Lower Lid Transconjunctival Blepharoplasty
- Article Author:
- Blake Raggio
- Article Editor:
- Ryan Winters
- Updated:
- 7/31/2020 3:19:13 PM
- For CME on this topic:
- Lower Lid Transconjunctival Blepharoplasty CME
- PubMed Link:
- Lower Lid Transconjunctival Blepharoplasty
Introduction
The goals of lower eyelid blepharoplasty are to correct the characteristic signs of aging that occur in the periorbital region, including excess eyelid skin, lid laxity, and orbital fat malposition. In general, two basic blepharoplasty approaches exist—the transcutaneous and transconjunctival approaches.[1] This activity discusses the nuances of the transconjunctival lower lid blepharoplasty approach, an effective and reliable technique ideal for patients with pseudoherniated orbital fat and good skin elasticity.[2] The modern-day aesthetic surgeon must understand the indications, preoperative considerations, operative techniques, and complications associated with transconjunctival lower lid blepharoplasty to maximize outcomes and improve patient satisfaction.[3]
Anatomy and Physiology
- Lower eyelid margin: this should rest at the inferior limbus with no scleral show and its lowest point slightly lateral to the pupil.
- Lower eyelid crease: should rest 2 mm below the lash line medially and 5 mm below the lash line laterally.
- Lamellae of the lower eyelid: anterior lamella (skin and orbicularis oculi muscle), middle lamella (orbital septum and tarsal plate), posterior lamella (lower eyelid retractors and palpebral conjunctiva).
- Lower eyelid retractors: consists of the capsulopalpebral fascia (web-like band of connective tissue which transmits forces from the inferior rectus to the lower lid) and the inferior tarsal muscle, both of which insert onto the tarsal plate.
- Post-septal infraorbital fat pads: there are small medial (nasal), large central, and small lateral (temporal). The fat in the medial compartment is classically lighter in color and denser than the fat of the other compartments. The clinician can best visualize the infraorbital fat pads with the patient looking upwards.
- Inferior oblique muscle: this muscle separates the medial and central fat pads of the lower lid.
- Arcuate expansion: separates the lateral and central fat pads of the lower lid.
- Sub-orbicularis oculi fat (SOOF): a supraperiosteal submuscular fat excess located below the lateral half of the infraorbital rim.
- Orbicularis oculi muscle: this muscle has a pretarsal component (approximately 4 mm) and pre-septal component (from the inferior border of the tarsus to the arcus marginalis or orbital rim). Medially, the orbicularis attaches just below the orbital rim without an intervening ligamentous structure, which contributes to the formation of the nasojugal groove (tear trough). The lateral orbicularis is secured to the bone via the orbital retaining ligament. The orbital portion of the orbicularis oculi muscle extends inferiorly from the arcus marginalis and overlies the upper maxilla.
Characteristic signs of aging to the lower eyelid and midface[8][9][10]:
- Dermatochalasis: excess lower lid skin.
- Steatoblepharon (pseudoherniated orbital fat): occurs secondary to globe descent within the orbit, weakening of the orbital septum, and attenuation of the orbicularis oculi muscle.
- Double-convex pattern of the eyelid-cheek transition: this is caused by fat herniation above the orbital rim (the first convexity), hollowing over the infraorbital rim (nasojugal groove or tear trough), and ptotic cheek tissue inferiorly (the second convexity).
- Negative vector: describes a posterior displacement of the orbital rim relative to the lower lid.
- Lid laxity: can be identified using 1) the snap test, where the lower lid is pulled inferiorly and observed to see how quickly it returns to its original position (should occur immediately) and 2) the distraction test, where the lower lid gets pulled from the globe, and the distance is measured (greater than 6 mm is abnormal). Note: Patients with lower lid laxity are prone to develop lower lid malposition post-operatively.
