Brachial Plexus Block Techniques
- Article Author:
- John Pester
- Article Editor:
- Matthew Varacallo
- Updated:
- 4/26/2020 9:52:26 AM
- For CME on this topic:
- Brachial Plexus Block Techniques CME
- PubMed Link:
- Brachial Plexus Block Techniques
Introduction
Blockade of the brachial plexus is an effective method for providing anesthesia to the upper limb from the shoulder to the fingertips. There are multiple approaches to blocking the brachial plexus which are dependent on the block indication, surgery or procedure being performed, patient-specific body habitus, medical comorbidities, and individual anatomy variations. This review will address the indications, probe placement, and sonoanatomy for ultrasound-guided interscalene block, superior trunk block, supraclavicular brachial plexus block, infraclavicular brachial plexus block, and axillary brachial plexus block.[1][2]
Anatomy and Physiology
The brachial plexus is formed from the C5 to T1 nerve roots. These roots join to form the superior (C5, C6), middle (C7), and inferior trunks (C8, T1) above the clavicle. As the trunks pass under the clavicle, they are found in proximity to each other and can be blocked easily at this level. Distal to the clavicle, the plexus splits into the lateral (C5-C7), posterior (C5-T1), and medial (C8, T1) cords which are found situated adjacent to the axillary artery. Finally, the terminal nerve branches are formed from the cords in the axilla. The median nerve is formed from the medial and lateral cords and usually is located superficial to the axillary artery. The ulnar nerve is formed from the medial cord and usually is located lateral to the axillary artery. The radial nerve is located deep and lateral to the axillary artery. The last terminal branch, the musculocutaneous nerve, branches off from the lateral cord and pierces through the coracobrachialis in the proximal axilla.
The brachial plexus can be blocked at multiple sites for varying effect. It is useful to be familiar with multiple approaches given variant patient anatomy and indications.
Indications
Interscalene brachial plexus block: provides analgesia or surgical anesthesia to the from the distal extent of the clavicle, shoulder joint, and proximal humerus
Superior trunk block: provides analgesia to the shoulder capsule and proximal humerus. This is a potentially diaphragm-sparing modification of the interscalene block. [3]
Supraclavicular brachial plexus block: analgesia or surgical anesthesia of the upper limb from the mid-humerus to the fingertips.
Infraclavicular brachial plexus block: analgesia or surgical anesthesia of the upper limb from the mid-humerus to the fingertips. This block typically spares the intercostobrachial nerve. This block can be performed in a traditional approach with a steep needle angle or with the retroclavicular approach (RAPTIR) [4]
Axillary brachial plexus block: analgesia or surgical anesthesia of the upper limb from mid humerus to the fingertips. This block also spares the intercostobrachial nerve, although it is blocked easily within the same window.[5][3][6]
Contraindications
Interscalene brachial plexus block: pulmonary disease, heart disease, cellulitis/abscess over the site of injection, patient refusal, allergy to the local anesthetic. Morbid obesity may be a relative contraindication as respiratory insufficiency can result in hemidiaphragmatic paralysis.
Superior trunk block: same as ISB, although phrenic nerve palsy is felt to occur less frequently. Be aware that the dorsal scapular nerve typically travels through the middle scalene near the typical site of injection.
Supraclavicular brachial plexus block: cellulitis/abscess over the site of injection. Use caution in patients with poor pulmonary reserve, as a resultant pneumothorax may significantly worsen their respiratory status (example: known pneumonia on the contralateral side).
Infraclavicular brachial plexus block: cellulitis/abscess over the site of injection.
Axillary brachial plexus block: cellulitis/abscess over the site of injection, inability to visualize a clear needle path through the highly vascular region.
Equipment
The same equipment is needed for all the listed approaches to brachial plexus block:
- High frequency (more than 10 MHz) linear ultrasound probe
- Chlorhexidine 2% or povidone iodine skin disinfectant solution
- Local anesthetic; for longer duration blocks bupivacaine 0.5% or ropivacaine 0.5%, for shorter blocks lidocaine 2% or mepivacaine 1.5%
- A 10 mL to 20 mL syringe with extension tubing
- Short bevel block needle (10 cm, 22-18 gauge)
- Sterile ultrasound probe cover
- Sterile ultrasound gel
- Standard vitals monitoring equipment (NIBP, rhythm monitoring, +/- pulse oximetry)
Personnel
Provider trained in ultrasound-guided regional anesthesia. Additional personnel (nurse, another provider) to actively monitor patient vitals and give rescue medications if needed.
