Anatomy, Head and Neck, Cervical Nerves
- Article Author:
- Joshua Waxenbaum
- Article Author:
- Vamsi Reddy
- Article Editor:
- Bruno Bordoni
- Updated:
- 7/27/2020 12:12:21 PM
- For CME on this topic:
- Anatomy, Head and Neck, Cervical Nerves CME
- PubMed Link:
- Anatomy, Head and Neck, Cervical Nerves
Introduction
Cervical nerves are spinal nerves that arise from the cervical region of the spinal cord. These nerves conduct motor and sensory information via efferent and afferent fibers, respectively, to and from the central nervous system. While classified as peripheral nerves, the motor cell body resides in the anterior horn of the spinal cord. There are eight pairs of cervical nerves, denoted C1 to C8, that emerge from the spinal cord superior to their corresponding vertebrae, except for C8 that exits inferiorly to the C7 vertebra. These nerves intertwine through plexuses that give rise to peripheral nerves that maintain a significant motor function in the head, neck, upper limbs, and diaphragm, as well as sensation in the head, neck, shoulders, and upper limbs in a dermatomal pattern.[1][2][3]
Structure and Function
The cervical nerves arise from the spinal cord in the form of rootlets, or fila radicularia, smaller neuron bundles that coalesce to form roots. For each spinal nerve, an anterior and posterior root join to form the completed nerve.[4] Shortly after branching out of the spinal cord, the cervical nerves form the cervical and brachial plexuses. It is important to note that the inputs and outputs may vary by individual, and therefore, different sources may offer different descriptions.[2][5][6]
The cervical plexus forms from the ventral rami of C1 to C4. It is known to anastomose with the facial nerve, hypoglossal nerve, spinal accessory nerve, vagus nerve, and the sympathetic trunk. It lies anteromedial to the scalenes, but is deep to the sternocleidomastoid,[7] and gives rise to the motor and sensory branches:
Motor
- The C1 spinal nerve gives rise to the nerve to the geniohyoid and the nerve to the thyrohyoid that both function in the oropharynx. Anatomically, these nerves travel closely to the hypoglossal nerve (CN XII).[8]
- The ansa cervicalis (“handle of the neck” in Latin), is a loop of nerves that lies superficial to the internal jugular vein, composed of the C1 to C3 nerves. More specifically, one end of the loop, the superior root, is derived from C1 (and possibly C2, depending on the literature), while the other, the inferior root, comes from C2 and C3. This structure gives rise to the nerves to the sternohyoid, sternothyroid, and superior and inferior bellies of the omohyoid muscles.[9] All of the muscles supplied by branches of the ansa cervicalis, along with the thyrohyoid, are infrahyoid muscles, and therefore serve to depress the hyoid bone. This function is necessary for proper speech and swallowing.[10]
- The C3, C4, and C5 roots contribute to form the phrenic nerves. These are responsible for motor and sensory supply to the diaphragm, as well as for sympathetic output. The phrenic nerves run anteriorly to the subclavian arteries, but posterior to the subclavian veins.[7]
- Outside of the cervical plexus, the several muscles are innervated directly by upper cervical nerve roots[11][12][13]:
- C1 to C2: Rectus capitis anterior/lateralis
- C1 to C3/4/5: Longus capitis
- C2/3 to C4: Trapezius (sensory)
Sensory
- The cutaneous branches of the cervical plexus transmit sensory information from the skin of the neck, the superior portions of the thorax, and the scalp.[7] These nerves emerge from a common point at the posterior aspect of the sternocleidomastoid, known as Erb’s point.[14] There are several branches:
- The lesser occipital nerve arises from C2 and supplies the skin of the neck and the scalp posterior and superior to the auricle.
- The greater auricular nerve of C2 and C3 ascends anterior to the auricle and supplies the skin over the parotid gland, the mastoid process, and the skin from the parotid gland to the mastoid process.
- The transverse cervical nerve, of C2 and C3, projects posteriorly and wraps around anteriorly to supply the skin of the anterior cervical region.
