Anatomy, Shoulder and Upper Limb, Biceps Muscle
- Article Author:
- Manpreet Tiwana
- Article Author:
- Matthew Charlick
- Article Editor:
- Matthew Varacallo
- Updated:
- 8/11/2020 8:21:02 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Biceps Muscle CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Biceps Muscle
Introduction
The biceps brachii is a large, thick muscle on the ventral portion of the upper arm. The muscle is composed of a short head (caput breve) and a long head (caput longum). The short head originates from the tip of the coracoid process, and the long head originates from the supraglenoid tubercle (tuberculum supraglenoidale) of the glenoid/scapula. Both heads course distally and become a confluent muscle belly before tapering across the anterior aspect of the elbow, eventually inserting on the radial tuberosity and the fascia of the forearm via the bicipital aponeurosis. [1][2] The antagonist of the biceps muscle is the triceps brachii muscle.[3][4][5]
Structure and Function
The long head of the biceps (LHB) brachii tendon originates at the supraglenoid tubercle and superior glenoid labrum. Its labral origin is mostly posterior in over half of cases, and the tendon, on average, is 9 cm in length. Inside the joint, the tendon is extrasynovial and passes obliquely heading toward the bicipital groove. As it exits the distal bicipital groove in the upper arm, the LHBT joins the short head of the biceps tendon (SHBT) as both transitions into their respective muscle bellies in the central third of the upper arm. After crossing the volar aspect of the elbow, the biceps brachii inserts on the radial tuberosity and medial forearm fascia. The latter occurs via the bicipital aponeurosis. [6]
The distal insertion point has become a relevant, yet controversial topic of interest. Over the last decade, there has been a renewed interest in investigating the insertional anatomy of the distal biceps tendon, specifically with respect to its relevance in the evolution of distal biceps reconstruction techniques. Historically, the insertion site was described as one homogenous tendon inserting on the radial tuberosity. More recent studies have reported its distal attachment as two distinct tendons. More specifically, recent studies have demonstrated the presence of an entirely bifurcated distal biceps tendon insertion. The studies found that the short head of the distal biceps tendon commonly inserts more distally than the long head and typically inserts at the apex of the tuberosity. The long head passes deep to the distal tendon of the short head before inserting proximal to the tendinous footprint of the short head. [7]
Biomechanics
The biceps brachii muscle primarily is a strong forearm supinator, but a weak elbow flexor. [8] Biomechanically, the LHBT has a controversial role in the dynamic stability of the shoulder joint. It has been demonstrated, mostly in biomechanical cadaveric-based studies and animal models, that the tendon at least plays a passive stabilizing role in the shoulder. Neer proposed in the 1970s that the LHBTs stabilizing role varied depending on the position of the elbow Several subsequent studies refuted the theory that the LHBT played any active shoulder stabilizing effect [9]. Jobe and Perry evaluated the activation of the biceps during the throwing motion in athletes. The authors reported the peak muscle stimulation occurred in relation to elbow flexion and forearm deceleration, with very little proximal biceps activity during the earlier phases of throwing. [10]
Pain generation
The LHBT is a well-recognized source of anterior shoulder pain. Mechanical causes include repetitive traction, friction, and glenohumeral rotation. The bicipital sheath itself is vulnerable to tenosynovial inflammation by association as it is contiguous with the synovial lining of the glenohumeral joint. The upper one-third of the LHBT demonstrates a rich sympathetic innervation network including neuropeptides such as substance P and Calcitonin gene-related peptide. These factors are present in the sensory nerves in this region of the tendon. This sympathetic network is known to exhibit vasodilatory changes as part of the neurogenic inflammatory process in the LHBT, which may play a critical role in at least the chronic phase of pathophysiology affecting the LHBT. [11][12]
Blood Supply and Lymphatics
The primary arterial blood supply for the biceps brachii muscle is via the muscular branches of the brachial artery.
Nerves
The nerve supply to the biceps is provided by the musculocutaneous nerve (root C5, C6).
Physiologic Variants
Approximately 30% of adults have some variation in the origin of the muscle. In many patients, a third head may arise from the humerus, but in about 2% to 5% of people, there may be supernumerary heads numbering anywhere from 3 to 7 in total.