Preparation
Prior to performing any of the aforementioned blocks, the patient is provided a description of the risks, benefits, and alternatives to the procedure. Informed consent is obtained from the patient. The skin of the site should be cleansed with chlorhexidine 2% or povidone iodine and allowed to dry. The sterile gel should be applied to the probe; then a sterile probe cover should be placed with additional sterile gel on the exterior surface of the probe cover. Draw up the desired volume of local anesthetic into a syringe, then connect extension tubing with a short bevel block needle attached. Prime the tubing and needle by ejecting all of the air from the system, an injection of air into the site will inhibit insonation.
Interscalene, superior trunk, supraclavicular, and infraclavicular (retrograde/RAPTIR) approaches: the patient should be placed supine with the head and neck rotated slightly toward the contralateral side. A towel roll may be used under the ipsilateral shoulder if needed, to allow more room for needle manipulation. The ipsilateral arm should be adducted.
Infraclavicular (classic/anterior) and axillary approaches: the patient should be supine with the head and neck rotated slightly toward the contralateral side. The ipsilateral shoulder may be abducted to 90 degrees with the elbow flexed to increase visualization of the axillary artery and facilitate needle passage.
Technique
Interscalene brachial plexus block:
- Place the ultrasound probe in the supraclavicular fossa in a transverse orientation, aimed caudad into the thoracic cavity, to visualize the brachial plexus near the subclavian artery. Once identified, follow the plexus cephalad where it is found in the interscalene groove.
- At the interscalene groove, the plexus is typically seen as multiple anechoic circular structures that have a "stoplight" appearance. Typically, the topmost structure is C5 while the middle and lower structures are both C6 as it divides.
- Use color doppler to identify any vascular structures which may be in the needle path.
- Insert a block needle in-plane from posterior to anterior and lateral to medial toward the interscalene groove. Be cautious not to advance the needle between any of the hypoechoic nerve roots.
- Once the needle tip is in the groove, confirm it is not intravascular by negative aspiration.
- Inject 1 mL to 2 mL of local anesthetic to verify tip placement and spread of local anesthetic into the interscalene groove, causing spread around the nerve roots.
- Once placement is confirmed, repeat incremental injection and negative aspiration until an adequate spread of local anesthetic has occurred. Typically this is between 10 mL to 30mL.
Superior trunk block:
- Place the ultrasound probe in the supraclavicular fossa in a transverse orientation, aimed caudad into the thoracic cavity, to visualize the brachial plexus near the subclavian artery. Once identified, follow the plexus cephalad where it is found in the interscalene groove.
- Scan caudad, following the C5 and C6 roots to where they appear joined as the superior trunk. Ideally, this location should be proximal to where the suprascapular nerve branches.
- Identify the dorsal scapular nerve as it courses through the middle scalene muscle, to avoid it during needle passage.
- Use color doppler to identify any vascular structures which may be in the needle path.
- Insert a block needle in-plane from posterior to anterior and lateral to medial toward the superior trunk.
- Once the needle tip is just deep to the superior trunk, confirm it is not intravascular by negative aspiration.
- Inject 1 mL to 2 mL of local anesthetic to verify tip placement and spread of local anesthetic adjacent to the superior trunk.
- Once placement is confirmed, repeat incremental injection and negative aspiration until an adequate spread of local anesthetic has occurred. Typically this is about 10 mL.
Supraclavicular brachial plexus block:
- Place the ultrasound probe in the supraclavicular fossa in a transverse orientation, aimed caudad into the thoracic cavity, to visualize the brachial plexus near the subclavian artery.
- Visualize the interface between the visceral and parietal pleura which is seen as "lung sliding" on ultrasound. Additionally, visualize the first rib as a hyperechoic line with dropout artifact deep to it. Ideally, the plexus and subclavian artery should be visualized overlying the first rib. This allows the first rib to be used as a bony backstop, decreasing the risk of pneumothorax. Rotating the lateral edge of the probe more posterior may aid in obtaining this window.