- The supraclavicular nerve, of C3 and C4, descends from the posterior sternocleidomastoid and provides sensory information from the skin over the clavicle and shoulder.[1][7]
Sympathetics
- The ventral rami that compose the cervical plexus each receive gray rami communicates from the superior cervical ganglion of the sympathetic trunk.[15][16]
The brachial plexus forms from the ventral rami of C5 to C8, as well as T1. The plexus projects laterally, anterior to the first rib, but posterior to the clavicle, into the axillary region. The plexus is divided into several sections through its several anastomoses from the five nerve roots into three trunks, six divisions, three cords, and finally, five branches.[17] The final outputs are best described by the location from which they emerge from the plexus, rather than simply based on their motor/sensory function as several nerves carry both types of information [2][5][6][18]:
- Roots
- The C4 and C5 roots give rise to the dorsal scapular nerve that supplies the rhomboids and levator scapulae.
- C5, as mentioned earlier, along with C3 and C4, contributes to the phrenic nerve that innervates the diaphragm.
- Roots C5, C6, and C7 produce the long thoracic nerve, responsible for controlling the serratus anterior.
- Trunks
- From the upper trunk C5 and C6 give rise to the nerve to the subclavius, and the suprascapular nerve, that supply the subclavius muscle, and the supra- and infraspinatus muscles, respectively.
- Cords
- From the lateral cord, C5, C6, and C7 supply the pectoralis major and minor muscles, via the lateral and medial pectoral nerves, as well as the coracobrachialis, brachialis and biceps brachii, via the musculocutaneous nerve. The musculocutaneous nerve provides sensation to the skin of the lateral forearm.
- These three roots also form the lateral root of the median nerve that controls most forearm flexors, except flexor carpi ulnaris and the medial portion of flexor digitorum profundus, the first and second lumbricals and the muscles of the thenar eminence. This nerve also provides sensation to the palmar aspect of the thumb, index finger, middle finger, and the lateral aspect of the fourth digit.
- The posterior cord has five outputs:
- From C5 and C6, the upper and lower subscapular nerves supply the upper and lower portions of the subscapularis. The lower subscapular nerve also innervates the teres major.
- Additionally, from C5 and C6, the axillary nerve supplies the motor function of the deltoid and teres minor, as well as the sensory aspect of the overlying skin, the superior lateral cutaneous nerve of the arm, and the skin of the lateral shoulder and arm.
- The thoracodorsal nerve originates from C6, C7, and C8, and innervates the latissimus dorsi.
- Lastly, the radial nerve, which derives from all five roots of the brachial plexus, is responsible for the motor innervation of the triceps brachii, the supinator, the anconeus, the brachioradialis, and all extensor muscles of the forearm. It also supplies the skin of the posterior arm, posterior hand, and the webbing between the thumb and index finger.
- The medial cord also produces five outputs, all of which derive from C8 and T1:
- The medial pectoral nerve, which supplies pectoralis minor and part of the pectoralis major
- The medial root of the median nerve (see the lateral root for details)
- The medial cutaneous nerves of the arm and forearm are purely sensory and supply the medial skin of arm and forearm, respectively.
- Lastly, is the ulnar nerve, which provides motor control to the flexor carpi ulnaris, the medial belly of flexor digitorum profundus, the two medial lumbricals, the interossei, and the muscles of the hypothenar eminence. It also provides sensation to the fifth digit, the hypothenar eminence, and the medial half of the fourth finger.
