida cystica with meningocele occurs when the bony vertebral arch fails to form, and there is a herniation of the spinal meninges.[17]
Spina bifida cystica with meningomyelocele is the most severe and involves herniation of the meninges and the spinal cord.[18]
(Click Image to Enlarge)

Major and Minor Oblique muscles of the Head, Occipital Bone, Oblique Superior and Inferior, Rectus posterior Major and Minor, Semispinalis Capitis, Longissimus Capitis, Semispinalis Cervicis, Longissimus Cervicis, Semispinalis Dorsi, Spinalis Dorsi, Longissimus Dorsi, Iliocostalis Dorsi, Iliocostalis Lumborum,Multifidus, Quadratus Lumborum, Sacrospinalis, Crest of the Ilium
Contributed by Gray's Anatomy
(Click Image to Enlarge)
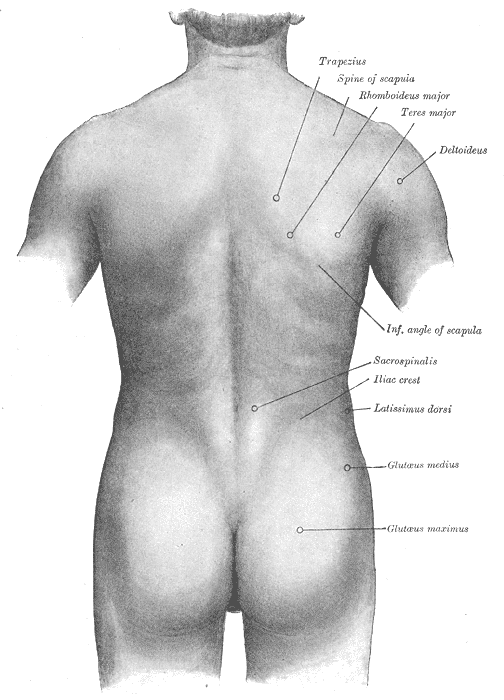
Surface anatomy of the back, Trapezius, Spine of Scapula, Rhomboideus major, Teres Major, Deltoideus, Inferior Angle of Scapula, Sacrospinalis, Iliac crest, Latissimus Dorsi, Glutaeus Medius and Maximus
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)

Extrinsic back muscles
Image courtesy S Bhimji MD