- Insert a block needle in-plane from posterior to anterior and lateral to medial aiming for the deep portion of the brachial plexus where it overlies the first rib.
- Confirm negative aspiration then inject a small amount of local anesthetic with the goal of raising the plexus off of the first rib.
- Advance the needle along the first rib to the anterior aspect of the plexus, adjacent to the subclavian artery. This is called the "corner pocket." It is important to cover this area for a successful block completely.
- Confirm negative aspiration then inject another 1 mL to 2 mL of local anesthetic in this area. Repeat until a total of about 10 mL has been injected deep into the plexus.
- Retract the needle to the skin then re-advance at a shallow angle, guiding the needle to the superficial aspect of the brachial plexus.
- Confirm negative aspiration then inject 1 mL to 2 mL of local anesthetic superficial to the plexus. Repeat until a total of about 10mL has been injected superficial to the plexus.
Infraclavicular brachial plexus block (classic/anterior approach):
- Place the ultrasound probe in the deltopectoral groove with the probe marker facing cephalad. The probe should be just caudad to the clavicle.
- Identify the axillary artery and vein deep to the pectoralis major and pectoralis minor muscles. The vein is usually found lateral to the artery and is compressible and non-pulsatile. Doppler may be used to aid in identification.
- Using color Doppler, identify the thoracoacromial artery and cephalic vein as these may be within the needle path.
- At this level, the brachial plexus has split into the lateral, posterior and medial cords which are typically found at 9, 6, and 3 o'clock respectively. However, they are not always visible and do not need to be visualized for a successful block.
- Insert a block needle in-plane from cephalad to caudad and medial to lateral, starting just caudad to the clavicle aiming for the lateral aspect of the axillary artery. The needle trajectory is often quite steep, which may limit needle visualization.
- Aim the needle toward the 6 o'clock position deep to the axillary artery.
- Confirm negative aspiration then inject 1 mL to 2 mL of local anesthetic to visualize the spread of local anesthetic deep into the artery.
- Repeat step six until the adequate spread of local anesthetic has been achieved. This is visualized as a 'U'-shaped spread of anesthetic along the lateral, posterior, and medial aspects of the axillary artery. Typically, 20 mL to 30 mL is required.
Infraclavicular brachial plexus block (retrograde approach):
- Proceed with steps one to three as above.
- Starting just cephalad and posterior to the clavicle, insert a block needle in-plane from medial to lateral with the needle trajectory parallel to the ultrasound probe. Having the superior edge of the ultrasound probe slightly overlying the clavicle may help in orientation and needle guidance.
- The needle should be visualized passing under the clavicle and parallel to the probe. Aim toward the 6 o'clock position deep to the axillary artery.
- Confirm negative aspiration then inject 1 mL to 2 mL of local anesthetic to visualize the spread of local anesthetic deep into the artery.
- Repeat step 4 until the adequate spread of local anesthetic has been achieved. This is visualized as a 'U'-shaped spread of anesthetic along the lateral, posterior, and medial aspects of the axillary artery. Typically, 20 mL to 30 mL is required.
Axillary brachial plexus block:
- Place the ultrasound probe in a transverse orientation in the axilla at the site where pectoralis major inserts onto the humerus.
- Scan distally and proximally to visualize the axillary artery, vein, and nerves surrounding the artery.
- The ideal ultrasound window should have the following structures: (1) musculocutaneous nerve seen piercing coracobrachialis and (2) teres major fascia/tendon insertion onto the humerus seen deep in the axillary artery.
- Color Doppler should be used to identify vasculature, as this is a highly vascular area.
- Insert a block needle in-plane from anterior to posterior, parallel to the ultrasound probe.
- Advance toward the musculocutaneous nerve (MCN).
- Confirm negative aspiration then inject 1 mL to 2 mL aliquots until adequate spread around the MCN is achieved.
- Retract and redirect needle deep into the axillary artery.
- Confirm negative aspiration then inject 1 mL to 2 mL aliquots until adequate spread around the posterior aspect of the axillary artery is achieved.
- If spread around the artery is inadequate, advance the needle under the artery toward the medial aspect and repeat step 9.
- Retract and redirect needle superficial to the axillary artery.
- Repeat step nine to ensure the circumferential spread of local anesthetic.
