Bell Palsy
- Article Author:
- Matthew Warner
- Article Author:
- Julia Hutchison
- Article Editor:
- Matthew Varacallo
- Updated:
- 8/10/2020 9:05:04 PM
- For CME on this topic:
- Bell Palsy CME
- PubMed Link:
- Bell Palsy
Introduction
Bell palsy (BP) is the most common peripheral paralysis of the seventh cranial nerve with an onset that is rapid and unilateral. The diagnosis is one of exclusion and most often made on physical exam. The facial nerve has both an intracranial, intratemporal, and extratemporal course as its branches. The facial nerve has a motor and parasympathetic function as well as taste to the anterior two-thirds of the tongue. It also controls salivary and lacrimal glands. The motor function of the peripheral facial nerve controls the upper and lower facial muscles. As a result, the diagnosis of BP requires special attention to forehead muscle strength. If forehead strength is preserved, a central cause of weakness should be considered. Although the utility of antivirals has been called into question, treatment is medical with most sources recommending a combination of corticosteroids and antiviral medication.[1][2][3]
BP is the most common cause of unilateral facial paralysis. It is more common in patients with diabetes mellitus and in pregnant females.
Etiology
BP is by definition idiopathic in nature. Increasing evidence in the literature demonstrates multiple potential clinical conditions and pathologies known to manifest, at least in part, with a period of unilateral facial paralysis. The literature has highlighted several viral illnesses such as herpes simplex virus, varicella-zoster virus, and Epstein-Barr virus. Providers may ambiguously (and incorrectly) refer to a diagnosis of BP in the setting of a potentially known etiologic mechanism. This can occur, for example, in the setting of known associations (e.g. Ramsay-Hunt syndrome and Lyme disease).[4]
While there are many potential causes, including idiopathic, traumatic, neoplastic, congenital, and autoimmune, about 70% of facial nerve palsies wind up with a diagnosis of BP.
Epidemiology
The annual incidence is 15 to 20 per 100,000 with 40,000 new cases each year and the lifetime risk is 1 in 60. There is an 8% to 12% recurrence rate. Even without treatment, 70% of patients will have complete resolution. There is no gender or racial preference, and palsy can occur at any age, but more cases are seen in mid and late-life with the median age of onset at 40 years. Risk factors include diabetes, pregnancy, preeclampsia, obesity, and hypertension.[5]
Pathophysiology
BP is thought to result from compression of the seventh cranial nerve at the geniculate ganglion. The first portion of the facial canal, the labyrinthine segment, is the narrowest and it is here that most cases of compression occur. Due to the narrow opening of the facial canal, inflammation causes compression and ischemia of the nerve. The most common finding is a unilateral facial weakness that includes the muscles of the forehead.
History and Physical
Patients present with rapid and progressive symptoms over the course of a day to a week often reaching a peak in severity on 72 hours. Weakness will be partial or complete to one-half of the face, resulting in weakness of the eyebrows, forehead, and angle of the mouth. Patients may present with an inability to close the affected eyelid or lip on the affected side.
The key physical exam finding is a partial or complete weakness of the forehead. If forehead strength is preserved, a central cause should be investigated. Patients may also complain of a difference in taste, sensitivity to sound, otalgia, and changes to tearing and salivation.
Ocular features include
- Corneal exposure
- Lagophthalmos
- Brow droop
- Paralytic ectropion of the lower lid
- Upper eyelid retraction
- Decreased tear output
- Loss of nasolabial fold
Evaluation
History and physical examination guide the evaluation. The House-Brackmann Facial Nerve Grading System can be used to describe the degree of facial nerve weakness. This grading system goes from a grade of I (no weakness) to VI (complete weakness). If the presentation is consistent with BP, there are no required lab or radiographic tests. If there are atypical features, patients may need to be evaluated for a central cause of their symptoms. Likewise, Lyme disease testing is based on a history of possible tick-borne illnesses. The routine testing for Lyme disease is not recommended without other findings of the disease such as a history of a tick bite, skin rash or arthritis. Diabetic testing should not be performed as facial nerve palsy is not considered diabetic neuropathy. There is no consensus on the optimal timing of imaging for Lyme disease, but most sources recommend after 2 months of no improvement of the facial palsy. Magnetic Resonance Imaging (MRI) is the imaging modality of choice. MRI can detect facial nerve inflammation as well as ruling out other conditions such as schwannoma, hemangioma or a space-occupying lesion.[6]
Nerve conduction studies and Electromyography (EMG) may help determine outcomes in patients with severe BP.
Electroneurgraphy uses EMG to monitor the difference in potentials generated by the facial muscles on both sides.
If hearing loss is suspected than auditory evoked potentials and audiography should be performed.
There is a grading system for clinical evaluation of BP. The grading system ranges from mild to severe dysfunction.
Other tests include testing for saliva flow, tear function, and nerve excitability.
Treatment / Management
It is important to know that spontaneous recovery does occur and hence the role of treatment remains questionable.
Corticosteroids are the main treatment with a common regimen consisting of 60 mg to 80 mg a day for approximately 1 week. There is also some evidence stating corticosteroids and antivirals combined improved the outcome of BP compared with corticosteroids alone. A meta-analysis in 2009 found that steroids alone were the treatment of BP and the addition of antivirals did not meet statistical significance.
