Carotid Artery Stenosis
- Article Author:
- Erion Qaja
- Article Author:
- Prasanna Tadi
- Article Editor:
- Pramod Theetha Kariyanna
- Updated:
- 7/8/2020 8:45:10 AM
- For CME on this topic:
- Carotid Artery Stenosis CME
- PubMed Link:
- Carotid Artery Stenosis
Introduction
Determining the difference between hemodynamic and embolic stroke in the presence of chronic internal carotid artery occlusion is important. Embolic symptoms may be from classic stroke or transient ischemic attack (TIA). Symptoms may include a contralateral motor or sensory deficits as well as amaurosis fugax. Hemodynamic symptoms may be similar to a classic stroke or TIA, but may also be less predictable and atypical. Patients have reported symptoms such as limb shaking, retinal claudication, headache from large pulsatile external carotid artery collaterals, syncope, and generalized fatigue. One-third of all strokes are related to cervical carotid disease. Standard risk factors for coronary and systemic atherosclerosis such as age, male sex, family history, smoking, hypertension, hyperlipidemia, sedentary lifestyle, and high dietary fat apply to this patient population. The mechanism of cervical carotid stroke is usually embolization from the carotid bifurcation plaque, but hemodynamic compromise from stenosis may also play a role. The risks of embolization and hemodynamic compromise increase with increasing carotid artery stenosis.[1][2][2][3]
Etiology
Carotid artery stenosis is a consequence of systemic atherosclerotic disease. Thus, any risk factor predisposing a patient to progressive atherosclerosis can potentially manifest itself as stenosis of the carotid artery with resultant ischemic stroke and or TIA like symptoms. Risks include smoking, hyperlipidemia, male gender, and age.[4][5][6][7]
In a minority of patients, especially young females with stenosis of the carotid artery, fibromuscular dysplasia (FMD) plays a much more significant role. Fibromuscular dysplasia is a noninflammatory, nonatherosclerotic process affecting the carotid and renal arteries, although it can occur elsewhere in medium-sized vessels. Fibromuscular dysplasia usually occurs in the mid and distal internal carotid artery, sometimes extending into the intracranial region. Aneurysms may also be a component of the disease process.
Epidemiology
Symptomatic internal carotid artery occlusion has an incidence of six per 100,000, though the rate of asymptomatic chronic occlusion is unknown and may be higher. Internal carotid artery occlusion is a known risk factor for stroke in the United States. One-third of all the strokes are related to carotid occlusive disease. Stroke ranks third among all causes of death in the United States, behind heart disease and cancer. Annually about 55,000 more women are affected compared with men, and approximately 60% of all stroke deaths occur in females. African Americans and Mexican Americans have a higher risk of stroke compared with Caucasians. Thus diagnosis, prevention, and treatment of the carotid artery stenosis play a pivotal role in stroke prevention.
Pathophysiology
Total internal carotid artery occlusion results from thrombosis in the setting of chronic stenosis. Cardiogenic embolization to a normal carotid bifurcation or carotid dissection may also cause total occlusion of the internal carotid artery occlusion. Acute occlusion may result in a carotid territory stroke. A previously asymptomatic chronic internal carotid artery occlusion may become symptomatic if related to embolic or hemodynamic issues. Embolism may occur from the ipsilateral external carotid artery via collaterals to the cerebral circulation. It may also happen when there is occult patency of the occluded internal carotid artery occlusion, which then serves as the source of embolic material. Hemodynamic insufficiency may occur when any condition that interferes with cerebral perfusions such as orthostasis, hypotension, volume depletion, or cardiac failure is superimposed on the carotid occlusion, especially when the contralateral carotid disease is significant.
History and Physical
Usually, patients will present with recent stroke (slurred speech, cranial nerve deficits, limb weakness, or visual disturbances), which either have resolved or should be expected to improve within 48 hours, otherwise known as a transient ischemic attack. Typically, history and physical examination are notable for a patient in their 70s and 80s because they may have a history of smoking, high lipid profile, sedentary lifestyle. It is imperative to realize that carotid artery atherosclerotic disease is not a segmental disease; rather it has the propensity to involve other arteries in the human body. Of concern are the coronary arteries. Hence, it is prudent for this patient to undergo a cardiac evaluation should surgical intervention be contemplated in treating the degree of stenosis.
Evaluation
Evaluation should include but not be limited to a thorough physical examination. The physical should be coupled with diagnostic imaging (computed tomography scan of the head), followed by telemetry floor admission, as only a third of ischemic strokes are due to carotid artery disease. The remaining is due to the cardiac embolic phenomenon. Thus, consultation with a stroke specialist like a neurologist, as well as a cardiologist, is of paramount importance.