- Optional step to block the intercostobrachial nerve: retract the needle to the skin and readvance between the skin and the muscle/fascia layer superficial to the axillary artery and plexus.
Complications
All blocks are at risk for nerve injury (neuropraxia, neurotmesis) due to multiple factors including inadvertent intraneural injection, local anesthetic neurotoxic properties, hematoma formation, physical damage from block needle. Local anesthetic systemic toxicity should also be considered as a complication for all blocks. Before placing a block, ensure that the total dose of local anesthetic to be injected is less than the theoretical toxic dose for the anesthetic being used. Listed below are complications unique to each approach for brachial plexus blockade.[7][8]
Interscalene brachial plexus block: ipsilateral phrenic nerve palsy resulting in hemidiaphragmatic paralysis, vascular injury including vertebral artery puncture, Horner syndrome, subdural block, injury to brachial plexus.
Superior trunk block: ipsilateral phrenic nerve palsy (possibly lower incidence compared to ISB), vascular injury, injury to brachial plexus, injury to the dorsal scapular nerve as it typically courses through the middle scalene where the superior trunk is inserted.
Supraclavicular brachial plexus block: pneumothorax and subclavian arterial puncture are the major risks. There is still a risk of causing ipsilateral hemidiaphragmatic paralysis with this block, although the risk is much lower than ISB. Ulnar nerve sparing may occur if the full spread of anesthetic is not achieved between the first rib and the plexus.
Infraclavicular brachial plexus block: injury to brachial plexus, specifically the lateral and posterior cords, injury to axillary artery and/or vein. Sparing of the medial cord may occur with the inadequate spread of local anesthetic around the axillary artery. Using the classic/anterior approach, the thoracoacromial artery and cephalic vein may lie in the needle path.
Axillary brachial plexus block: there is virtually no risk of causing a pneumothorax with this approach. The use of color doppler is recommended to avoid inadvertent vascular puncture and injection (LAST).
Clinical Significance
Ultrasound-guided brachial plexus block can provide dense analgesia and anesthesia to the upper extremity from the shoulder to the fingers depending on the indication and approach utilized. The use of ultrasound has made these blocks more accessible and safer to perform. There is evidence to suggest that the use of ultrasound reduces the total volume of anesthetic required, decreases complications such as pneumothorax and vascular injury, and increases block success. Interscalene brachial plexus blockade can be used for acute pain management in fractures of the proximal humerus and clavicle, as well as in managing glenohumeral dislocations. It is effective in post-op pain control and reducing opiate use in patients recovering from shoulder surgeries, and has been used as the sole anesthetic in shoulder arthroscopy.
When performing an interscalene block for analgesia to the shoulder, there is a high risk for causing ipsilateral hemidiaphragmatic paralysis via phrenic nerve palsy. If this is a concern, other approaches should be considered, such as a superior trunk block or a combined suprascapular and axillary nerve block (CSANB). The superior trunk block potentially is diaphragm sparing, but further research is needed to determine efficacy. [3] There are multiple approaches to block the brachial plexus distal to the interscalene groove, all of which result in anesthesia to the entire upper extremity from the mid humerus to the fingertips. Which approach is utilized depends on many factors including the ability to position the patient appropriately, infection over the intended injection site, coagulopathy (compressible site may be preferred), operator experience, and variation in adjacent structures.
