Anatomy, Head and Neck, Buccinator Muscle
- Article Author:
- Manu Rathee
- Article Editor:
- Prachi Jain
- Updated:
- 8/23/2020 8:02:13 PM
- For CME on this topic:
- Anatomy, Head and Neck, Buccinator Muscle CME
- PubMed Link:
- Anatomy, Head and Neck, Buccinator Muscle
Introduction
The Buccinator muscle is a bilateral square-shaped muscle constituting the mobile as well as the adaptable cheek area.[1] Couper and Myot coined the term buccinator in the year 1694.[2] This muscle is sometimes referred to as an accessory muscle of mastication due to its role in compressing the cheeks inwards against molars, thus, aiding in chewing and swallowing.[3] Due to its function of puffing out cheeks, it is also called “trumpeter muscle.” It lies deep to the skin. Superficial to this muscle lies the anterior border of the masseter muscle and more superficial facial muscles.[4] One of the first muscle in an infant to get activated during sucking is buccinator.
Structure and Function
The buccinator muscle plays an active role along with orbicularis oris and superior constrictor muscle during swallowing, mastication, blowing, and sucking. It aids in mastication and blowing by compressing the cheek inwards. There are theories that the muscle thickens the cheek mucosa acting as a muscular hydrostat.[5] Due to this thickening, the cheek pushes a food bolus towards the tongue.[5]
Its contraction also pulls the corner of the mouth laterally. While closing the mouth, the muscle contracts gradually and during the opening movement, it relaxes; this maintains the required tension of the cheeks, thereby preventing injury of the buccal mucosa.[2][3]
It also helps in retention and stabilization of the complete denture. Research also shows it to play a role in patients with a habit of thumb/finger sucking.[6]
There are different phases of swallowing. Buccinator tends to act during two of the phases of swallowing. i.e. oral and pharyngeal phase. Buccinator, along with the orbicularis oris muscle begins the swallowing movement in the oral phase by generating a peristaltic wave-like contraction.[7] This wave passes through the pharynx. The wave gets initiated by buccinator muscle and is followed by the orbicularis oris muscle quickly.[7]
Apart from this, buccinator muscle gets activated during some mandibular movements like protrusion and retrusion. This activation does not cause the movements directly but aids in the expression of an effort to perform them.[8]
Also, there are reports that some small fibers originate from this muscle and insert into the parotid duct (distal portion). These fibers play an active role in regulating the physiological secretion of saliva from the parotid duct.[9]
Embryology
The muscle derives from the second pharyngeal arch or the hyoid arch. It starts to develop along with other facial muscles between 3 and 8 weeks from the laminae formed on each side of the face from pre-myeloblasts and myeloblasts. There are five laminae formed out of which the mandibular lamina creates the buccinator.[10]
Blood Supply and Lymphatics
The main blood supply to the buccinator comes from three arteries which form extensive anastomotic vascular plexus on the muscle's lateral surface and within its fibers. The posterior part of the muscle is supplied by the buccal artery, which is a branch of the internal maxillary artery. The artery runs in an anteroinferior direction under the external pterygoid muscle to reach the posterior part of the muscle. The facial artery, via its numerous branches, supplies the posterior, inferior, and anterior part of the muscle. The posterior buccal branch, which is the largest branch of the facial artery supplies the posterior half of the muscle. Inferior buccal branches of the facial artery supply the inferior half of the muscle. It then runs anterosuperiorly to give off anterior buccal branches which supply the anterior half of the muscle. Two small branches form the posterosuperior alveolar artery, which is a branch of internal maxillary artery enter the buccinator muscle posterosuperiorly and supply the surrounding area.
Venous drainage of the muscle occurs through the pterygoid plexus and internal maxillary vein.
Nerves
The muscle has both motor and sensory innervations. Sensory innervation is by the long buccal nerve, which is a branch of the maxillary division of the fifth cranial nerve. Motor innervation of the muscle is via the temporal and cervical divisions of the seventh cranial nerve (facial nerve).[11]
Muscles
The fibers of the buccinator muscle have their origin from three areas due to which this muscle has three muscular bundles.[2] Two of the muscular bundles have a bony origin. The maxillary bundle arises from the buccal portion of the alveolar process of maxilla, mandibular bundle arises from the buccal portion of the alveolar process of the mandible, and the longitudinal bundle arises from the pterygomandibular raphe.[1] Raphe connects the posterior fibers of this muscle with the anterior portion of a pharyngeal muscle, i.e., superior constrictor muscle.[1] The fibers of all the three bundles run in the anterior direction and descent through the modiolus thus, forming the musculature of the cheek.[3] They insert and blend with fibers of orbicularis oris muscle. Fibers of maxillary bundle blend with fibers of orbicularis oris muscle at the mandibular lip, fibers of mandibular bundle run upward at the maxillary lip and fibers of the longitudinal bundle at the oral commissure to insert into the upper and lower lip.[12]
On the lateral aspect, this muscle is related to the ramus of mandible, muscle of mastication (masseter and medial pterygoid muscle), the buccal fat pad, and the buccopharyngeal fascia. On the medial aspect, its covering is the submucosa and mucosa of the cheek.