Regarding diagnosing carotid artery stenosis, one usually starts with the least invasive, inexpensive test, such as Carotid Duplex. This examination typically shows a high-resistance signal in the carotid bulb and the very proximal internal carotid artery. Distally, there are no Doppler signals audible in the carotid artery. As a confirmatory test, some form of contrast examination such as digital subtraction arteriography, magnetic resonance arteriography (MRA), or computed tomographic (CT) arteriography is required to confirm the diagnosis and plan a surgical approach. Gadolinium-enhanced MRA is better for differentiating high-grade stenosis than the time of flight which overestimates the stenosis in some times. Conventional angiography is the gold standard for the diagnosis.
Treatment / Management
Acute symptomatic carotid occlusion should be treated with urgent revascularization in select cases with an immediate presentation. This can be accomplished with carotid endarterectomy (CEA) or interventional techniques, including thrombolysis. In the setting of chronic total internal carotid artery occlusion (ICA) occlusion, medical management is preferred over revascularization. However, several special clinical indications exist for procedural intervention. Ipsilateral hemodynamic symptoms in the setting of ipsilateral ICA occlusion and contralateral ICA stenosis may benefit from contralateral ICA revascularization to ameliorate hemodynamic insufficiency. Ipsilateral embolic symptoms in the setting of ipsilateral ICA occlusion and ipsilateral external carotid occlusion (ECA) stenosis may be treated with ipsilateral ECA revascularization to eliminate the source of embolization, which occurs via enlarged ECA collaterals; ligation of the ipsilateral ICA also eliminates a source for embolization. Finally, ipsilateral hemodynamic symptoms in the setting of a patent contralateral carotid system, ipsilateral ICA occlusion, and ipsilateral ECA stenosis indicate ipsilateral ECA revascularization to improve ipsilateral hemodynamic flow.[8][9][10][11]
For patients with symptomatic carotid occlusion (50-99%), if carotid endarterectomy was done within two weeks of symptoms, the number needed to treat for preventing one stroke is 5. The number needed to treat increases to 125 if it has done more than two weeks of symptoms of stroke onset. CEA is beneficial if the symptoms are non-disabling, with no tandem stenoses, high-grade stenosis. CEA can be deferred if the stroke is too big, contralateral carotid occlusion, hemodynamic instability, and contralateral laryngeal palsy is a relative contraindication. There is more myocardial infarction associated with CEA.
Carotid artery stenting (CAS) is preferred in symptomatic carotid occlusion (50-99%) with multiple comorbidities, tracheostomy, patients with prior neck radiation, or dissection. Usually, there is an increased risk of stroke after the CAS. Due to the advancement of the stents and technique, CAS is comparable to CEA in most instances. Carotid revascularization for primary prevention of stroke (CREST-2) study is ongoing and will shed more light on this important area.
Differential Diagnosis
The differential diagnosis of carotid artery stenosis may include:
Pearls and Other Issues
There are no specific criteria for surveillance of patients with chronically occluded ICA, nor are there criteria to specify the degree of ECA stenosis by duplex ultrasound. A reasonable regimen is to follow the patient clinically every six months to a year, with or without a duplex study. The development of symptoms indicates investigation with imaging of some kind to see if cerebrovascular revascularization is indicated.
Enhancing Healthcare Team Outcomes
The management of patients with carotid artery stenosis is with an interprofessional team that consists of a nurse practitioner, primary care provider, internist, vascular surgeon, an interventional radiologist, and a neurologist. When a patient is discovered to have carotid stenosis, a referral should be made to the neurologist who can determine if treatment is required. Today, the carotid stenosis can be managed via surgery or stenting; both have similar outcomes in the short term. The treatment also dramatically reduces the risk of a future stroke.[17]
(Click Image to Enlarge)
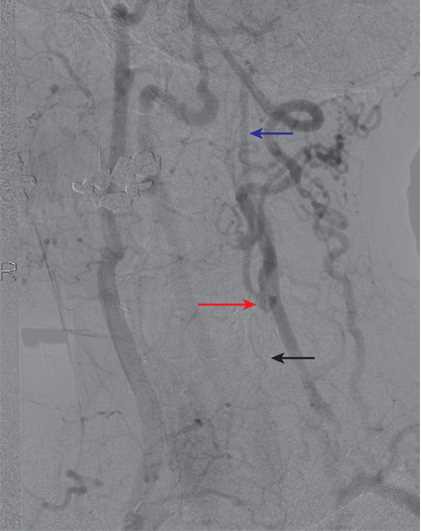
An example of collateralization in a patient with left common carotid artery (CCA) occlusion. The left CCA is occluded (black arrow). There is filling of the left external carotid artery (ECA) via collaterals, and the left carotid bifurcation fills via the ECA (red arrow). The distal left internal carotid artery (ICA) then fills antegrade (blue arrow).
Contributed by Scott Dulebohn, MD