Enhancing Healthcare Team Outcomes
Knowing how to perform a brachial plexus block is very useful as it allows the surgeon to perform a range of procedures on the ipsilateral arm. While a brachial plexus block is usually performed by an anesthesiologist, the role of the nurse is vital. During the block, a nurse must be dedicated to observing the patient's vital signs for any changes. In addition, the nurse must frequently listen to the lung sounds to ensure that air entry is bilateral and equal- the procedure can be associated with a pneumothorax. [9] After the procedure, a portable x-ray is recommended to ensure that there is no pneumothorax, and the diaphragm is not elevated (the procedure can injure the phrenic nerve). [10] Adept anesthesia providers can confirm the presence or absence of a pneumothorax and elevated diaphragm in real-time via ultrasound, which is both sensitive and specific and avoids delays in diagnosis. [11]
(Click Image to Enlarge)
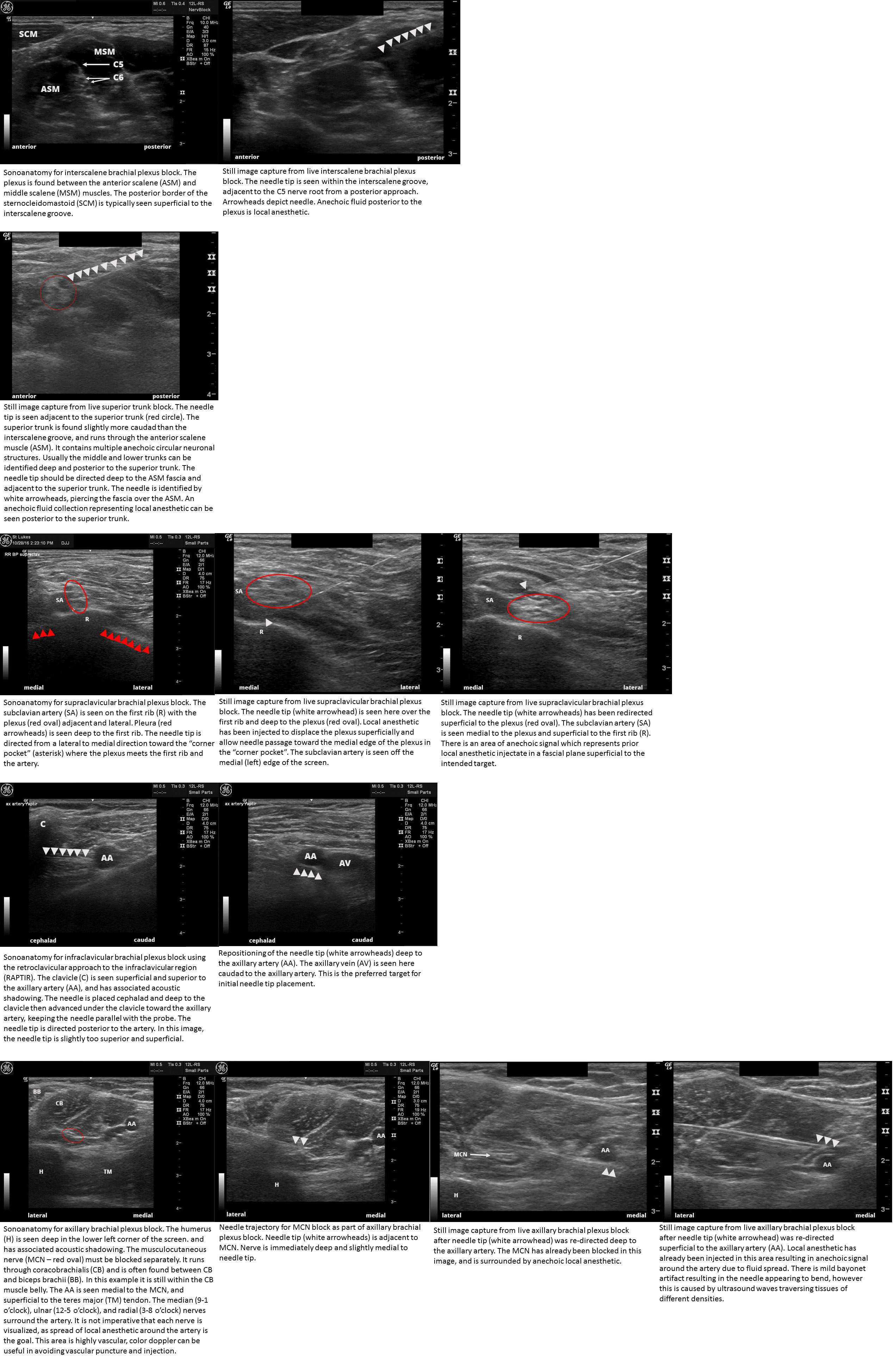
Sonoanatomy and needle placement for ultrasound guided brachial plexus blocks Includes interscalene brachial plexus block, superior trunk block, supraclavicular brachial plexus block, infraclavicular brachial plexus block (retroclavicular approach - RAPTIR), and axillary brachial plexus blocks
Contributed by John Pester, DO