- Malar bags (festoons): hammocks of lax skin and orbicularis muscle that appear as bag-like structures, typically rest below the orbital rim
Indications
The transconjunctival lower lid blepharoplasty approach is best suited for the patient with steatoblepharon with minimal to moderate lower eyelid laxity. Fat repositioning can also address a prominent tear trough deformity. While modern-day periorbital rejuvenation principles emphasize orbital fat preservation during blepharoplasty (with either fat repositioning or augmentation); nevertheless, fat resection may be suitable for patients with steatoblepharon and no tear trough deformity.[11][12]
Other indications for a transconjunctival approach include patients with a history of hypertrophic scarring, history of blepharoplasty, or a pre-existing pseudoproptosis (at risk for lower eyelid retraction and further scleral show).[13]
Contraindications
Contraindications for performing a transconjunctival approach include[14][15][16]:
- Active blepharitis
- Unrecognized dry eye syndrome or orbitopathy: warrants referral to an ophthalmologist
- History of refractive procedures (such as laser epithelial keratomileusis or photorefractive keratectomy): surgery should be delayed at least 6 months after refractive surgery
- Smoking: may predispose patients to tear film abnormalities and subsequent ocular surface disease
- Anticoagulants: should be withheld for at least 2 weeks prior to surgery
- Niacin, echinacea, and kava: may predispose the patient to ocular surface disease
Equipment
Preoperatively
- Surgical marker
- Local anesthesia, such as 1% lidocaine with epinephrine 1 to 100000
- Topical antiseptic, such as povidone-iodine paint (diluted to a concentration suitable for ophthalmic exposure)
- Corneal shield (optional) and lubrication to protect the eyes
- If under local anesthesia, instill 0.5% topical tetracaine hydrochloride ophthalmic drops before placement of protective corneal shields
Intraoperatively
- Small retractors (Desmarres)
- Fine-tip cautery device
- Fine tissue forceps (Bishop)
- Small dissecting scissors (Westcott)
- Cotton-tip applicators
- Elevators (Freer or Cottle)
- Suture (5-0 nylon or prolene, 5-0 vicryl, and 6-0 fast absorbable gut sutures)
- Bolster
Postoperatively
- Ophthalmic antibiotic ointment
- Ice packs
Personnel
- Anesthesiologist
- Scrub technician
- Operative Nurse
- Surgical assistant: to help retract, manage intraoperative bleeding, and cut suture
Preparation
Photographic views should be obtained using a 5-view head series with the patient in a seated and upright position with no facial animation. There should be documentation with close-up views of the eyes (closed/open/upward gaze/lateral gaze).[17]
The infraorbital fat pads, tear trough, and site of the infraorbital nerve are marked. If a performing a concomitant skin pinch, this can be marked out with a conservative (2 to 3 mm) skin pinch along the subciliary margin.
Although the transconjunctival blepharoplasty may be performed entirely under local anesthesia, nevertheless general anesthesia or intravenous (IV) techniques are advisable to ensure patient comfort.
A single dose of intravenous antibiotics should be administered before the start of the procedure.
Local anesthesia should infiltrate along the inferior orbital rim, tear trough, and conjunctiva.
Eye shields can are an option per surgeon preference.
Technique
Herein, we describe the principle techniques required to perform a safe and reproducible transconjunctival lower lid blepharoplasty with fat transposition.[18][1][19][20]
First, the surgeon incises the lower conjunctiva. If a pre-septal approach is utilized, the conjunctival incision is made 4 mm inferior to the tarsus with dissection proceeding anterior to the septum. Alternatively, a post-septal approach requires an incision made 6 to 7.5 mm inferior to the tarsus, with dissection following posterior to the orbital septum (middle lamella). Although the theoretical benefit to the post-septal approach is the preservation of the orbital septum, either approach may be used as they both posess similar risk profiles.[21]
In order to protect the cornea and maximize exposure of the fat pads, the posterior conjunctival flap is secured cephalad with a traction suture, while the anterior edge of the divided conjunctiva is retracted caudally using a small retractor.
Before dissecting the orbital fat, a subperiosteal pocket for fat transposition is created by making a periosteal incision through the arcus marginalis just below the inferior orbital. An elevator is used to raise the periosteum over the upper maxilla for approximately 15 mm, with care not to injure the infraorbital nerve. Depending on the extent of fat repositioning, dissection may be carried laterally to release the orbital retaining ligament. As an alternative to the subperiosteal technique, a supraperiosteal pocket may be used for fat repositioning; both have similar clinical outcomes and high patient satisfaction.[22]
The orbital fat is then dissected. If a pre-septal approach was used, the inferior edge of the septum is incised to expose the medial and central fat pads. The extruded fat is then carefully dissected and made into a pedicle with care to prevent devascularization and to avoid injury to the inferior oblique muscle.
Transposition of the orbital fat into the subperiosteal or subperiosteal pocket is done with a series of transcutaneous horizontal mattress retention sutures placed beyond the marked tear trough. The suture is then secured using a bolster or fixed in place using adhesive tape.
The conjunctival incision may be left to heal secondarily or closed loosely with buried 6-0 fast-absorbable gut sutures.
Secondary procedures to maximize results:[23][1][24]
- Skin pinch: to correct excess lower eyelid skin (dermatochalasis), performed via a subciliary incision extended out to the crow’s feet crease
- Suture canthopexy: to correct and/or prevent minimal (1 to 2 mm) lower lid laxity, a stitch capturing the periosteum of the inside orbital rim is placed with a vector posterior, superior, and lateral to shorten and tighten the lower lid.