The distal biceps tendon may be bifurcated in about 20% or be completely separated in about 40% of individuals. These variations have no adverse effect on arm function.[13]
Surgical Considerations
Proximal biceps (LHBT) surgical considerations:
In the setting of advanced tendinopathy affecting the LHBT, and in the setting of persistent, debilitating symptoms despite exhausting all nonoperative treatment options, two common procedures can be performed.
Biceps tenotomy [14]
Arthroscopic inspection of the tendon allows for estimation of the relative percentage of the LHB tendon that is compromised. A popular classification system utilized for the intra-operative grade corresponding to degree of LHB tendon macroscopic pathology is the Lafosse grading scale: [15]
- Grade 0: Normal tendon
- Grade 1: Minor lesion (partial, localized areas of tendon erosion/fraying, focal areas affect <50% of the tendon width)
- Grade 2: Major lesion (extensive tendon loss, compromising >50% of the tendon width)
Some surgeons solely debride the tendon in the setting of <25%-50% tendinous compromise. Arthroscopic biceps tenotomy is performed by releasing the tendon as close as possible to the superior labrum. As long as the tendon is free from intimate soft tissue adhesions to surrounding structures, the tendon should retract distally toward the bicipital groove. If adhesions are present, all efforts should be made to mobilize the tendon in order to allow for retraction following the tenotomy. In cases where the LHB tendon is particularly hypertrophic and scarred to other soft tissue structures in the joint, this serves as a potential source of postoperative pain.
Biceps tenodesis [16]
- Recommended over tenotomy in the setting of LHBT instability
- Preferred technique in younger patients, athletes, laborers, and those patients specifically concerned with postoperative cosmetic (“popeye”) deformity
- Optimizes the length-tension relationship of the biceps muscle; mitigates postoperative risk of muscle atrophy, fatigue, and cramping
Clinical Significance
The initial management for pathologic conditions affecting the biceps brachii tendon (both proximal and distal) is often nonoperative management modalities. Conditions affecting the distal biceps brachii tendon is beyond the scope of this review. Proximally, shoulder range of motion, rotator cuff srengthening and periscapular stabilization parameters focus on restoring muscle balance across the shoulder girdle.
For conditions affecting the LHBT proximally, the following physical therapy regimens can be considered:
- Proximal biceps stretching/strengthening exercises
- NSAIDs
- Iontophoresis (e.g. dexamethasone)
Focused stretching on the anterior shoulder structures, including pectoralis minor, should also be considered. Other modalities such as dry needling have demonstrated promise in preliminary animal studies.
In refractory conditions, or conditions beyond the scope of this review, surgical consideration is warranted.
(Click Image to Enlarge)

Front of right upper extremity Anatomy, Flexor Carpal Radius, Abductor and Exterior Pollicis Longus and Brevis, Palmaris Longus, Medial group of Antebrachial muscles, Antecubital fossa, Lateral group of Antebrachial muscles, Brachialis, Biceps brachii, Triceps brachii, Medial epicondyle
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
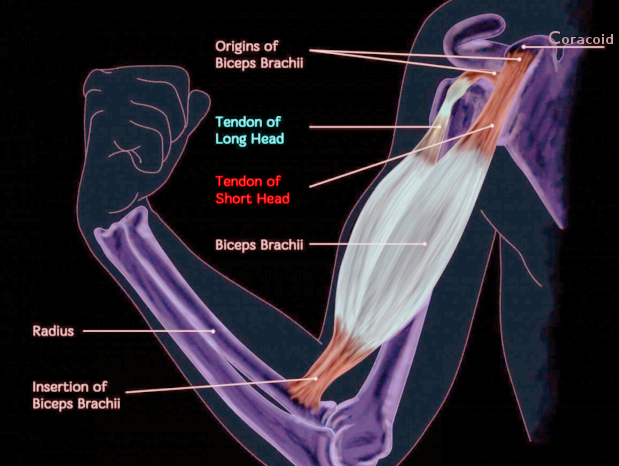
Biceps anatomy
Image courtesy O. Chaigasame