For patients with severe facial nerve palsy (House-Brackmann IV or greater) can be offered combination therapy with steroids and antivirals. There was no significant increase in adverse reactions from antivirals compared with either placebo or corticosteroids. Patients should be instructed to use eye lubrication and patch the affected eye at bedtime to reduce the likelihood of a corneal abrasion.
Surgical options can be considered when there is no improvement in symptoms after weeks or months. Techniques to present eye desiccation range from eyelid weights to muscle transfers. Facial nerve decompression has not been found to be a recommended treatment option and is considered on a case by case basis. Prior studies evaluating facial nerve compression have been of poor quality. It is recommended to refer to a specialist (plastic surgery, neurology, otolaryngology) sooner rather than later if no improvement has been seen in 4 weeks to explore more aggressive treatments.[7][8][9]
Differential Diagnosis
Causes of peripheral seventh nerve palsy such as Lyme disease and Ramsey Hunt syndrome should be excluded. Other less common causes of facial palsy include tuberculosis, HIV, trauma, sarcoidosis, vasculitis, and neoplasm. There is a reported 10.8% misdiagnosis rate from specialty referral centers. Also, if there are episodes of recurrence, clinicians should consider Melkersson-Rosenthal syndrome. This is a rare neurocutaneous syndrome with a recurrence of facial palsy, orofacial edema, and a fissured tongue. Melkersson-Rosenthal syndrome is more commonly diagnosed in females.
Prognosis
In 71% of untreated cases, BP resolves completely without treatment. Treatment with corticosteroids has been found to increase the likelihood of improved nerve recovery. Recurrence does occur, and one study found a recurrence rate of 12%.[8] Another study reported up to 10% of patients afflicted with BP will experience symptomatic recurrence after a mean latency of 10 years [10].
Risk factors associated with poor outcomes include 1) complete paralysis 2) age more than 60 and 3) decreased salivation or taste on the ipsilateral side. The longer the recovery, the more likely that residual sequelae may develop.
A recurrence rate of 5-15% has been reported.
Complications
- Corneal dryness leading to visual loss
- Permanent damage to the facial nerve
- Abnormal growth of nerve fibers
Postoperative and Rehabilitation Care
Continued monitoring of patients with BP is required to ensure that recovery is taking place. If the EMG studies show that less than 25% of muscles are involved, then supportive care is recommended. But if the paralysis is severe, the patient will need counseling.
Consultations
- Ophthalmologist
- Neurologist
- ENT surgeon
Pearls and Other Issues
As stated, the misdiagnosis rate can be up to 10.8%, so careful history, and physical exam is essential. The focus on the physical exam is the forehead muscles. Since BP is a peripheral facial nerve palsy, there needs to be involvement of the forehead muscles. The history and physical guide testing for causes of facial nerve weakness. It is not recommended that all patients be tested for Lyme disease, only those that have a history of tick bite or manifestations of rash and arthritis. Patients may be treated at home medically with close follow up to assure improvement of symptoms. There should be a consideration for timely specialty referral if there has been little improvement in the first few weeks of disease. There are no known preventative measures, and 8% to 12% of patients will have a recurrence.
Enhancing Healthcare Team Outcomes
BP is the most common cause of unilateral facial paralysis. While benign, the condition does have moderate morbidity and can lead to loss of vision. Thus, the disorder is best managed by an interprofessional team.
The cause of BP remains unknown, and its treatment remains controversial. While steroids and/or antiviral medications are often prescribed, there are no randomized clinical trials to determine which is better or effective. The problem is compounded by the fact that the majority of cases resolve spontaneously. However, in individuals with long-standing facial paralysis accompanied by poor speech, incomplete eyelid closure or poor aesthetics, treatment needs to be addressed by an interprofessional team. Because the disorder affects different organ systems, an interprofessional team of clinicians, nurses, and technologists have proven effective. The most important feature of the treatment is to be patient-focused rather than symptom focus.
In any case, all clinicians including the pharmacist and nurse practitioner must educate the patient on eye protection and lubrication. Eye dryness should be prevented at all costs using tears and other liquid preparations. If there is evidence of non-compliance or evidence that the eye is becoming dry and irritated, the nurse or pharmacist should report back to the clinical team leader.
The neurology nurse must educate the patient on facial exercises that can help improve muscle strength and facial coordination. These exercises can reduce poor aesthetics and improve the functionality of the facial muscles. If the patient is non-compliant, the nurse should report to the clinical team leader and assist with further education of the patient.
The availability of botulinum toxin has helped reduce the long-term burden of this disorder. Surgery is the last resort treatment and may be required in chronic cases. The facial muscles do remain viable for several years, and in these cases, complex reconstructions are available. However, rather than subjecting the patient to complex surgery with no guarantee of improvement, early recognition and initiation of steroidal therapy are recommended.[11] (Level lll) Close follow up with the interprofessional team is necessary to ensure that no complications occur.
Outcomes
Evidence-based medicine is lacking when it comes to treatment and outcomes for BP. The problem is made more difficult because many cases resolve spontaneously. The majority of outcomes have been from case reports or small case series. While recovery does occur in most patients, it often takes months or even years for a full recovery. Because there are several types of treatments available besides medications, an interprofessional team should be involved in the management since not everyone responds to the same treatment. [12](Level V)
(Click Image to Enlarge)
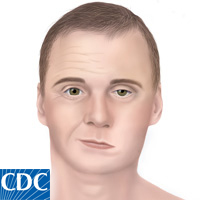
Bell's Palsy
Contributed by Centers for Disease Control and Prevention (NIH), PD US HHS CDC