- Malar/cheek lateral suspension: depending on the etiology and severity of the problem, multiple methods can be used to efface the transition from lid to cheek. These include 1) the suspension of the preseptal orbicularis, 2) the SOOF lift, and 3) the subperiosteal midface lift.[19]
- Skin resurfacing (chemical peels or lasers): improves crepey (thin and wrinkled) skin appearance and dark pigmentation of the lower lid.
- Botulinum toxin injection: treats the crow’s feet area.
- Facial fillers and autologous fat-grafting techniques: supplement mid-face volume and further camouflage tear trough.[25]
Complications
A major advantage of the transconjunctival approach compared to the transcutaneous approach is the decreased incidence of complications, namely lid malposition, and external scarring. Nevertheless, the blepharoplasty surgeon must possess a thorough knowledge of the potential complications of the transconjunctival lower lid approach.[26][27][28]
Early
- Corneal abrasions: may be prevented with the use of corneal shields and intentionally not to passing instruments directly over the eyes.
- Orbital hemorrhage: a rare but potentially sight-threatening complication, requiring emergent identification and intervention with lateral canthal release and/or medications (i.e., mannitol, steroids).
- Infections: should be promptly treated with topical and/or systemic antibiotics.
Intermediate
- Eyelid malposition:
- Lower lid retraction – a common complication caused by damage to the anterior and/or middle lamella which can be initially managed conservatively with lid massage and upward taping but may require surgical revision if persistent at three months.
- Lagophthalmos – a result of zygomatic nerve injury leading to reduced orbicularis tone and subsequent exposure keratopathy; initial treatment involves aggressive lubrication, though persistence may be correctable with lateral canthal repositioning.
- Ectropion – results from vertical lid shortening of the anterior lamella, may be avoided with routine use of lateral canthopexy to support the lower lid position in cases of increasing vertical tension.
- Strabismus: most commonly due to inferior oblique muscle injury and can usually be managed conservatively.
- Corneal exposure: can be avoided with frequent eye lubrication.
- Epiphora
Late
- Changes in eyelid height and contour: caused mainly by anterior and middle lamellar changes.
- Hypertrophic scarring: may be present when performing concomitant skin pinch.
- Dermal pigmentation
Clinical Significance
A transconjunctival lower lid blepharoplasty aims to restore a more youthful and rested appearance to the periorbita with removal or relocation of pseudoherniated fat. When performing a transconjunctival blepharoplasty, proper patient evaluation, and development of a thorough, anatomic-based treatment plan can produce safe, reliable, and satisfactory outcomes.
Enhancing Healthcare Team Outcomes
It remains imperative to identify the risk factors and perform a thorough assessment of the patient before transconjunctival blepharoplasty. A team approach is an ideal way to limit the complications of this procedure. Before surgery, the patient should have the following done:
- Evaluation by a surgeon experienced in selecting the appropriate patient for the surgery
- Evaluation by their primary care physician, anesthesiologist, and nurse anesthetist to ensure that the patient is fit for anesthesia
- Evaluation by the optometrist or ophthalmologist if the patient suffers from dry eye, ptosis, or lagophthalmos
- Evaluation and monitoring by the pre-operative, operative, and post-operative specialty trained nurses assisting with patient and family education as well as coordination of care.
an interprofessional team of an experienced surgeon, anesthesiologist, and surgical assistants and operative nurses should perform the transconjunctival blepharoplasty for the best outcomes. Close follow-up during the initial post-operative period, either by a wound care nurse and/or clinician experienced in the post-operative care of transconjunctival blepharoplasty should monitor the patient for possible complications, including any visual deficits. It is also critical to counsel the patient on avoiding strenuous activity, heavy lifting, or bending over during the first several days post-operatively to prevent such complications. This type of interprofessional team approach will lead to optimal patient outcomes in transconjunctival blepharoplasty cases. [Level 5]
Nursing, Allied Health, and Interprofessional Team Interventions
Adequate pain medication is given, as patients often report mild peri-incisional pain for 1-2 days post-operatively. In order to minimize edema and ecchymosis, the patient should place ice packs around the eyes intermittently for the first 24 hours, sleep with the head elevated for 1 week, and avoid rigorous activity for 2 weeks. A low dose corticosteroid taper may help lessen bruising and swelling as well. Patients are asked to return at 1 week for wound assessment with or without suture removal. Photographic documentation should occur at around 6 months postoperatively.
Nursing, Allied Health, and Interprofessional Team Monitoring
Close follow-up during the initial post-operative period, either by a wound care nurse and/or clinician experienced in the post-operative care of transconjunctival blepharoplasty, should monitor the patient for possible complications including acute visual disturbances.