- Branches
- Musculocutaneous nerve
- Axillary nerve
- Radial nerve
- Median nerve
- Ulnar nerve
For more detailed coverage of the structure of the brachial plexus, see the associated StatPearls articles referenced.[19][20]
Embryology
Spinal nerves originate from the sclerotome, more specifically, the central region of the anterior-half-sclerotome. This portion of the sclerotome is also responsible for the endoneurium and perineurium of the spinal nerves. This origin stands in contrast to the posterior-half-sclerotome that forms the bone and cartilage of the vertebral column. The posterior half also acts to block the outgrowth of neural crest cells and spinal nerve axons, thus leading to the segmentation of the spinal nerves.[21]
Blood Supply and Lymphatics
The roots of spinal nerves receive vascular supply from the radicular arteries. These arteries pass through the intervertebral foramina with the nerve roots. The first six vessels most commonly arise from the vertebral arteries or the ascending cervical branch of the thyrocervical trunk. In either case, the spinal branches of these two vessels anastomose, so if either source has a blockage, blood flow is maintained. The radicular arteries of the seventh and eighth segments always form from branches of the costocervical trunk.[22]
Muscles
The Cervical Nerves innervate numerous muscular structures. The C1 spinal nerve gives rise to the nerve to the geniohyoid and the nerve to the thyrohyoid that both function in the oropharynx. Anatomically, these nerves travel closely to the hypoglossal nerve (CN XII).[8] The ansa cervicalis (“handle of the neck” in Latin), is a loop of nerves that lies superficial to the internal jugular vein, composed of the C1 to C3 nerves. More specifically, one end of the loop, the superior root, is derived from C1 (and possibly C2, depending on the literature), while the other, the inferior root, comes from C2 and C3. This structure gives rise to the nerves to the sternohyoid, sternothyroid, and superior and inferior bellies of the omohyoid muscles.[9] All of the muscles supplied by branches of the ansa cervicalis, along with the thyrohyoid, are infrahyoid muscles, and therefore serve to depress the hyoid bone. This function is necessary for proper speech and swallowing.[10] The C3, C4, and C5 roots contribute to form the phrenic nerves. These are responsible for motor and sensory supply to the diaphragm, as well as for sympathetic output. The phrenic nerves run anteriorly to the subclavian arteries, but posterior to the subclavian veins.[7] Outside of the cervical plexus, the several muscles are innervated directly by upper cervical nerve roots[11][12][13]: C1 to C2: rectus capitis anterior/lateralis; C1 to C3/4/5: longus capitis; C2/3 to C4: trapezius (sensory)
Physiologic Variants
There are numerous variants of cervical nerves and their derivatives that can present in a patient. Specifically, the cervical nerves that contribute to the cervical and brachial plexuses vary between individuals to a significant degree. Moreover, the terminal nerves that branch off the cervical and brachial plexuses may vary in contribution and location of origin.[18]
Surgical Considerations
Cervical nerve pathologies include radiculopathy, which is caused most commonly by impingement by spondylosis or disk herniation. This topic is covered in depth by the StatPearls article referenced here.[23] Surgery should be a consideration if patients present with any neurological deficit as well as after confirming the ability to approach on MRI, prior surgeries, and any comorbid conditions.
Clinical Significance
The most common pathology associated with cervical nerves, radiculopathy, is caused most commonly by impingement by spondylosis or disk herniation. This topic is covered in depth by the StatPearls article referenced here.[23] For more information on the specifics of brachial plexus injuries, as well as other cervical nerve-related pathologies, see the associated StatPearls articles.[24]
(Click Image to Enlarge)
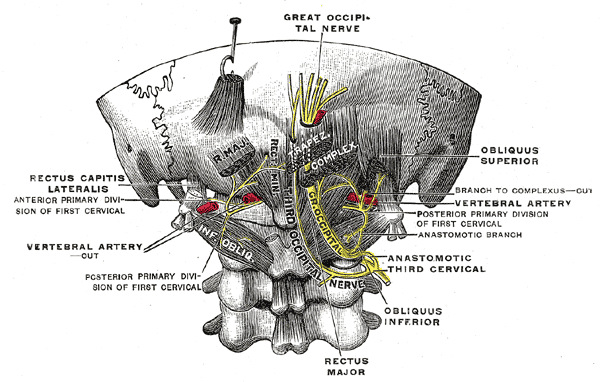
The Posterior Divisions, Posterior primary divisions of the upper three cervical nerves, Great Occipital Nerve
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)

Cervical plexus. Includes ansa cervicalis.
Contributed by Henry Vandyke Carter [Public domain]