The buccinator muscle is pierced by the parotid duct (Stenson's duct) after it crosses the masseter muscle and turns medially at the anterior border of the muscle to open in the oral cavity into a small papilla opposite the maxillary second molar.
Physiologic Variants
The crestal attachment of buccinator muscle, although a rare phenomenon, may lead to difficulty in routine oral functions and restoring the edentulous area.
Surgical Considerations
As the parotid duct pierces the buccinator muscle, it should be identified and preserved during surgery such as while raising buccinators flap. Small to moderate-sized defects of the oral cavity can have reconstruction with the buccinator flap, which is easy and quick to raise. It replaces mucosa with mucosa and correlates with a very low degree of morbidity of the donor site. It is remarkably elastic, thus can be stretched easily to conform to defects with a complex shape.
Clinical Significance
Hyperactivity of the buccinators muscle can cause excessive pressure on the underlying hard tissues resulting in narrow arches and malocclusion.[13][14]
Damage to the facial nerve can lead to paralysis of the buccinator muscles, which can lead to difficult mastication as the non-functioning of this muscle can cause repeated laceration of the cheek mucosa.
Abnormal attachment of this muscle may interfere with the proper prosthodontic management and in maintaining oral hygiene. It will also restrict the cheek and lip movement leading to difficulty in mastication and phonation.
The muscle has been shown to have an indirect involvement during parafunctional movements.
Clinical implication in Prosthodontics:
In the oral cavity, inward forces by the orbicularis oris and the buccinator muscle get balanced by the outward forces of the tongue. While making an impression for a completely edentulous patient, molding must be done by muscle function in such a manner that it is in harmony with the surrounding musculature.
Buccinator along with orbicularis oris and pharyngeal constrictor forms a functional unit (buccinator mechanism) which is essential for orofacial functions (swallowing, sucking, whistling, chewing, vowel pronunciation). If buccinator is weakened or paralyzed, food tends to accumulate in the vestibule during chewing.
Buccinator muscle plays a role in stabilizing the denture by gripping the polished surface of the denture. Also, the longitudinal fibers hold the bolus of food between the teeth during mastication. The maxillary bundle of this muscle tends to raise the upper denture, whereas the mandibular bundle of this muscle depresses the lower denture, thus aiding in denture stability and retention.
Other Issues
The fascial spaces confine early infection, but since the spaces communicate with each other, as the infection progresses, the inflammation can involve the other spaces. The buccal space is the fascial space limited superomedially and inferomedially by fibers of the buccinator muscle originating from alveolar processes of maxilla and mandible. Thus, the roots of the posterior teeth are related to this space. Any infection in the parotid may extend to the buccal space and vice versa.[15]
(Click Image to Enlarge)
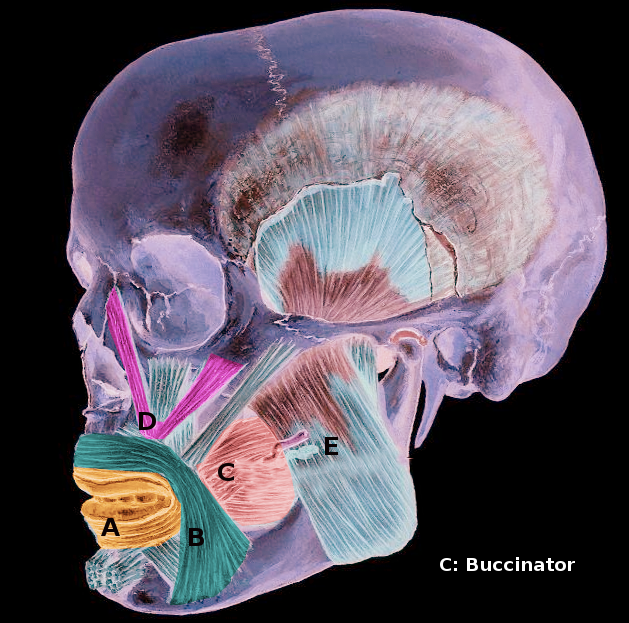
Buccinator muscle
Image courtesy O. Chaigasame