(Click Image to Enlarge)
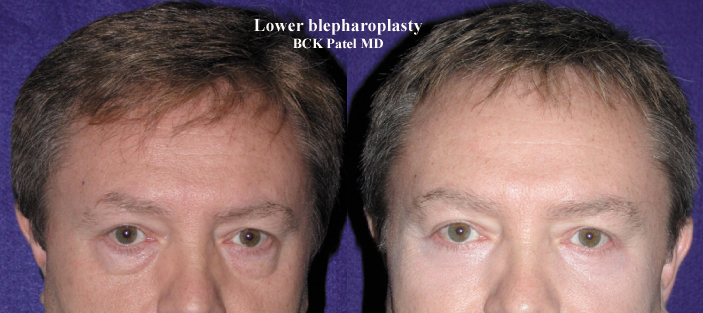
Before and after photographs of lower trans conjunctival blepharoplasty with lateral canthal tightening and CO2 laser application to the skin, together with fat transposition over the inferior orbital rim.
Contributed by Prof. Bhupendra C.K. Patel MD, FRCS
(Click Image to Enlarge)
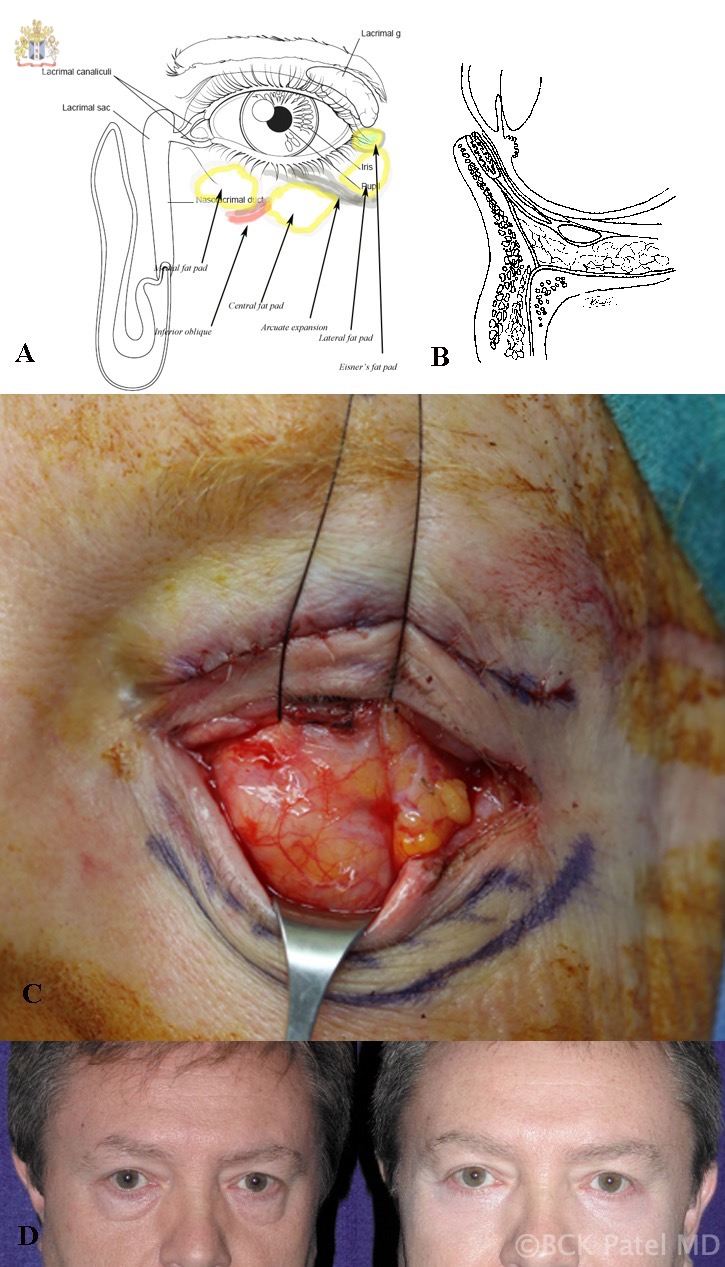
A: Surface anatomy of the left lower eyelid fat pads. B: Cross-sectional anatomy showing the septum and post-septal fat and lower eyelid retractors. C: Traction sutures through the lower eyelid retractors (left eye) showing the medial and central fat pads often appearing as one and the lateral fat pad. D: Before-and-after photographs of transconjunctival lower blepharoplasty in a male.
Contributed by Professor Bhupendra C. K. Patel MD, FRCS